Background
California encephalitis is a relatively common, reportable, childhood central nervous system (CNS) disease transmitted by mosquito bites. California serogroup viral encephalitis/meningitis includes infections with the following viruses: La Crosse, Jamestown Canyon, snowshoe hare, trivittatus, Keystone, and California encephalitis viruses.
La Crosse virus is the most common cause of disease in the California encephalitis group. It is second in importance to West Nile viral encephalitis [16] among the mosquito-borne viral diseases in the United States, with about 68 cases reported yearly.
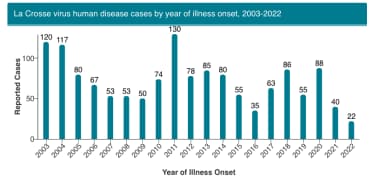 La Crosse virus human disease cases by year of illness onset, 2003-2022. Courtesy of CDC and ArboNET (https://www.cdc.gov/lac/statistics/historic-data.html).
La Crosse virus human disease cases by year of illness onset, 2003-2022. Courtesy of CDC and ArboNET (https://www.cdc.gov/lac/statistics/historic-data.html).
The condition was named California encephalitis after the first human case was described in Kern County, California, in 1946, [1] even though cases in the United States rarely are from California or the West Coast.
Since first described, most cases of California virus disease have been associated with La Crosse virus, [14] a closely related virus to CE virus.
Most infections due to California encephalitis virus group are asymptomatic, and the majority of infected individuals who develop symptoms recover completely; however, up to 10% of patients develop behavioral problems or recurrent seizures. Severe disease often manifests as encephalitis (inflammation of the brain) and can cause seizures, coma, and paralysis. Mortality rates are low (< 1%).
Etiology
California encephalitis disease is caused by a group of viruses that belong to the genus Orthobunyavirus and the family Peribunyaviridae. This largest family of RNA viruses has more than 350 named isolates with worldwide distribution. Peribunyaviridae are spherical, lipid membrane–enclosed viruses that are 90-110 nm in diameter. They contain 3 negative-sense RNA segments and an enveloped nucleocapsid. The nucleocapsid protein is believed to be immunogenic.
La Crosse virus is the main virus in the California serogroup. La Crosse and Jamestown Canyon viruses more commonly cause human diseases. Other rare viruses in the California serogroup virus include California encephalitis virus, snowshow hare virus, and trivitattus virus.
La Crosse virus was first isolated from the brain of a 4-year-old boy who died of encephalitis in La Crosse County, Wisconsin. La Crosse virus is the most common cause of arboviral-induced pediatric encephalitis in the United States. The principal vector is Aedes triseriatus, a forest-dwelling, tree-hole–breeding mosquito of the north central and northeastern regions of the United States. La Crosse virus is maintained in the mosquito via transovarial transmission supplemented by venereal transmission and amplification during summer by mosquitoes feeding on viremic chipmunks, foxes, squirrels, and woodchucks. [17] During winter, the virus survives in infected mosquito eggs. [2]
Aedes triseriatus and albopictus are important vectors and Aedes japonicus also may be involved in virus maintenance and transmission. Alternating cycles of infection occur between the mosquito and the vertebrate hosts, including humans. The mosquitoes obtain the virus after a blood meal from hosts who are in the viremia stage.
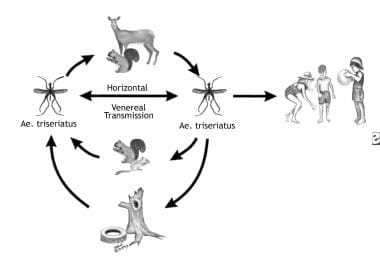 La Crosse virus transmission cycle. The virus is maintained by vertical transmission in Aedes triseriatus mosquitoes; the virus winters in infected eggs that are usually deposited in tree holes or in artificial containers holding rainwater. Horizontal transmission (by viral amplification in small vertebrates, eg, squirrels and chipmunks, and venereally among adult mosquitoes) is required to supplement vertical transmission. The role of deer in viral amplification is uncertain. Human infections are incidental to the transmission cycle.
La Crosse virus transmission cycle. The virus is maintained by vertical transmission in Aedes triseriatus mosquitoes; the virus winters in infected eggs that are usually deposited in tree holes or in artificial containers holding rainwater. Horizontal transmission (by viral amplification in small vertebrates, eg, squirrels and chipmunks, and venereally among adult mosquitoes) is required to supplement vertical transmission. The role of deer in viral amplification is uncertain. Human infections are incidental to the transmission cycle.
