Overview
The term breathing-related sleep disorder refers to a spectrum of breathing anomalies ranging from chronic or habitual snoring to upper airway resistance syndrome (UARS) to frank obstructive sleep apnea (OSA) or, in some cases, obesity hypoventilation syndrome (OHS). The American Academy of Sleep Medicine (AASM) identifies several types and subtypes of sleep-related breathing disorders. [1]
In adults, there is a male preponderance of OSA during middle age. [2] In women, menopause, pregnancy, and polycystic ovaries are associated with increased risk. [3] In children, prevalence ranges between 1 and 4 % with habitual snoring prevalence at about 7.45 %. [4] Consequences of untreated sleep apnea can be life altering and include both cardiovascular and neurobehavioral morbidities. In children, growth failure can also occur.
The aim of this article is to increase the reader's awareness of the importance of sleep-disordered breathing in daily practice.
Treatment
General treatment measures for breathing-related sleep disorders include (1) behavior modification aimed at improving sleep hygiene and avoiding additional sleep deprivation, (2) avoidance of supine positioning during sleep, and (3) avoidance of ethanol and sedative medications.
Treatment can require major changes in lifestyle. Appropriate weight management strategies and compliance with either positive airway support or the use of a dental appliance usually represent a lifetime commitment. For this reason, some patients have explored surgical alternatives. (See the images below.)
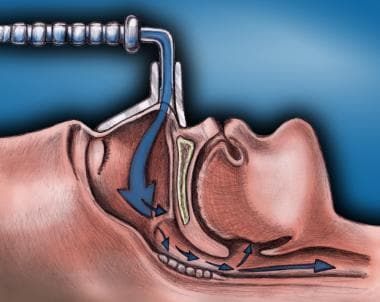 Breathing-related sleep disorder. Lateral cross-section diagram of continuous positive airway pressure (CPAP) system. This system forces air (arrows) through to the lungs in obstructive sleep apnea (OSA) patients.
Breathing-related sleep disorder. Lateral cross-section diagram of continuous positive airway pressure (CPAP) system. This system forces air (arrows) through to the lungs in obstructive sleep apnea (OSA) patients.
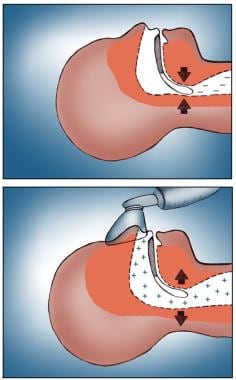 Breathing-related sleep disorder. Before and after the use of a continuous positive airway pressure (CPAP) system. Note that airflow to the lungs is restored with CPAP.
Breathing-related sleep disorder. Before and after the use of a continuous positive airway pressure (CPAP) system. Note that airflow to the lungs is restored with CPAP.
Surgical care
Surgical treatment options for breathing-related sleep disorders include (1) procedures designed to increase upper airway size, (2) procedures designed to bypass the upper airway, and (3) procedures that ensure weight loss. The latter 2 procedures have traditionally been reserved for the more severely affected and recalcitrant patients.
For patients with morbid obesity who are refractory to diet and drug therapy, bariatric surgery has been associated with effective weight loss and significant improvement in sleep-disordered breathing.
Differentials
Differentials to consider in the diagnosis of breathing-related sleep disorders include the following:
-
Depression
-
Gastroesophageal reflux disease
-
Hypothyroidism
-
Obstructive sleep apnea-hypopnea syndrome
-
Congestive heart failure
-
Narcolepsy
-
Nocturnal asthma
-
Daytime sequelae of sleep deprivation, including depression, irritability, poor concentration and memory, and daytime sleepiness
Etiology
Complex interactions among the central and peripheral nervous systems, upper airway musculature, and neurotransmitters may result in partial or complete collapse of a portion or portions of the upper airway. Basic factors such as airway anatomy (eg, adenotonsillar hypertrophy), nasal obstruction, presence and distribution of body fat, and muscle tone may contribute, alone or in combination, to the presence and severity of this disorder. Data suggest that the primary defect is an anatomically small or collapsible pharyngeal airway in combination with a sleep-related fall in upper airway muscular tone.
OSA results from airflow obstruction secondary to upper airway collapse or anatomic airway obstruction. In adults, the obstruction typically occurs at the level of the uvula/soft palate or tongue. The interrelationship of age, sex, obesity, and craniofacial size and dynamics is still poorly understood.
Patients with neuromuscular disease—including Duchenne muscular dystrophy (DMD), amyotrophic lateral sclerosis, postpolio syndrome, and myasthenia gravis—have additional risk factors that may predispose them to sleep-disordered breathing. These include central nervous system (CNS) involvement, chest wall deformity with restrictive lung disease, diaphragmatic weakness, increased upper airway resistance, and impaired respiratory chemosensitivity.
