Practice Essentials
Nonarticular rheumatic pain syndromes can be classified into five general categories, as follows:
- Tendonitis and bursitis, such as the common lateral epicondylitis (tennis elbow) and trochanteric bursitis
- Structural disorders, such as pain syndromes resulting from flatfoot and the hypermobility syndrome
- Neurovascular entrapment, such as carpal tunnel syndrome and thoracic outlet syndrome
- Regional myofascial pain syndromes, with trigger points similar to those of fibromyalgia but in a localized distribution, such as the temporomandibular joint syndrome
- Generalized pain syndromes, such as fibromyalgia (FMS) and multiple bursitis-tendonitis syndrome
The more generalized and chronic the syndrome, the more difficult it is to treat.
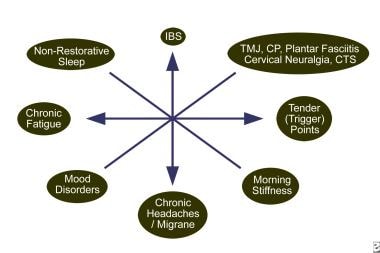
The spectrum of nonarticular pain syndromes and their interactions with mood disorders and chronic fatigue is depicted in the image below. Comorbidity is common. [1, 2]
The following articles provide additional information:
Pathophysiology
Tendonitis presents as local pain, inflammation, dysfunction, and degeneration. It can be associated with overuse, infection, systemic rheumatic disease, or metabolic disturbance such as calcium apatite or pyrophosphate deposition. Fluoroquinolone antibiotic use can be associated with tendonitis and rupture. Inflammation can cause "triggering," in which the digit locks and a snapping sensation is felt upon release. [3]
Bursitis presents as local pain and inflammation of the synovial fluid–filled saclike structures that protect soft tissues from underlying bone. Overuse, infection, trauma, systemic rheumatic disease, and metabolic disturbance such as calcium apatite or pyrophosphate deposition can also cause bursitis. Gout often causes olecranon bursitis and prepatellar bursitis.
Structural disorders such as scoliosis, lateral patellar subluxation, flatfoot, or other body asymmetry can cause local pain but are not always a source of pain or dysfunction. [4] Individuals whose condition falls into the category of hypermobility spectrum disorders often present with polyarthralgias due to increased joint laxity in the face of muscle disuse.
Neurovascular entrapment can occur centrally (eg, in spinal stenosis), in deep tissues (eg, thoracic outlet syndrome), or more peripherally (eg, carpal or tarsal tunnel syndromes). [5, 6, 7, 8] Bone enlargement due to osteophytes, muscular tension, and inflammation can contribute to narrowing of a neurovascular passage. Pain and paresthesia usually occur distal to the site of entrapment.
Regional myofascial pain syndromes, such as temporomandibular joint syndrome, may represent a pain-spasm pain cycle triggered by mechanical injury, such as strain or overuse. [9]
Multiple bursitis and tendonitis syndrome presents with anatomically localized areas of pain and dysfunction. Pain can be widespread, but the muscle tender points observed in fibromyalgia are absent. Usually, much less fatigue occurs, and responses to local therapies are better than in fibromyalgia.
Fibromyalgia, in many cases, presents as a form of allodynia, in which usually painless stimuli are perceived as painful, and hyperalgesia, in which normally painful stimuli is amplified. It is currently believed to be a disorder of pain regulation, also known as a type of central pain sensitization. Cerebrospinal fluid levels of substance P are elevated, and additional abnormalities in the serotonin system and in the regulation of cortisol exist. Studies showing abnormalities of cerebral blood flow in the thalamus and caudate nucleus help support the likelihood that pain processing in the central nervous system behaves abnormally. [10, 11, 12]
Fibromyalgia can also coexist with various autoimmune diseases and onset may follow a severe flulike syndrome, a defined infection (eg, Lyme disease), or other physical or mental trauma. Sleep is often disturbed, and nonrestorative sleep is associated with increased pain. The increased prevalence in females may suggest a hormonal influence. Few abnormalities occur in the peripheral musculature.
A study by Light and colleagues found that patients with chronic fatigue syndrome (myalgic encephalomyelitis) have an increased expression of sensory, adrenergic, and immune genes during moderate exercise. [13] Abnormalities of the neuroendocrine immune system are well documented, but none has yet been proven to be sensitive and specific enough to be used as a criterion for diagnosis.
