Background
Ureteropelvic junction (UPJ) obstruction is defined as an obstruction of the flow of urine from the renal pelvis to the proximal ureter. The condition is frequently encountered by both adult and pediatric urologists. Congenital abnormalities may be observed in both adults and children, but adults may also present with UPJ obstruction secondary to surgery or other disorders that can cause inflammation of the upper urinary tract.
The critical decision to be made in dealing with suspected UPJ obstruction is whether the radiologic findings correlate with the physiologic picture. In other words, severely dilated hydronephrotic kidneys may, in fact, be found to be draining well when studied appropriately. Defining the exact anatomy and function of these kidneys is crucial when evaluating and treating these patients.
The treatment strategies for UPJ obstruction have shifted significantly in the last several years. The gamut of current surgical treatments for UPJ obstruction includes the following:
-
Laparoscopic pyeloplasty
-
Open pyeloplasty
-
Endopyelotomy
-
Endopyeloplasty
-
Robotic-assisted laparoscopic pyeloplasty
While open pyeloplasty is still considered the criterion standard for treatment of UPJ obstruction in infants, laparoscopic pyeloplasty, with or without robotic assistance, is the treatment of choice in older children and in most adults. [1]
History of the Procedure
UPJ obstruction is the most common cause of neonatal and antenatal hydronephrosis, occurring in one per 1500 live births. Prior to the use of prenatal ultrasonography, most patients with UPJ obstruction presented with pain, hematuria, urosepsis, failure to thrive, or a palpable mass. With the enhanced ability and availability of prenatal ultrasonography, urologic abnormalities are being diagnosed earlier and more frequently. Fifty percent of patients diagnosed with antenatal hydronephrosis are eventually diagnosed with UPJ obstruction upon further workup.
Initially, most children are treated conservatively and monitored closely. Intervention is indicated in the event of significantly impaired kidney drainage or poor kidney growth.
Problem
UPJ obstruction is defined as an obstruction of the flow of urine from the renal pelvis to the proximal ureter. The resultant back pressure within the renal pelvis may lead to progressive renal damage and deterioration.
UPJ obstruction presents most frequently in childhood, but adult and elderly individuals can also present with a primary obstructive lesion. In adults, other etiologies for ureteral obstruction must be considered, including stones, ureteral compression due to extrinsic processes, retroperitoneal fibrosis, and other inflammatory processes.
Epidemiology
Epidemiologic features of UPJ obstruction are as follows:
-
Ultrasonography reveals fetal upper urinary tract dilatation in approximately one in 100 pregnancies; however, only one in 500 of those infants are later diagnosed with significant urologic problems
-
UPJ obstruction is found in approximately 50% of patients diagnosed with antenatal hydronephrosis
-
The male-to-female ratio of UPJ obstruction is 3-4:1
-
In general, the left kidney is more commonly affected than the right kidney
-
UPJ obstruction is less common in adults than in children but is not rare in either population
-
UPJ obstruction is bilateral in 10% of cases
Etiology
Possible etiologies for UPJ obstruction include the following:
-
Intrinsic obstruction may result from stenosis due to scarring of ureteral valves.
-
Ureteral hypoplasia may result in abnormal peristalsis through the UPJ. Asymmetry of ureteral wall musculature may inhibit the natural peristaltic emptying of the renal pelvis into the ureter.
-
An abnormal or high insertion of the ureter into the renal pelvis may alter the configuration and impair drainage of urine. This may be an effect rather than a cause because the two etiologies mentioned above may manifest as a high-insertion variant seen on imaging studies.
-
Crossing lower-pole renal vessel(s) or entrapment of the ureter by a vessel can block urinary flow down the ureter. Vessels that wrap around the UPJ may be associated with obstruction or may be a product of renal dilatation and hydronephrosis that distorts renal vascular architecture.