Epidemiology
Occurrence
According to estimates, at least 2–4% of the adult population experience breathing-related sleep disorders. [5, 6] In a study by Young and associates, 24% of men and 9% of women aged 3–60 years were reported to have sleep-disordered breathing. [2]
Obstructive sleep apnea (OSA) may affect as many as 30% of adults and is more common in men than women. [7] The condition is likely underdiagnosed. [8] Caples et al reviewed pooled data from 4 large prevalence studies on OSA and found that 20% of adult Caucasians with a body mass index (BMI) between 25 and 28kg/m2 had an apnea hypopnea index (AHI) of 5 or greater and that approximately 6% of these same patients had AHIs of 15 or greater. [9]
Prevalence studies in the elderly population show significantly higher rates of sleep-disordered breathing, with the rate for elderly men reported as 28–67% and the rate for elderly women as 20-54%. In the subset of patients with severe OSA, men have an 8-fold increased frequency. Prevalence rates in children are estimated to be 5–6%. [3]
Race-, sex-, and age-related demographics
Comparison data between African American and Caucasian adults when corrected for BMI suggest that prevalence of sleep-disordered breathing in African Americans is at least equal to, and may in fact exceed, that of their Caucasian peers.
Male sex appears to be related to a significant increase in the prevalence of sleep-disordered breathing, presumably because of hormonal influences. Testosterone in particular is associated with increased severity of breathing-related sleep disorders. In the subset of patients with severe obstructive sleep apnea, men outnumber women by 8 fold.
Sex hormones play a role in the modulation of upper airway musculature. In adults, the prevalence in males exceeds that of females by 3 fold in middle age. In women with OSA, apneas tend to cluster during rapid eye movement (REM) sleep. In men with OSA, apneas predominate in the supine position.
No sex difference exists before puberty, and after menopause, the differences again become small. The increase in frequency of breathing-related sleep disorders in women who are postmenopausal may be related to decreases in progesterone levels.
In children, those born prematurely have been found to be 3–5 times more likely to have sleep-disordered breathing compared with their full-term counterparts. Childhood OSA has its peak incidence between ages 2–8 years, corresponding to the time when tonsils and adenoids are the largest in relationship to upper airway size. [10] The prevalence for habitual snoring in children is 7.45% and for obstructive sleep apnea, prevalence rates range between 1 and 4%. [11]
Snoring and breathing-related sleep disorders increase in frequency with advancing age, at least until age 60 years. Older persons exhibit central and obstructive apnea. The pattern of apnea in older persons having an AHI of greater than 5 resembles typical sleep apnea with regard to duration and degree of desaturation. However, the effect on general health in elderly people with OSA appears to be minimal.
In elderly people, little to no relationship seems to exist between sleep apnea and typical risk factors such as excess weight and increased airway resistance. The mechanisms underlying sleep apnea in elderly people are purportedly different, and they may reflect a gradual increase in sleep instability, which results in central apnea and OSA.
Morbidity and Mortality
Obesity, [12] advanced age, and snoring have been found to be important factors in the progression of sleep-disordered breathing.
In cases of severe OSA, centers should make every effort to treat patients as soon as possible. Although OSA-related death is rare, a few patients with very severe OSA have died in their sleep soon after being diagnosed with the disease.
Morbidity with OSA falls into 2 major categories: (1) neuropsychiatric or social and (2) cardiovascular.
Neuropsychiatric or psychosocial
This includes excessive daytime sleepiness, poor concentration and memory, decreased performance, irritability, depression, and disturbed social relationships. This population has a significantly increased risk of motor vehicle accidents, with reports of a 7-fold increased risk in patients with an AHI of greater than 5.
Daytime fatigue may affect a person's daytime function and sense of well-being. Depressive symptoms associated with disrupted sleep may require additional intervention after the airway obstruction of OSA has been addressed.
Children with sleep-disordered breathing exhibit increased use of healthcare services (2.6-fold increase), with deficits in school performance and IQ, as well as a higher prevalence of neuropsychiatric disorders. [10]
In a large, population-based, longitudinal study, sleep-disordered breathing symptoms in early life increased the odds of problematic behavior at ages 4 and 7. [13]
Cardiovascular
Untreated OSA may be associated with hypertension and congestive heart failure. Even patients with mild changes in their AHI, with values ranging between 0.1 and 4.9, were found to have an increased risk of developing systemic hypertension when compared with those who had an AHI of 0.
Systemic hypertension occurs in 45-90% of patients with OSA. Pulmonary hypertension has been reported in 15-20%. [14]
Patient Education
Teaching patients to identify breathing-related sleep disorders is important. Chronic snoring, witnessed apnea, and daytime sleepiness warrant further workup.
Education regarding the benefits of good sleep hygiene is beneficial to all patients but has specific importance for patients with breathing-related sleep disorders. Physicians should be alert to the presence of comorbidities.
Daytime sleepiness is associated with poor focus and performance. Patients with OSA and daytime sleepiness should be counseled about their increased risk of having an accident while driving a vehicle or operating heavy machinery.