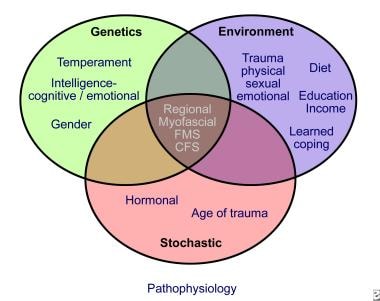
Psychological, personality, and social factors may play important roles in many chronic cases of local and generalized pain syndromes. The image below depicts possible factors that contribute to the generation of these syndromes.
Etiology
The cause of fibromyalgia has not been elucidated. A possible link between chronic fatigue syndrome and a little-known infectious retrovirus, xenotropic murine leukemia virus–related virus (XMRV) [14] proved unreliable. [15]
Associated conditions, but not necessarily etiologic factors for fibromyalgia, may include the following:
-
Severe flulike syndrome
-
Autoimmune diseases (eg, rheumatoid arthritis [RA], systemic lupus erythematosus [SLE])
-
A defined infection (eg, Lyme disease, hepatitis C, HIV)
-
Physical trauma (eg, a motor vehicle accident)
-
Chronic disturbed sleep (eg, insomnia or undiagnosed obstructive sleep apnea)
-
Family history of fibromyalgia
-
Female sex
-
Psychological stress and depression
-
Emotional trauma
Many of the above associated factors may contribute to multiple bursitis-tendonitis syndrome, which may be a subset of fibromyalgia.
Possible etiologic factors for other conditions include the following:
-
Regional and local bursitis and tendonitis are often associated with repetitive motion and localized trauma.
-
Fluoroquinolones have been linked to tendonitis, as have systemic disorders such as rheumatoid arthritis and spondyloarthropathies.
-
Carpal tunnel syndrome may be idiopathic or may be associated with pregnancy, endocrine disorders (eg, hypothyroidism, acromegaly), wrist synovitis (eg, rheumatoid arthritis, gout, pseudogout), and systemic illnesses such as amyloidosis (eg, primary, secondary to hemodialysis).
-
Hypermobility syndrome appears in familial clusters, indicating a genetic predisposition. Defined genetic disorders characterized by joint laxity include Ehlers-Danlos syndrome, Marfan syndrome, and pseudoxanthoma elasticum.
Epidemiology
United States
The incidence of all types of soft tissue rheumatism has been estimated at about 4000 per 100,000 population. The prevalence rate of fibromyalgia is about 2% of the population. [16]
International
International incidence and prevalence are similar to those in the United States.
Race-, Sex-, and Age-related Demographics
Racial differences in prevalence have not been reported.
Localized nonarticular rheumatism occurs with fairly equal distribution between males and females. In contrast, the female-to-male ratio of fibromyalgia is about 8:1, affecting about 3.5% of females and 0.5% of males in the United States.
Nonarticular rheumatism is most common in persons aged 45-64 years, and less than 0.2% of people with nonarticular rheumatism are younger than 14 years. Fibromyalgia is most common in women in their fifth decade of life and is rare in prepubescent girls. The prevalence of fibromyalgia in women aged 60-79 years is 7%. [16, 17]
Prognosis
These syndromes are not life threatening but can be a cause of significant functional disability. [18, 17]
Prognosis in fibromyalgia and multiple bursitis-tendonitis syndrome
In one study, 65% of patients improved with therapy. A similar percentage reported feeling poor or fair 3 years after diagnosis. About 10-30% of patients are disabled because of fibromyalgia. Most patients function well but continue to report chronic pain. Complete remissions are uncommon.
Better response to treatment is observed in patients of younger age with continued employment, supportive families, an absence of affective disorders, and without involvement in litigation. [19] One study showed that the level of disease activity did not change significantly over an average of 6.4 years that patients were studied. These findings suggest that current conventional medical treatment is unsatisfactory and does not alter the prognosis in fibromyalgia.
Regional and local bursitis, tendonitis, neurovascular entrapment, and structural syndromes
Most patients do well with therapy. Exacerbations are common but respond well to treatment.
Patient Education
Internet resources for patient education include the following:
-
The Arthritis Foundation has patient education pamphlets, support group information, and physician referrals.
-
National Institutes of Arthritis and Musculoskeletal and Skin Diseases has questions and answers and information sources for patients.
-
Fibrohugs is an Internet support network.
For additional patient education information, see Fibromyalgia, Chronic Pain, and Tennis Elbow.
-
The spectrum of nonarticular myofascial pain syndromes.
-
Possible factors that lead to myofascial pain syndromes.