-
Rotation of the kidney (eg, renal ectopy) and renal hypermobility can cause intermittent obstruction that is solely dependent on the position of the kidney relative to the ureter. This was once a very popular diagnosis; however, the other etiologies mentioned above are more prevalent today, and this cause is particularly rare.
-
Secondary UPJ obstruction can be caused by prior surgical intervention to treat other disorders (eg, renal stone disease) or failed repair of a primary UPJ obstruction. This obstructive lesion is usually secondary to ureteral-wall and periureteral scar formation.
All of the above abnormalities impair drainage of urine from the kidney into the ureter, resulting in elevated intrarenal back pressure, dilatation of the collecting system, and hydronephrosis.
Scanning electron microscopy studies using 3-dimensional techniques have shown that normal elasticity and distension of the renal pelvis are impaired secondary to rigid collagen bundling. Increased collagen deposition between smooth muscle cells results in wider cell-to-cell and nerve-to-cell distances. Neural depletion has also been reported. In addition, immunohistochemical studies have shown decreased neuronal markers and nerve growth factors within the smooth muscle layer, thus impeding peristalsis.
In the rat model, acute obstruction resulted in increased levels of angiotensin 11 and increased transforming growth factor–β expression, resulting in pathological deposition of extracellular matrix, which may be one mechanism that leads to obstruction.
Presentation
Neonates may present with hydronephrosis. Older children may present with urinary tract infection (UTI), a flank mass, or intermittent flank pain secondary to a primary UPJ obstruction. Hematuria may also be a presenting sign if obstruction is associated with infection.
Adults with UPJ obstruction can present with various symptoms, including back and flank pain, UTI, and/or pyelonephritis. A detailed history may reveal that the pain correlates with periods of increased fluid intake or ingestion of a food with diuretic properties (ie, Dietl crisis).
Indications
The goals in treating patients with ureteropelvic junction (UPJ) obstruction are to improve kidney drainage and to maintain or improve kidney function.
As mentioned above, dilatation of the intrarenal collecting system or hydronephrosis does not necessarily imply obstruction. Specifically in children, renal pelvic dilatation should be monitored with serial imaging to assess for changes in dilatation, renal parenchymal thickness and/or the presence of scarring, and function. Surgical repair is indicated upon a significant differential on serial imaging or progressive deterioration of kidney function.
Using this algorithm, patients with hydronephrosis are monitored closely with renal ultrasonography and nuclear medicine renography every 3-6 months. Similarly, in adults, repair is recommended if nuclear medicine renal scan or intravenous pyelography (IVP) reveals ureteral obstruction.
Relevant Anatomy
The evaluation of an obstructed ureteropelvic junction (UPJ) requires information about ureteral and surrounding anatomy, kidney position and ectopy, associated vasculature, and kidney function. Prior to surgical intervention, the surgeon frequently evaluates for kidney position/ectopy, mobility, and UPJ anatomy, such as high-insertion variants versus annular stricture variants.
The major vascular supply of the UPJ comes from branches of the renal artery. These vessels usually lie in an anteromedial location in relation to the proximal ureter. Aberrant polar vessels may also be associated with the renal pelvis, causing compression and obstruction of the collecting system. These vessels arise from either the renal artery from a position proximal to the main intrarenal branching site or directly from the aorta. They can surround the UPJ and can be associated with obstruction, or they may be aberrantly positioned secondary to increasing hydronephrosis.
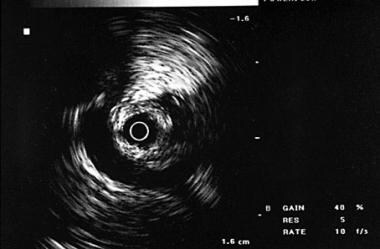 Intraluminal sonogram demonstrating the renal vein surrounding the ureteropelvic junction and causing extrinsic compression and obstruction.
Intraluminal sonogram demonstrating the renal vein surrounding the ureteropelvic junction and causing extrinsic compression and obstruction.