Patients treated with oral appliances should be educated about good dental hygiene and care of the appliance. Unsupervised, patient-initiated alteration of the oral appliance can be harmful.
For patient education information, see the Ear, Nose, and Throat Center and the Sleep Disorders Center, as well as Snoring, Sleep Disorders and Aging, and Insomnia. Additional patient resources can be found at the National Sleep Foundation.
Physical Examination
General characteristics
Obesity and craniofacial dysmorphology are important features to identify. Micrognathia, retrognathia, maxillary hypoplasia, cleft palate, and macroglossia are among the important initial features to assess. The image below shows a patient with significant retrognathia, which contributed to his OSA.
Mental status
The Mental Status Examination should be tailored to the individual patient, with particular attention to affect because depression is not an uncommon comorbidity in people with sleep deprivation. In patients with neuropsychiatric disease, this evaluation is more extensive.
In addition to insomnia, patients with depressed mood may have a poor appetite, resulting in weight gain or weight loss, fatigue, psychomotor retardation or agitation, difficulty concentrating, or poor memory. Suicidal ideation and actual attempts may occur, especially during the recovery phase.
Blood pressure
Systemic hypertension occurs in approximately 45-90 % of patients with OSA. [14] While diagnostic upper limits may vary somewhat by study site, most agree that hypertension exists when systolic blood pressure is documented repeatedly (ie, on 2 or more visits) as greater than 140mm Hg or when the diastolic value equals or exceeds 90mm Hg on 2 or more visits. Patients with hypertension have an increased incidence of OSA (ie, up to 30% [14] ), and questions about sleep should be included in the workup of patients with hypertension.
Height and weight (BMI)
A BMI greater than 28 is frequently associated with OSA.
Collar (neck) size
Collar size is measured at the level of the cricothyroid membrane and is another parameter associated with predicting risk for OSA. In snoring male patients with collar sizes greater than 17 inches, the prevalence of OSA is 30%. Women with collar sizes greater than 15 inches have also been found to be at increased risk. Neck size was shown to be the strongest predictor of OSA [15] while others have identified it to be an independent risk factor of OSA in adults. [16]
Nasal examination
The nasal examination is critical in identifying potential anatomic sites of obstruction, such as a deviated septum, enlarged adenoids, swollen nasal turbinates, polyps, or other mass lesions. The nasal examination is often conducted using a flexible fiberoptic nasopharyngoscope. In addition to the potential diagnostic value of this procedure, a patent nasopharyngeal airway is necessary if nasal continuous positive airway pressure (n-CPAP) is considered as a treatment option in OSA.
Craniodentofacial examination
In addition to the features described above (eg, retrognathia, micrognathia, macroglossia), mandibular alignment, dental occlusion, and cephalometric data are often helpful.
Oropharynx
A variety of anatomic features can have an impact on airflow limitation at this level, including large tonsils, a long soft palate, a large uvula, a pharyngeal flap, posterior pharyngeal stenosis and scarring, a redundant fold, and tumors. The relationship of the tongue, palate, and posterior pharyngeal wall can cause posterior pharyngeal crowding and predisposition to OSA.
Neck
Fat distribution in this area can compromise airflow during sleep, when muscle tone is reduced, especially during REM sleep. Masses, including significant lymphadenopathy, should be noted.
Lab Tests and Diagnostic Procedures
Clinical scenarios dictate the type and extent of testing beyond the polysomnogram. Clinicians may consider the following tests:
Arterial Blood Gas
Baseline blood gases obtained when the patient is awake provide an indication of ventilatory function and oxygenation. Patients who have chronic obstructive pulmonary disease or chronic interstitial lung disease may have worsening ventilatory function, as well as oxygen desaturation, during sleep.
Pulmonary function testing
Pulmonary function testing (PFT), in the form of prebronchodilator and postbronchodilator spirometry, lung volumes, and diffusing lung capacity for carbon monoxide (DLCO), provides further insight into the presence of underlying lung disease and may raise concerns about nocturnal asthma to explain a patient's symptomatology.
Nasopharyngoscopy with the Müller maneuver
Nasopharyngoscopy is an office procedure used to evaluate the patency of the nasopharyngeal airway. It is generally performed during wakefulness, and the patient often performs a Müller maneuver. In the supine position, the patient inhales against an occluded oronasal airway. The maneuver is performed as an attempt to simulate the pharyngeal collapse that may be occurring during sleep.
Imaging Studies
Imaging studies are generally used in research protocols or in the course of presurgical evaluations, and they should be tailored to address specific questions or concerns. Acoustic reflection is rarely used in clinical practice, because of limited resolution. It is a noninvasive modality designed to enable visualization of upper airway dynamics.
