Practice Essentials
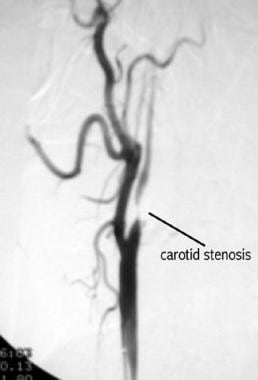
Atherosclerosis is a diffuse, degenerative disease of the arteries that results in the formation of plaques composed of necrotic cells, lipids, and cholesterol crystals. These plaques can cause stenosis (see the image below), embolization, and thrombosis. Atherosclerosis has a predilection for certain arteries, including the extracranial carotid artery.
Signs and symptoms
Atherosclerotic disease of the carotid artery may be associated with the following:
-
Amaurosis fugax (transient ipsilateral visual loss)
-
Transient ischemic attacks (TIAs)
-
Crescendo TIAs
-
Stroke-in-evolution
-
Cerebral infarction
See Overview for more detail.
Indications and contraindications for carotid endarterectomy
Indications
Indications for carotid endarterectomy (CEA), based on prospective randomized trials, include the following:
-
Symptomatic patients with greater than 70% stenosis - Clear benefit was found in the North American Symptomatic Carotid Endarterectomy Trial (NASCET) [1]
-
Symptomatic patients with greater than 50-69% stenosis - Benefit is marginal; appears to be greater for male patients
-
Asymptomatic patients with greater than 60% stenosis - Benefit is significantly less than for symptomatic patients with greater than 70% stenosis
Note: The percentage of stenosis used as the threshold for CEA varies among available literature. Generally, symptomatic patients with greater than 50% stenosis and healthy, asymptomatic patients with greater than 60% stenosis warrant consideration for CEA.
Contraindications
Contraindications for CEA include the following:
-
Patients with a severe neurologic deficit following a cerebral infarction
-
Patients with an occluded carotid artery
-
Concurrent medical illness that would significantly limit the patient’s life expectancy
Laboratory and radiologic studies
Studies to be considered include the following:
-
Complete blood count
-
Levels of electrolytes, blood urea nitrogen, creatinine
-
Lipid profile
-
Coagulation studies - Prothrombin time/activated partial thromboplastin time
-
Electrocardiography (ECG) - To identify evidence of prior MI as well as ischemic changes
-
Carotid duplex ultrasonography (US), with or without color - Screening test of choice to evaluate for carotid stenosis
-
Cranial computed tomography (CT) or magnetic resonance imaging (MRI) - To rule out other intracranial lesions and to identify the presence of new and old cerebral infarcts
-
Carotid magnetic resonance angiography (MRA) - May be useful in collaborating the finding of an occluded carotid with duplex US; however, this modality tends to overstate the significance of the stenosis
-
Aortic arch and carotid arteriography - To evaluate the percentage of stenosis
See Workup for more detail.
Management
Treatment of atherosclerosis of the carotid artery is dependent on the severity and degree of the disease.
Pharmacotherapy
Medications used to manage atherosclerotic disease of the carotid artery include the following:
-
Antiplatelet agents (eg, aspirin, ticlopidine, clopidogrel)
-
Statin therapy (atorvastatin, rosuvastatin, simvastatin, pravastatin, lovastatin)
-
Anticoagulants (eg, warfarin) - Note that the use of warfarin in patients with noncardiac emboli is controversial
Surgery
Management of atherosclerotic disease of the carotid artery includes the following procedures:
-
CEA
-
Carotid angioplasty and stenting (CAS)
-
Transcarotid artery revascularization (TCAR)
See Treatment for more detail.
Background
Atherosclerosis is a degenerative disease of the arteries that results in the formation of plaques composed of necrotic cells, lipids, and cholesterol crystals (see the images below). These plaques can result in symptoms by causing stenosis, by embolizing, or by thrombosing. Atherosclerosis is a diffuse process with a predilection for certain arteries. This article describes the history and impact of this process as it occurs in the extracranial carotid artery.
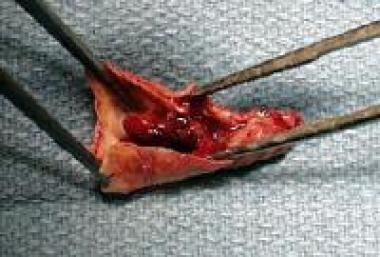
 Atherosclerotic plaque removed at time of carotid endarterectomy (areas of ulceration with thrombus and intraplaque hemorrhage are present).
Atherosclerotic plaque removed at time of carotid endarterectomy (areas of ulceration with thrombus and intraplaque hemorrhage are present).
