Practice Essentials
Intramedullary spinal cord tumors (IMSCTs), like the one depicted in the image below, refer to a subgroup of intradural spinal tumors that arise from cells within the spinal cord, as opposed to adjacent structures such as the nerve roots or meninges. They are much less common than brain tumors and are thought to account for 5-10% of all intrinsic tumors of the central nervous system. Their most common initial symptom is generalized back pain, which is very difficult to distinguish clinically from back pain from musculoskeletal conditions. Most intramedullary spinal cord tumors are considered to be glial in origin because they are histologically and immunohistochemically similar to differentiated non-neuronal cell types, such as ependymal cells and astrocytes, which occur in nonpathological spinal cord tissue. Because of the slow-growing nature of many of these tumors, symptoms precede diagnosis by an average of 2 years. Patients with malignant or metastatic spinal cord tumors present in the range of several weeks to a few months after symptoms develop. [1, 2, 3, 4, 5, 6]
The most commonly encountered intramedullary spinal tumors are ependymomas, astrocytomas, and hemangioblastomas. Collectively, spinal ependymomas and astrocytomas account for 80-90% of intramedullary spinal tumors, with ependymomas occurring roughly twice as frequently as astrocytomas. [7] In adults, ependymomas are the most common tumor type. In children, astrocytomas are the most common tumor type,
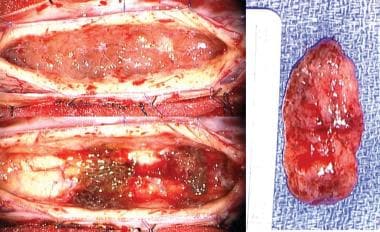 View of a cervical intramedullary ependymoma in situ after midline myelotomy and initial dissection (top left). The tumor was removed en bloc (right), and the postsurgical cavity in the spinal cord is shown (bottom left).
View of a cervical intramedullary ependymoma in situ after midline myelotomy and initial dissection (top left). The tumor was removed en bloc (right), and the postsurgical cavity in the spinal cord is shown (bottom left).
Diagnosis
MRI produces exquisite detail of the spinal cord. Most tumors are isointense or slightly hypointense as compared to the normal cord signal. Tumors generally exhibit some enhancement with gadolinium, and this enhancement may be homogenous or irregular. Contrast-enhanced MRI is very sensitive and may reveal minute lesions.
Plain radiographs of the spine cannot diagnose an intramedullary tumor but may be useful for surgical planning if the tumor is associated with a deformity.
Patients are often diagnosed only after the development of neurologic signs and symptoms that may occur later in the course of the disease. Early diagnosis is important, however, because surgical removal for most tumors is curative, and surgical results are optimized when tumors are smaller. Also, neurologic deficits resulting from intramedullary spinal cord tumors are seldom reversible. As such, functional outcomes after surgery are closely tied to the patient's preoperative neurologic condition.
In the case of a complete spinal block by the tumor, lumbar puncture may precipitate a disastrous shift in the intrathecal contents and, therefore, should not be the first test performed when a spinal cord tumor is suspected. Cerebrospinal fluid (CSF) may show extremely elevated protein levels, and xanthochromia may be present.
Treatment
The first-line treatment for intramedullary tumors is open surgical resection. Surgery is indicated for all symptomatic lesions. Small asymptomatic lesions may be followed clinically and radiographically because the majority of intramedullary tumors are relatively benign and slow growing. However, this approach carries the risk of the development of neurologic deficits that are likely not recoverable and the uncertainty that comes with undetermined diagnosis.
At surgery, aggressiveness with respect to resection depends on the histologic diagnosis of a frozen section and the ability to find and maintain a surgical plane.
Steroids are used in the perioperative period or if a rapid decline in neurologic function occurs. The slow-growing nature of these neoplasms makes proving the benefit of radiation therapy difficult.
In a study of 70 adult cases of intramedullary spinal cord tumors consisting of ependymomas, astrocytomas, carcinoma metastases, hemangioblastomas, cavernomas, and others, the investigators recommended evoked potential-guided microsurgical total resection for ependymomas and other benign lesions; partial resection or biopsy followed by adjuvant therapy for high-grade astrocytomas; and resection or biopsy for metastatic lesions.