Somnofluoroscopy
This technique has been employed by otolaryngologists to evaluate the area of pharyngeal collapse and maximal airway narrowing during sleep. While this technique has been used to predict surgical success in some patients undergoing uvulopalatopharyngoplasty (UPPP), its use remains limited, especially in patients with obstruction distal to the velopharyngeal region.
Although this is a dynamic study, it does not allow for accurate cross-sectional measurements nor is it sensitive enough to be used to define the contribution of soft tissue dynamics in the upper airway.
Cephalometry
This radiographic technique is used to evaluate the craniofacial skeleton for deficiencies. The airway can be measured in 2 dimensions. Hyoid position seems to be most predictable. However, because the study is performed during wakefulness, it is of limited value.
CT scan of the upper airway
Shepard and associates performed computed tomography (CT) scans of the upper airway in a group of 23 patients before and after UPPP in an attempt to find predictors for surgical success. [17] Cross-sectional areas of the upper airway were analyzed. While UPPP increased the anatomic size of the upper airway in all patients, response defined as decreasing AHI by greater than 50% was observed in only 35%. CT scan alone was not useful in predicting response.
Magnetic resonance imaging
Magnetic resonance imaging (MRI) is the only currently available technique that allows for dynamic imaging of the airway with good resolution of the airway, soft tissues, and fat.
Overnight Polysomnogram
Overnight polysomnogram (PSG) is the gold standard for the diagnosis and characterization of breathing-related sleep disorders. This study measures oral and nasal airflow, respiratory effort, and pulse oximetry, along with a 2-lead electrocardiogram (ECG), leg and chin electromyelogram (EMG), electrooculogram (EOG), and 2-lead electroencephalogram (EEG).
From this data, obstructive apnea (ie, continued muscle activity in the setting of cessation of airflow), central apnea (ie, absent muscle and airflow activity), mixed apnea, and hypopnea (ie, drop in airflow by at least 50% and associated with oxygen desaturation) can be identified and the AHI calculated.
The AHI is a measure that is defined as the total number of apneas and hypopneas divided by the total sleep time in hours. This value plays an important role in defining and grading the severity of sleep-disordered breathing. Not only is the PSG used to define the frequency and duration of the respiratory events; it is also used to evaluate the physiologic consequences of these events; specifically, associated oxygen desaturations, cardiac dysrhythmias, and sleep fragmentation. The image below shows a hypnogram of a patient with severe OSA.
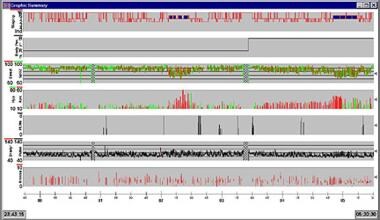 Breathing-related sleep disorder. Hypnogram of patient with severe obstructive sleep apnea (OSA).
Breathing-related sleep disorder. Hypnogram of patient with severe obstructive sleep apnea (OSA).
Weight Loss, Diet, and Activity
The recommendation for weight loss is critical in even mildly obese patients because even small amounts of weight loss may have significant impact on the respiratory disturbance index (RDI), may reduce the degree of oxygen desaturation, and may improve sleep architecture.
Depression and fatigue may hamper weight loss plans, and, at least initially, weight loss may need to be combined with psychotherapy.
Diet
A study by Johansson et al showed that a very-low-energy diet improved OSA after 1 year in obese men with moderate to severe disease. [18] The diet consisted of a standard 2.3MJ/day liquid energy intake protocol (Cambridge Weight Plan; Northants, UK) for 7 weeks. Over the next 2 weeks, the patients gradually returned to a normal food diet of 6.3MJ/day. Patients who lost weight and those with severe cases of sleep apnea showed the most benefit.
Activity
Obese patients with breathing-related sleep disorders should have medical clearance before beginning an exercise program.
Positive Airway Pressure
The following variations of positive pressure support via nasal mask are used at home for the treatment of OSA:
-
n-CPAP - Delivers a constant pressure throughout inspiration and expiration
-
Bilevel positive airway pressure (BiPAP) - Allows independent adjustment of inspiratory and expiratory pressures; this technique provides a lower mean airway pressure, and risk of barotrauma reportedly is decreased, but no improvement in compliance has been observed with BiPAP in comparison with n-CPAP
-
Autotitrating CPAP - Has also been used in the home setting and has the advantage of adjusting to the individual patient's airflow patterns
The most frequently used medical modality for the treatment of OSA is n-CPAP. This technique involves the application of positive pressure to the upper airway via a nasal mask. In this way, n-CPAP is used to stent open the collapsed pharyngeal tissue and improve airflow. Effective delivery pressures are titrated in the sleep laboratory. (See the images below.)
 Breathing-related sleep disorder. A patient using a continuous positive airway pressure (CPAP) system. Courtesy of Jim Matchuny.
Breathing-related sleep disorder. A patient using a continuous positive airway pressure (CPAP) system. Courtesy of Jim Matchuny.