An endopyelotomy refers to an endoscopic incision of the UPJ, performed to create a more funneled drainage system and to bring the UPJ more dependent or caudad below areas of pathology.
The vascular anatomy at the UPJ becomes crucial during an endopyelotomy. The renal collecting system may be accessed percutaneously (antegrade) or in a retrograde fashion via passage of a ureteroscope through the urethra, bladder, and ureter in order to access the obstruction and to perform an incision. While most associated UPJ vessels lie in the anteromedial plane, accessory vessels may lie posteriorly or laterally. If all endoscopic incisions are made in the posterior-lateral plane, intraoperative hemorrhage may occur. For this reason, a comprehensive vascular evaluation with intraoperative endoluminal ultrasonography, preoperative CT scanning, or MRI with vascular reconstruction is recommended prior to this form of treatment.
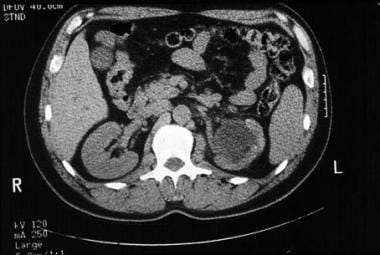 CT scan without contrast demonstrating severe left-sided hydronephrosis secondary to ureteropelvic junction obstruction.
CT scan without contrast demonstrating severe left-sided hydronephrosis secondary to ureteropelvic junction obstruction.
 CT scan with intravenous contrast demonstrating pooling of contrast and delayed excretion of contrast from a left-sided ureteropelvic junction obstruction.
CT scan with intravenous contrast demonstrating pooling of contrast and delayed excretion of contrast from a left-sided ureteropelvic junction obstruction.
Multidetector CT scanning with 3-dimensional reconstruction can be particularly helpful in establishing the anatomy of UPJ obstruction, revealing an intrinsic or high-insertion UPJ. Crossing vessels and their relationship to the ureter of the UPJ can also be evaluated. The location of these vessels and their possible contribution to renal obstruction can help the surgeon decide whether endopyelotomy, open pyeloplasty, or laparoscopic pyeloplasty would be the most effective treatment modality.
When an open or laparoscopic pyeloplasty is performed, an accurate understanding of the vascular anatomy allows the surgeon to preserve the accessory renal vessels and to redirect them if the surgeon feels that they contribute to the obstruction. If an endopyelotomy is planned, this information can guide the surgeon in directing the endopyelotomy incision away from crossing vessels. CT scanning in combination with 3-phase and 3-dimensional contrast imaging yields a reported sensitivity of 75%-97% in revealing crossing vessels. El-Nahas et al reported that CT scanning yielded a sensitivity of 97%, specificity of 92%, and accuracy of 96% in detecting crossing vessels associated with UPJ obstruction. [2]
Retrograde pyelography at the time of surgery is often used to estimate the length of the stricture and the amount of pelvis/ureter that needs to be excised at the time of the pyeloplasty to create a dependent funnel.
-
Intravenous pyelogram demonstrating ureteropelvic junction obstruction with dilatation of the collecting system and non-visualization of the ureter on delayed imaging.
-
Retrograde pyelogram demonstrating ureteropelvic junction obstruction secondary to annular stricture.
-
Retrograde pyelogram demonstrating ureteropelvic junction obstruction secondary to crossing vessels.
-
Intraluminal sonogram of ureteropelvic junction obstruction demonstrating multiple crossing vessels.
-
CT scan without contrast demonstrating severe left-sided hydronephrosis secondary to ureteropelvic junction obstruction.
-
CT scan with intravenous contrast demonstrating pooling of contrast and delayed excretion of contrast from a left-sided ureteropelvic junction obstruction.
-
Intraluminal sonogram demonstrating the renal vein surrounding the ureteropelvic junction and causing extrinsic compression and obstruction.
-
Retroperitoneal laparoscopic dissection showing UPJ with stent in place, pelvic stone and lower pole vessels.