A study of 225 patients with 250 intramedullary tumors found that 83.3% of displacing tumors underwent gross total resection (GTR), 22.5% of infiltrating tumors underwent GTR, and none of the nonproliferating tumors underwent GTR. Permanent morbidity (19.5%) was lowest after GTR and correlated significantly with surgical experience and the preoperative neurologic state. Patients with tumors of thoracic levels, tumor hemorrhages, and malignant and recurrent tumors were at a higher risk for permanent morbidity. [8]
A group of patients who underwent spinal surgery with the use of neurophysiologic intraoperative monitoring (NIOM) (N=38) were compared with a group who underwent surgery without NIOM (N=36), before the introduction of NIOM, and the number of neurologic complications was found to be significantly lower in the intramedullary procedure group with NIOM. There was no significant difference in the number of complications in patients undergoing intradural or extradural extramedullary procedures with NIOM versus without NIOM. [9]
Epidemiology
Spinal tumors occur with an incidence of 0.97 per 100,000 persons in the United States. [10] Spinal cord gliomas account for approximately 80% of intradural intramedullary spinal tumors. Of the spinal cord gliomas, astrocytomas constitute 30-40% and ependymomas 60-70%. However, hemangioblastomas, gangliogliomas, lymphomas, and melanomas also occur. [11, 5, 6]
In adults, intramedullary spinal tumors comprise 5-10% of all spinal tumors and are the most common spinal tumor in children. The most commonly encountered intramedullary spinal tumors are ependymomas, astrocytomas, and hemangioblastomas.. Collectively, spinal ependymomas and astrocytomas account for 80-90% of intramedullary spinal tumors, with ependymomas occurring roughly twice as frequently as astrocytomas. [7]
Astrocytoma accounts for 6-8% of all spinal cord tumors and is primarily low grade. It occurs in both adult and pediatric populations, with the most common presenting symptoms being back pain, sensory dysfunction, or motor dysfunction. [11, 5, 6]
Ependymoma is a common primary neoplasm of the spinal cord and filum terminale. It is the most common primary glial neoplasm of the spinal cord, constituting 50-60% of intramedullary cord neoplasms. They frequently present in middle age but can occur at any age. Ependymomas are believed to be slow-growing tumors. Because of their tendency to compress adjacent parenchyma, patients with spinal ependymomas usually experience gradual symptoms because of slow progression, making early diagnosis difficult. [12]
Hemangioblastomas are benign, slow-growing, highly vascularized tumors of the central nervous system, with the most common location being the posterior fossa. Hemangioblastomas are often associated with von Hippel-Lindau disease. [13]
In children, astrocytomas are the most common tumor type, accounting for around 60% of all intramedullary spinal tumors, and the mean age of presentation is 5-10 years.
Intramedullary spinal tumors can arise anywhere in the spinal cord, from the cervicomedullary junction to the filum terminale. Spinal ependymomas are found most frequently in the cervical cord, presumably because it contains more neural tissue than the thoracic or lumbar segments. [14, 15]
Hemangioblastomas and astrocytomas most commonly arise in the thoracic cord, followed by the cervical cord. [16]
Etiology
The etiology of intramedullary spinal tumors remains obscure but undoubtedly varies according to histology. Most intramedullary spinal cord tumors are considered to be glial in origin because they are histologically and immunohistochemically similar to differentiated non-neuronal cell types, such as ependymal cells and astrocytes, which occur in nonpathologic spinal cord tissue. The traditional thinking is that tumors occur when these differentiated cells, which normally stop propagating after spinal cord development, acquire mutations that cause them to divide again in an uncontrolled fashion.
There is increasing evidence that genes regulating radial glial cell differentiation play a role in molecular pathogenesis. Compared to supratentorial and posterior fossa ependymomas, spinal ependymomas overexpressed homeobox (HOX) family genes and insulinlike growth factor 1 (IGF1). Distinct malignant transformations in regional radial glial cells also can give rise to anatomically and molecularly distinct ependymomas. These findings underscore the notion that cranial and spinal ependymomas should be considered separately, for both clinical management and biological investigation. [7]
Individuals with type I and type II neurofibromatosis (NF1 and NF2) have been recognized for some time as having an increased incidence of intramedullary spinal tumors, as well many other kinds of tumors, compared with the general population. This general predisposition to tumors has been linked to germline mutations in 2 different genes named for their associated diseases. Patients with the NF1 gene are predisposed to spinal astrocytomas, whereas patients with the NF2 gene are predisposed to spinal ependymomas. Genetic analyses of spinal ependymomas from individuals without syndromic neurofibromatosis have shown somatic mutations in the NF2 gene in a subset of cases.