 Breathing-related sleep disorder. A standard continuous positive airway pressure (CPAP) mask. Courtesy of S.R. Dong, MD.
Breathing-related sleep disorder. A standard continuous positive airway pressure (CPAP) mask. Courtesy of S.R. Dong, MD.
 Breathing-related sleep disorder. The Adam Circuit continuous positive airway pressure (CPAP) mask. Courtesy of S.R. Dong, MD.
Breathing-related sleep disorder. The Adam Circuit continuous positive airway pressure (CPAP) mask. Courtesy of S.R. Dong, MD.
 Breathing-related sleep disorder. A gel-filled continuous positive airway pressure (CPAP) mask. Courtesy of S.R. Dong, MD.
Breathing-related sleep disorder. A gel-filled continuous positive airway pressure (CPAP) mask. Courtesy of S.R. Dong, MD.
The technique is noninvasive and highly effective in reducing apnea and improving sleep architecture. However, n-CPAP is often limited by poor patient compliance. Compliance studies showed that 46% of patients used n-CPAP for at least 4 hours per day for 5-7 days. Seventy-six percent of patients overestimated their compliance. The images below show CPAP maintaining upper airway patency during sleep.
Breathing-related sleep disorder. Lateral cross-section diagram of continuous positive airway pressure (CPAP) system. This system forces air (arrows) through to the lungs in obstructive sleep apnea (OSA) patients.
Breathing-related sleep disorder. Before and after the use of a continuous positive airway pressure (CPAP) system. Note that airflow to the lungs is restored with CPAP.
Complications
Possible adverse effects related to this type of nocturnal ventilatory support include those related to pressure, airflow, and the mask-face interface. Therefore, dry mouth, barotrauma, pneumothoraces, and aerophagia, as well as air leaks and pressure sores at the mask interface, may be observed. Sinusitis and dermatitis can also occur with positive airway pressure (PAP) devices. Tinnitus and dyspnea are other possible complications, but they are less frequently seen.
Oral Appliances
Customized dental appliances are designed to increase airway size and to facilitate airflow by advancing the mandible or tongue or lifting the soft palate. While success with oral appliances often is difficult to predict, such devices may offer a valid treatment option in nonobese patients with micrognathia or retrognathia who have mild or mild-to-moderate apnea.
Oral appliances may be categorized into (1) those that advance the tongue, such as the tongue-retaining device (TRD); (2) those that advance the jaw, such as the mandibular advancing device (MAD); and (3) those that simultaneously lift the soft palate and advance the mandible (known as Z appliances). Examples of TRDs are shown below.
 Breathing-related sleep disorder. The tongue-retaining device (TRD) is a dental appliance used for obstructive sleep apnea (OSA). The patient inserts his or her tongue into the bulb at the front of the appliance. Because this device is sealed at the front, the patient must be able to breathe quite well through the nose in order to use it. Courtesy of S.R. Dong, MD.
Breathing-related sleep disorder. The tongue-retaining device (TRD) is a dental appliance used for obstructive sleep apnea (OSA). The patient inserts his or her tongue into the bulb at the front of the appliance. Because this device is sealed at the front, the patient must be able to breathe quite well through the nose in order to use it. Courtesy of S.R. Dong, MD.
 Breathing-related sleep disorder. The tongue-retaining device (TRD) is a dental appliance used for obstructive sleep apnea (OSA). Courtesy of the Sleep Disorders Dental Society.
Breathing-related sleep disorder. The tongue-retaining device (TRD) is a dental appliance used for obstructive sleep apnea (OSA). Courtesy of the Sleep Disorders Dental Society.
 Breathing-related sleep disorder. This dental appliance is used for obstructive sleep apnea (OSA). Its tongue-retaining flange is intended to hold the tongue out of the airway. The patient cannot swallow when using this type of device. Also, the flange can cause obstruction of small upper airways (a common finding in OSA). Courtesy of S.R. Dong, MD.
Breathing-related sleep disorder. This dental appliance is used for obstructive sleep apnea (OSA). Its tongue-retaining flange is intended to hold the tongue out of the airway. The patient cannot swallow when using this type of device. Also, the flange can cause obstruction of small upper airways (a common finding in OSA). Courtesy of S.R. Dong, MD.
Adverse effects of oral appliances may include temporomandibular joint (TMJ) discomfort, excessive salivation, dry mouth, and dental malalignment. In general, patients with severe OSA have had poor results. High cost, poor reimbursement, and patient discomfort have contributed to limiting the use of these devices.
The images below show a Herbst appliance, a mandibular advancing device (MAD) used in the treatment of OSA.