For patient education resources, see the Brain and Nervous System Center and the Cholesterol Center, as well as Stroke, High Cholesterol, Understanding Your Cholesterol level, and Lifestyle Cholesterol Management.
Anatomy
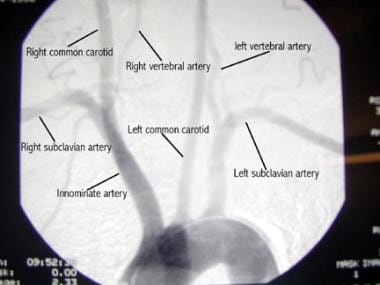
The carotid artery originates from the innominate artery on the right and directly from the aortic arch on the left. The carotid artery enlarges in the midneck, forming the carotid bulb, before bifurcating into the external and internal carotid arteries. The carotid sinus and carotid body are located at the bifurcation (see the image below).
Pathophysiology
Currently, embolization is considered the most common mechanism causing ischemic strokes from atherosclerotic lesions in the carotid bulb. Thrombosis and low flow are other possible mechanisms.
Stroke is one of the most devastating complications of carotid stenosis. However, carotid stenosis is not the only cause of stroke. In fact, among patients with asymptomatic stenosis of 60-99%, as many as 45% of strokes may be caused by lacunar infarcts or cardiac emboli.
Epidemiology
Stroke from any cause represents the third leading cause of death in the United States. About 610,000 new strokes occur each year in the United States, and about 185,000 occur in people who have previously had a stroke. [2] Stroke is the leading cause of serious long-term disability in the United States. Between 2014 and 2015, the direct and indirect cost of stroke in the United States was estimated at nearly $46 billion. [2]
Prognosis
Cranial nerve injuries occur in 2-7% of patients. Recurrent laryngeal and hypoglossal nerve dysfunctions are the most common. Postoperative stroke occurs in 1-5% of patients. [1] The perioperative mortality is 0.5-1.8%. Recurrent stenosis develops in 1-20% of cases, and reoperation is necessary in 1-3% of cases.
Pharmacotherapy vs intervention
In the North American Symptomatic Carotid Endarterectomy Trial (NASCET), the 2-year stroke risk after a successful carotid endarterectomy (CEA) was 1.6%, compared with 12.2% for the medically managed patients. [1] The cumulative risk of an ipsilateral stroke was 9% for the surgical patients and 26% for the medically managed patients.
In the Asymptomatic Carotid Atherosclerosis Study (ACAS), the 5-year risk for ipsilateral stroke was 5.1% for the surgical group and 11% for the medical group. [3] The stroke risk of arteriography was attributed to the surgical group and was 1.2%.
Endarterectomy vs stenting
The Endarterectomy Versus Stenting in Patients With Symptomatic Severe Carotid Stenosis (EVA-3S) trial revealed a higher stroke and death rate with carotid artery stenting (CAS); however, cerebral protection was not uniformly used, and dual antiplatelet therapy was not initiated on all patients. [4]
A meta-analysis revealed that protected CAS (with the use of an embolic protection wire) was associated with an 8.2% rate of stroke or death at 30 days, compared with 6.2% for surgery [5] ; however, the rates of disabling stroke or death within this period were not significantly different between the two groups.
Meier et al conducted a systematic review and meta-analysis of 11 randomized controlled clinical trials to evaluate the relative short-term safety and intermediate-term efficacy of CEA versus CAS. [6] CEA carried a lower risk of periprocedural mortality or stroke than CAS did, mainly because of a decreased risk of stroke. However, the risk of death and the composite endpoint of mortality or disabling stroke did not differ significantly between the two procedures. In addition, the odds of periprocedural myocardial infarction (MI) or cranial nerve injury (CNI) were higher among the CEA group as compared with the CAS group. In the intermediate term, the risk of stroke or death did not differ significantly between the two.
Numerous studies, including the Stenting and Angioplasty with Protection in Patients at High Risk for Endarterectomy (SAPPHIRE) trial, have found that CAS is not inferior to CEA at 1 year. Published long-term results show no significant difference between groups in the prespecified secondary endpoint trial, a composite at 3 years of death, stroke, or MI within 30 days of the procedure (or death or ipsilateral stroke between 31 and 1080 days). [7]
A study by Illuminati et al suggested that with regard to the timing of CEA, previous or simultaneous CEA in patients with unilateral severe asymptomatic carotid stenosis (>70%) undergoing coronary artery bypass grafting (CABG) was better able to prevent stroke than delayed CEA was. [8] The overall surgical risk was not increased.