The identification of mitotically active neural stem cells and neural progenitor cells throughout the central nervous system has altered current thinking about how all intrinsic CNS tumors arise. Many lines of evidence point toward neural stem cells as the cells of origin in brain tumors. This line of inquiry is not nearly as advanced in the spinal cord, but some preliminary work has shown similarities between tumor cells from spinal ependymomas and neural stem cells from the spinal cord.
The other relatively common type of intramedullary spinal tumor is hemangioblastoma. Hemangioblastomas are thought to arise from red blood cell precursors and are not intrinsic spinal cord tumors, but they are often anatomically intramedullary because of their association with the blood vessels that penetrate and nourish the spinal cord. Hemangioblastomas occur as a result of mutations in a tumor suppressor gene called vhl, which was found to be altered in patients with the neurocutaneous disorder von Hippel-Lindau disease (VHL). Patients are predisposed to form hemangioblastomas in the brain and spinal cord, and somatic mutations in the vhl gene have been found in tumors from patients without syndromic VHL.
Pathophysiology
The pathophysiology of intramedullary spinal cord tumors varies according to tumor type. Ependymomas are usually indolent, encapsulated tumors that are histologically benign. Pain and neurologic deficits arise as a result of a progressive stretching and distortion of nerve fibers. Usually a clear anatomic plane is present at surgery, and a gross visual anatomic resection results in a cure. Rare anaplastic subtypes can be invasive, however, and are more likely to recur or spread through CSF spaces. Even histologically benign–appearing spinal ependymomas can metastasize in this way.
Although malignant forms do exist, most spinal astrocytomas are low grade (WHO grade II) and less aggressive than astrocytomas in the brain. Pain and neurologic defects arise from a combination of nerve fiber stretching and the invasion of cord parenchyma. Because they are infiltrative tumors, complete surgical removal without damage to functional tissue is usually not possible. Exceptions to this general rule may include some pilocytic astrocytomas of the spinal cord (WHO grade I) that are more common in children.
Hemangioblastomas are highly vascular tumors with capillaries that display an increased permeability thought to be related to a hypersensitivity to vascular endothelial growth factor (VEGF). Lesions usually become symptomatic because this capillary hyperpermeability leads to fluid collections or syringes, which are often larger than the tumor itself, causing mass effect in addition to stretching of neural pathways. These fluid spaces are not lined with tumor cells, however, and only the tumor nidus needs to be removed at surgery.
Presentation
Symptoms
The clinical features of intramedullary spinal cord tumors are variable. Symptoms are not specific to spinal cord tumors and may be present in any myelopathic process.
Because of the slow-growing nature of many of these tumors, symptoms precede diagnosis by an average of 2 years. Patients with malignant or metastatic spinal cord tumors present in the range of several weeks to a few months after symptoms develop.
Pain and weakness are the most common presenting symptoms of intramedullary spinal cord tumors. Pain is often the earliest symptom, classically occurring at night when the patient is supine. The pain is typically local over the level of the tumor but may radiate.
Progressive weakness may occur in the arms (cervical tumors) or legs (cervical, thoracic, conus tumors). Impaired bowel, bladder, or sexual function often occurs early. Patients may have poor balance. Rarely, symptoms of subarachnoid hemorrhage may be present.
Intratumoral hemorrhage can cause an abrupt deterioration, a presentation most often associated with ependymomas.
Examination
Examination may reveal a combination of upper and lower motor neuron signs. Lower motor signs may be at the level of the lesion and may aid in localization. Other signs evident upon physical examination may include spine tenderness, stiffening of gait, trophic changes of extremity, sensory loss, hyperreflexia, clonus, and scoliosis or torticollis (generally in children).
Indications
The first-line treatment for intramedullary tumors is open surgical resection. Surgery is indicated for all symptomatic lesions. Small asymptomatic lesions may be followed clinically and radiographically because the majority of intramedullary tumors are relatively benign and slow growing. However, this approach carries the risk of the development of neurologic deficits that are likely not recoverable and the uncertainty that comes with undetermined diagnosis.