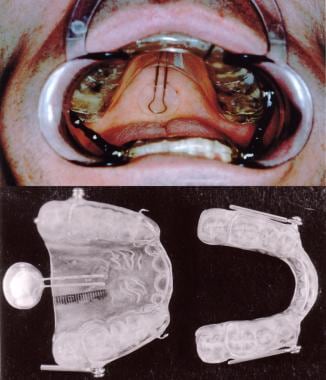
 Breathing-related sleep disorder. The Herbst appliance, a mandibular advancing device (MAD), is a dental appliance used for obstructive sleep apnea (OSA). Herbst is a registered trademark of Dentaurum. Courtesy of Great Lakes Orthodontics, Ltd.
Breathing-related sleep disorder. The Herbst appliance, a mandibular advancing device (MAD), is a dental appliance used for obstructive sleep apnea (OSA). Herbst is a registered trademark of Dentaurum. Courtesy of Great Lakes Orthodontics, Ltd.
 Breathing-related sleep disorder. The Herbst appliance, a mandibular advancing device (MAD), is a dental appliance used for obstructive sleep apnea (OSA). Herbst is a registered trademark of Dentaurum. Courtesy of Orthodontic CYBERjournal.
Breathing-related sleep disorder. The Herbst appliance, a mandibular advancing device (MAD), is a dental appliance used for obstructive sleep apnea (OSA). Herbst is a registered trademark of Dentaurum. Courtesy of Orthodontic CYBERjournal.
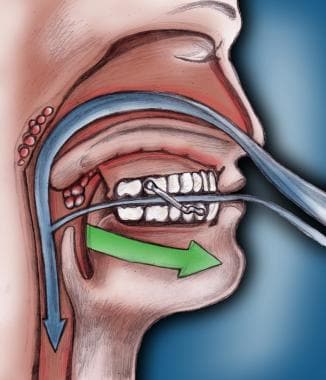 Breathing-related sleep disorder. Lateral, cross-sectional diagram of the Herbst appliance, a mandibular advancing device (MAD), showing its function in reopening the airway in obstructive sleep apnea (OSA). Herbst is a registered trademark of Dentaurum.
Breathing-related sleep disorder. Lateral, cross-sectional diagram of the Herbst appliance, a mandibular advancing device (MAD), showing its function in reopening the airway in obstructive sleep apnea (OSA). Herbst is a registered trademark of Dentaurum.
 Breathing-related sleep disorder. The bonded Herbst appliance, a mandibular advancing device (MAD), is a dental appliance used for obstructive sleep apnea (OSA). Herbst is a registered trademark of Dentaurum. Courtesy of Johns Dental Laboratories.
Breathing-related sleep disorder. The bonded Herbst appliance, a mandibular advancing device (MAD), is a dental appliance used for obstructive sleep apnea (OSA). Herbst is a registered trademark of Dentaurum. Courtesy of Johns Dental Laboratories.
 Breathing-related sleep disorder. The bonded Herbst appliance, a mandibular advancing device (MAD), is a dental appliance used for obstructive sleep apnea (OSA). Herbst is a registered trademark of Dentaurum. Courtesy of Johns Dental Laboratories.
Breathing-related sleep disorder. The bonded Herbst appliance, a mandibular advancing device (MAD), is a dental appliance used for obstructive sleep apnea (OSA). Herbst is a registered trademark of Dentaurum. Courtesy of Johns Dental Laboratories.
The image below shows a customized, original design for a Z appliance, combining features of the Herbst appliance and the TRD.
 Breathing-related sleep disorder. This photograph shows an example of a Z appliance, which is an original design of F. Danziger, DDS, FAGD.
Breathing-related sleep disorder. This photograph shows an example of a Z appliance, which is an original design of F. Danziger, DDS, FAGD.
Surgery To Increase Upper Airway Size
Pediatric patients
The first line and most common procedure done in children with obstructive sleep apnea (OSA) and adenotonsillar hypertrophy who are surgically acceptable candidates is an adenotonsillectomy. High-risk children, including those with obesity or failure to thrive, young age, severe apnea, craniofacial anomalies, or neuromuscular or cardiac disease should be monitored as inpatients. High-risk children should be reevaluated postoperatively for persistent OSA symptoms.
If adenotonsillar hypertrophy is not present, other options may be considered. In those children whose OSA has not resolved or sufficiently improved after surgery and those who are not surgical candidates, CPAP should be considered. [19]
Uvulopalatopharyngoplasty
UPPP is a surgical procedure designed to enlarge the pharyngeal airway dimensions at the level of the soft palate. It involves resection of the uvula and posterior margins of the soft palate, as well as the resection of any redundant nasopharyngeal tissue. It is not indicated in patients with severe OSA.
The overall incidence of complications is low but may include velopharyngeal insufficiency and nasopharyngeal stenosis with worsening apnea.
Maxillomandibular osteotomy and advancement
This procedure is designed to advance the maxilla, mandible, and chin in a patient with dentofacial deformity–related sleep apnea (see the image below). Often, hyoid suspension and genioglossal advancement are performed simultaneously with these surgical procedures.