A study by Brown et al suggested that the risk of external carotid artery occlusion may be lower with CEA than it would be with CAS, though such occlusion after CAS was still uncommon overall (~4%) and was not associated with in-stent restenosis. [9]
The Carotid Revascularization Endarterectomy vs Stenting Trial (CREST) evaluated the outcomes of 2502 patients with symptomatic or asymptomatic carotid stenosis after undergoing CAS or CEA, and found that the risk of stroke, MI, or death was similar between the two procedures. [10]
Although there was no difference in the primary outcome of CREST, there was a higher risk of periprocedural stroke in the group who underwent CAS, whereas there was a higher risk of MI in the group undergoing CEA. [10] Additional analysis, however, indicated that stroke had an adverse long-term effect on quality-of-life measures, whereas MI did not. Further study of the CREST data showed that 4-year mortality was significantly higher in patients who had a stroke after intervention (21.1% vs 11.6%). [11]
Whereas CNI occurred in 4.6% of the CREST patients who underwent CEA, there was a 80% rate of resolution at 1 year, and there was no statistical difference in health-related quality-of-life outcomes between patients who had CNI and those who did not. [12]
Brott et al carried out a pooled analysis of individual patient data (N = 4754) from the EVA-3S, SPACE (Stent-Protected Percutaneous Angioplasty of the Carotid Artery versus Endarterectomy), ICSS (International Carotid Stenting Study), and CREST trials to compare long-term outcomes of CEA and CAS for treatment of symptomatic carotid stenosis. [13] Patients were followed for a maximum of 12.4 years (median follow-up, 2.0-6.9 years). The primary outcome was the composite risk of stroke or death within 120 days after randomization (periprocedural risk) or subsequent ipsilateral stroke up to 10 years after randomization (postprocedural risk).
In patients who underwent CEA, 129 periprocedural and 55 postprocedural outcome events occurred, compared with 206 periprocedural and 57 postprocedural outcome events in those who underwent CAS. [13] After the periprocedural period, annual rates of ipsilateral stroke per person-year were 0.60% for CEA and 0.64% for CAS. Overall, the combined periprocedural and postprocedural risks favored CEA; treatment differences at 1, 3, 5, 7, and 9 years ranged from 2.8% to 4.1%. However, the similarity in postprocedural rates suggested that improvements in the periprocedural safety of CAS could yield outcomes similar to those of CEA in the future.
Transcarotid artery revascularization
Transcarotid artery revascularization (TCAR) represents an alternative to CAS in which the risk of navigating the often diseased atherosclerotic arch is eliminated through the use of direct, open surgical access to the proximal common carotid artery. Additionally, the use of flow reversal as embolic protection allows the institution of cerebral protection before the lesion is engaged, which has been shown to be the primary mechanism of stroke reduction in TCAR. [14]
The initial ROADSTER 1 and 2 trials evaluating the 30-day and 1-year safety of TCAR demonstrated high technical success rates (96.5%) and favorable safety outcomes, with a 30-day ipsilateral stroke rate of 1.4%, a 1-year ipsilateral stroke rate of 0.4%, respectively, a composite 30-day stroke/death rates of 2.3%, and a stroke/MI/death rates of 3.2%. [15, 16]
Multiple studies have demonstrated the safety of TCAR in comparison with both CEA and transfemoral CAS. Observational comparative registry studies evaluating TCAR and CEA among patients entered into the Society for Vascular Surgery (SVS) Vascular Quality Initiative (VQI) TCAR Surveillance Project (TSP) registry and the CEA database, respectively, demonstrated comparable stroke/death rates among patients undergoing TCAR as compared with CEA, despite higher rates of medical comorbid conditions. [17]
Other comparative studies evaluating in-hospital outcomes of TCAR and transfemoral CAS demonstrated that patients undergoing TCAR, despite having higher rates of comorbid conditions, had a significantly lower risk of stroke or death. [18, 19]
-
Arteriogram of aortic arch and its branches.
-
Arteriogram of carotid stenosis.
-
Atherosclerotic plaque removed at time of carotid endarterectomy (areas of ulceration with thrombus and intraplaque hemorrhage are present).
-
Carotid artery exposed prior to carotid endarterectomy (coil present in internal carotid artery).
-
Carotid artery following endarterectomy and prior to closure (tapered endpoint and smooth appearance of lumen).
-
Carotid artery following Dacron patch angioplasty.
-
Selective left carotid angiogram.
-
Oblique view of left carotid artery demonstrating lesion within internal carotid artery.
-
Placement of stent into internal carotid artery. Note filter wire in upper photos (dots at top of internal carotid artery).
-
Angioplasty after stent placement; again, note filter wire protecting distal carotid artery.
-
Completion arteriogram displaying improvement in diameter of internal carotid artery.
-
Normal carotid arteries on color flow duplex ultrasonography.
-
Color flow duplex ultrasonogram reveals 80-99% left carotid stenosis and normal right carotid.
-
Carotid plaque.