After inoculation via a mosquito bite (usually the female mosquito), the virus undergoes a local replication at the original skin site. A primary viremia occurs, with seeding of the reticuloendothelial system, mainly the liver, spleen, and lymph nodes.
With continued virus replication, a secondary viremia occurs, with seeding of the CNS. The probability of CNS infection depends on the efficiency of viral replication at the extraneural sites and the degree of viremia. The virus invades the CNS through either the cerebral capillary endothelial cells or the choroid plexus. Rarely, the virus is isolated from brain tissue.
Antibodies against the G1 part of the virus neutralize the virus, block fusion, and inhibit hemagglutination. They also are important in virus clearance and recovery and in prevention of reinfection.
Epidemiology
Several epidemiologic factors influence arboviral encephalitis, including (1) the season of the year , (2) the geographic location, (3) the regional climate conditions (eg, spring rainfall), and (4) patient age.
The highest incidence of La Crosse neuroinvasive disease in the United States is in the upper midwestern states (Ohio, Minnesota, Wisconsin, Illinois, Iowa, and Indiana). Most cases occur in the late spring to early fall, although, in subtropical endemic areas (eg, the Gulf States), some cases occur in winter as long as mosquito activity is high. Outdoor activities, especially in woodland areas, are associated with an increased risk of infection.
Historically, La Crosse encephalitis has been reported in 24 states, mostly from the northern midwestern states (Minnesota, Wisconsin, Iowa, Illinois, Indiana, and Ohio). Recently, more cases have been reported from mid-Atlantic, southeastern, and northeastern states (West Virginia, Virginia, Kentucky, Georgia, North Carolina, and Tennessee).
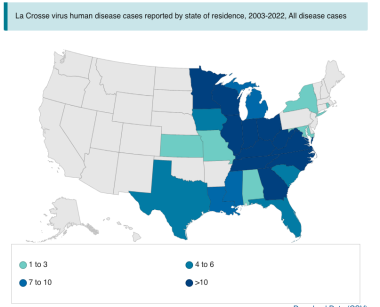 La Crosse virus human and non-human activity by county of residence, 2003-2022. Courtesy of CDC and ArboNET (https://www.cdc.gov/lac/statistics/historic-data.html).
La Crosse virus human and non-human activity by county of residence, 2003-2022. Courtesy of CDC and ArboNET (https://www.cdc.gov/lac/statistics/historic-data.html).
La Crosse virus is more common in males than in females, probably because of more outdoor exposure. Clinical disease occurs almost exclusively in children aged 6 months to 16 years (peak, 4-10 y). The older the patient, the less likely they are to develop the clinical illness. It may be underrecognized in terms of its prevalence and severity.
Patient Education
For patient education information, see the Brain and Nervous System Center, as well as Encephalitis.
-
La Crosse virus transmission cycle. The virus is maintained by vertical transmission in Aedes triseriatus mosquitoes; the virus winters in infected eggs that are usually deposited in tree holes or in artificial containers holding rainwater. Horizontal transmission (by viral amplification in small vertebrates, eg, squirrels and chipmunks, and venereally among adult mosquitoes) is required to supplement vertical transmission. The role of deer in viral amplification is uncertain. Human infections are incidental to the transmission cycle.
-
Brain biopsy specimen from a 7-year-old boy with severe La Crosse encephalitis (hematoxylin and eosin stain, 200X). Perivascular infiltration with mononuclear cells is present on light microscopy. This biopsy material tested positively for La Crosse virus antigen on direct immunofluorescence assay.
-
Left image of a CT scan of an 8-year-old boy with severe La Crosse encephalitis complicated by uncal herniation (obtained on the second hospital day) reveals brain edema with associated obliteration of perimesencephalic cisterns (arrows). On the right, a T2-weighted magnetic resonance image obtained from a 7-year-old boy with severe La Crosse encephalitis shows focal areas of increased signal intensity in the right temporoparietal and left frontotemporal regions (arrows).
-
La Crosse virus neuroinvasive disease cases reported in the United states from 2010-2019. Courtesy of CDC and ArboNET (https://www.cdc.gov/lac/tech/epi.html).
-
La Crosse virus neuroinvasive disease cases reported by state, 2010-2019. Courtesy of CDC and ArboNET (https://www.cdc.gov/lac/tech/epi.html).
-
La Crosse virus human disease cases by year of illness onset, 2003-2022. Courtesy of CDC and ArboNET (https://www.cdc.gov/lac/statistics/historic-data.html).
-
La Crosse virus human and non-human activity by county of residence, 2003-2022. Courtesy of CDC and ArboNET (https://www.cdc.gov/lac/statistics/historic-data.html).