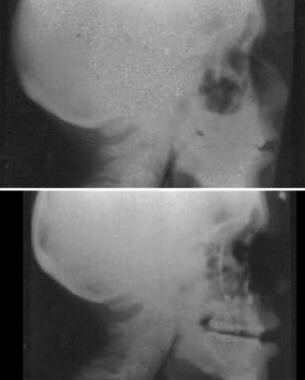 Breathing-related sleep disorder. Preoperative and postoperative radiographs of a patient who underwent jaw advancement surgery. Courtesy of Stephanie Drew, MD.
Breathing-related sleep disorder. Preoperative and postoperative radiographs of a patient who underwent jaw advancement surgery. Courtesy of Stephanie Drew, MD.
Additional techniques
Other techniques in this category include adenotonsillectomy, laser-assisted uvulopalatoplasty, lingual resection, lingualplasty, genioglossal advancement, and hyoid suspension.
Tracheostomy
Tracheostomy is a surgical technique used to bypass the upper airway in order to relieve upper airway obstruction. This option is reserved for the most severe cases because of the very significant psychosocial implications and potential complications of the procedure. In most patients, a rapid response occurs, with return of sleep architecture to normal within the first postoperative month.
Tracheostomy may be considered as a temporary or permanent option in patients with severe oxygen desaturation or cardiac dysrhythmia precipitated by OSA in whom CPAP therapy is refused, poorly tolerated, or unsuccessful and in those patients in whom underlying cardiac, pulmonary, or neuromuscular disease is exacerbated by the severity of the OSA.
Pharmacologic Therapy
Several pharmacotherapeutic options have been explored with regard to stimulating breathing, improving diaphragmatic function, and altering sleep architecture. Studies on these drug options are limited in number and variable in response. With limited exceptions, such treatments are not effective options. Individuals interested in exploring the pharmacologic studies in this area are referred to the paper by Hudgel that reviews the published literature. [20]
Drug categories that have been explored include ventilatory stimulants, such as medroxyprogesterone, which have had limited success in some patients with hypercapnic OSA. Clinical trials with modafinil (a wakefulness-promoting agent) showed some efficacy in patients with OSA, although they continued to have daytime sleepiness in spite of effective treatment.
Follow-Up
Patients with comorbidities (eg, obesity, depression) should receive appropriate evaluation as inpatients, and arrangements should be made for specific follow-up for their respiratory intervention (eg, n-CPAP) and any comorbidities.
In children, follow-up sleep studies are recommended.
Outpatient follow-up is tailored to the individual patient and the interventions selected to address the diagnoses. For example, a patient with obesity, depression, and severe OSA who underwent a tracheostomy requires more intensive follow-up from a therapeutic team than does a healthy young man with mild apnea who required an adenoidectomy or the repair of a deviated nasal septum.
Patients with mild to moderate OSA who are treated with an oral appliance should have regular follow-up with their dentist to be monitored for adherence, to have the device evaluated for deterioration or maladjustment, and to be assessed for signs and symptoms of worsening OSA. In addition, attention to dental hygiene is important. Practice parameters for the use of oral appliances recommend that once optimal fit is obtained, patients should be seen every 6 months for the first year and then annually, unless a problem occurs that requires more urgent assessment and care.
Patients treated with positive airway pressure (PAP) devices are required to have long-term follow-up. The initial follow-up visit is recommended within the first few weeks after the initiation of treatment, to assess compliance and address any concerns. Long-term follow-up is recommended annually or as needed to address compliance and address any concerns about the PAP device or interface.
Consultations
Most of the procedures involved in the diagnosis, evaluation, and treatment of breathing-related sleep disorders involve subspecialty consultations.
Sleep medicine physicians
Sleep medicine physicians are generally affiliated with a sleep disorder center. Their specialty training may come from a variety of sources, but most commonly from pulmonology, neurology, or psychiatry. Additional training in the area of sleep disorders may lead to board certification by the American Board of Sleep Medicine.
Once patients have been identified with OSA, titration of positive pressure ventilation can be achieved under supervision in the sleep laboratory.
Otolaryngologists
Many patients with OSA decide to explore the surgical options to allow complete correction or cure in an effort to avoid a lifetime commitment to n-CPAP or a dental appliance.
Oral surgeons and dentists
The evaluation of patients with dentofacial abnormalities can be greatly assisted by the input of these specialists, who can customize dental appliances and, in special cases, offer additional surgical options for patients.
Psychiatrists
Patients with OSA may have difficulties with the sequelae of chronic sleep deprivation, the need for n-CPAP or surgery, and the prospect of often-significant weight loss. Depression may coexist with chronic sleep deprivation and may require ongoing psychiatric intervention until both are under control.
Pulmonologists
Underlying pulmonary parenchymal or airway disease can influence the severity of the response to OSA. Treatment of such disorders can complement the treatment of OSA.
Cardiologists
Systemic and pulmonary hypertension have been associated with OSA. In such cases, a cardiologist can provide valuable assistance with disease management.