At surgery, aggressiveness with respect to resection depends on the histologic diagnosis of a frozen section and the ability to find and maintain a surgical plane. Given the difficulty in determining many ependymomas from astrocytomas on frozen section, the presence or absence of a clear surgical plane is usually the key determining factor in defining the surgical goal. If, after analysis of all available data, including imaging characteristics, frozen section, and intraoperative appearance, a diagnosis of ependymoma is perceived, a complete surgical resection should be attempted. If a diagnosis of astrocytoma is perceived, most clinicians advocate a more limited debulking of only the tissue that is clearly abnormal.
External beam radiation is generally reserved for disseminated ependymomas and infiltrative astrocytomas but remains an option whenever radiographic residual or recurrent ependymoma is found. Stereotactic radiosurgery for intramedullary tumors remains untested.
Relevant Anatomy
The spinal cord originates at the foramen magnum and extends to the conus medullaris, which terminates at the L1-L2 vertebral body junction in adults. The pia matter condenses caudally to this area, extending to the sacrum as the filum terminale. It is an ovoid structure, most narrow in the anterior-posterior direction. At every vertebral level paired ventral and dorsal nerve roots exit the lateral aspect of the cord and coalesce to form 31 pairs of spinal nerves.
In contrast to the brain, the white matter of the spinal cord surrounds the interior gray matter. The spinal cord is covered by a supporting connective tissue layer called the pia matter that acts as a trellis for the vascular supply. A vestigial extension of the ventricular system, the central canal runs the length of the spinal cord. Dilation of the central canal may be pathologic in some instances. In general, ventral portion of the spinal cord parenchyma subserves motor function, whereas the dorsal portion subserves sensation. The spinal cord contains the same cell types as the brain, but these are highly specialized to their niche in the spinal cord.
The vascular supply for the spinal cord comes from the anterior spinal artery, the paired posterior spinal arteries, and the 31 radicular arteries. The anterior and posterior spinal arteries form off branches of the vertebral arteries at the cervicomedullary junction and course inferiorly along the length of the spinal cord. The anterior spinal artery is relatively constant and runs in the middle of the ventral surface of the cord, sending deep penetrating branches into the anterior median sulcus. These branches then send arterial twigs radially to the deepest portions of the spinal cord.
The paired posterior spinal arteries are relatively inconstant, course along the posterolateral surface of the cord, medial to the dorsal root entry zones, and send short penetrating end arterioles into the dorsal cord parenchyma. Thus, the anterior spinal artery supplies the ventral two thirds of the cord, whereas the posterior spinal artery supplies the dorsal third.
The spinal arteries form the nexus of an arterial network that is replenished by the radicular arteries that enter the spinal canal through the spinal nerve root sleeves. The radicular supply to the spinal cord is highly variable, but a few vital feeding arteries are usually present. The most important of these is the artery of Adamkiewicz, which is usually found on the left side, from T9 to L2.
Contraindications
Absolute contraindications to surgical intervention include uncorrected coagulopathy and systemic infection.
Relative contraindications to surgical intervention include complete neurologic deficit over 24 hours and short life expectancy.
-
The first panel shows a cervical syrinx. The differential diagnosis for syrinx includes trauma, Chiari malformation, and dysmerogenesis. A syrinx can also be the by product of a tumor, which may be distant anatomically from the associated syrinx. The second panel shows a small enhancing ependymoma of the thoracic spine that was found during the workup for the cervical syrinx.
-
This is a sagittal image of an enhancing conus medullaris lesion in a 45-year-old man who presented with midline back pain. This hemangioblastoma was removed completely. The patient remains neurologically intact, and imaging of his neuroaxis did not reveal other lesions.
-
Axial image of hemangioblastoma.
-
This is a sagittal image of an enhancing cord lesion in a 41-year-old man with a rapidly progressing severe quadriparesis. A biopsy showed this to be sarcoidosis. Following treatment with steroids, he is now ambulatory with assistance.
-
Axial image.
-
View of a cervical intramedullary ependymoma in situ after midline myelotomy and initial dissection (top left). The tumor was removed en bloc (right), and the postsurgical cavity in the spinal cord is shown (bottom left).