Bariatric surgeons
Bariatric surgery may be considered in morbidly obese patients who have failed to achieve effective weight loss despite diet and drug therapy. In Buchwald's analysis of 136 studies, which included roughly 22,000 patients who underwent bariatric surgery, patients with OSA experienced a significant improvement in oxygen saturation, carbon dioxide (CO2) retention, and arterial oxygen content.
Treatment Concerns
The time between diagnosis and treatment (typically a CPAP titration) of a breathing-related sleep disorder may be extended for various reasons. The most common is scheduling limitations at the sleep center. In addition, the sleep center often serves as a diagnostic facility, leaving the treatment decision to the referring physician.
-
Breathing-related sleep disorder. Significant retrognathia contributed to this patient's obstructive sleep apnea (OSA).
-
Breathing-related sleep disorder. Hypnogram of patient with severe obstructive sleep apnea (OSA).
-
Breathing-related sleep disorder. A patient using a continuous positive airway pressure (CPAP) system. Courtesy of Jim Matchuny.
-
Breathing-related sleep disorder. Lateral cross-section diagram of continuous positive airway pressure (CPAP) system. This system forces air (arrows) through to the lungs in obstructive sleep apnea (OSA) patients.
-
Breathing-related sleep disorder. Before and after the use of a continuous positive airway pressure (CPAP) system. Note that airflow to the lungs is restored with CPAP.
-
Breathing-related sleep disorder. A standard continuous positive airway pressure (CPAP) mask. Courtesy of S.R. Dong, MD.
-
Breathing-related sleep disorder. The Adam Circuit continuous positive airway pressure (CPAP) mask. Courtesy of S.R. Dong, MD.
-
Breathing-related sleep disorder. A gel-filled continuous positive airway pressure (CPAP) mask. Courtesy of S.R. Dong, MD.
-
Breathing-related sleep disorder. The Herbst appliance, a mandibular advancing device (MAD), is a dental appliance used for obstructive sleep apnea (OSA). Herbst is a registered trademark of Dentaurum. Courtesy of Great Lakes Orthodontics, Ltd.
-
Breathing-related sleep disorder. The Herbst appliance, a mandibular advancing device (MAD), is a dental appliance used for obstructive sleep apnea (OSA). Herbst is a registered trademark of Dentaurum. Courtesy of Orthodontic CYBERjournal.
-
Breathing-related sleep disorder. Lateral, cross-sectional diagram of the Herbst appliance, a mandibular advancing device (MAD), showing its function in reopening the airway in obstructive sleep apnea (OSA). Herbst is a registered trademark of Dentaurum.
-
Breathing-related sleep disorder. The bonded Herbst appliance, a mandibular advancing device (MAD), is a dental appliance used for obstructive sleep apnea (OSA). Herbst is a registered trademark of Dentaurum. Courtesy of Johns Dental Laboratories.
-
Breathing-related sleep disorder. The bonded Herbst appliance, a mandibular advancing device (MAD), is a dental appliance used for obstructive sleep apnea (OSA). Herbst is a registered trademark of Dentaurum. Courtesy of Johns Dental Laboratories.
-
Breathing-related sleep disorder. The tongue-retaining device (TRD) is a dental appliance used for obstructive sleep apnea (OSA). Courtesy of the Sleep Disorders Dental Society.
-
Breathing-related sleep disorder. The tongue-retaining device (TRD) is a dental appliance used for obstructive sleep apnea (OSA). The patient inserts his or her tongue into the bulb at the front of the appliance. Because this device is sealed at the front, the patient must be able to breathe quite well through the nose in order to use it. Courtesy of S.R. Dong, MD.
-
Breathing-related sleep disorder. This dental appliance is used for obstructive sleep apnea (OSA). Its tongue-retaining flange is intended to hold the tongue out of the airway. The patient cannot swallow when using this type of device. Also, the flange can cause obstruction of small upper airways (a common finding in OSA). Courtesy of S.R. Dong, MD.
-
Breathing-related sleep disorder. This photograph shows an example of a Z appliance, which is an original design of F. Danziger, DDS, FAGD.
-
Breathing-related sleep disorder. Preoperative and postoperative radiographs of a patient who underwent jaw advancement surgery. Courtesy of Stephanie Drew, MD.
-
Breathing-related sleep disorder. Courtesy of F. Danziger, DDS, FAGD.
Tables

What would you like to print?
- Overview
- Etiology
- Epidemiology
- Morbidity and Mortality
- Patient Education
- Physical Examination
- Lab Tests and Diagnostic Procedures
- Imaging Studies
- Overnight Polysomnogram
- Weight Loss, Diet, and Activity
- Positive Airway Pressure
- Oral Appliances
- Surgery To Increase Upper Airway Size
- Tracheostomy
- Pharmacologic Therapy
- Follow-Up
- Consultations
- Treatment Concerns
- Show All
- Media Gallery
- References