Background
A pacemaker-mediated tachycardia (PMT) can be defined as any condition in which a pacemaker paces the ventricles at rates that are inappropriately fast. [1] This can be due to (1) a rate response setting that is too sensitive, (2) tracking of atrial noise (such as what may occur with electromagnetic interference), (3) inappropriate pacemaker manipulation with rate response turned on, or (4) tracking of an atrial tachyarrhythmia related to upper rate settings.
Traditionally, however, the term pacemaker-mediated tachycardia, also called endless-loop tachycardia, is used to refer to a form of a reentrant tachycardia and can occur in patients who have dual-chamber pacemakers. [16] The pacemaker forms the anterograde (atrium to ventricle [A → V]) limb of the circuit and the atrioventricular (AV) node is the retrograde limb (ventricle to atrium [V → A]) of the circuit. [2] This classic form is referred to and discussed as PMT for the rest of this article.
See the electrocardiograms (ECG) below.
 Pacemaker-Mediated Tachycardia. Telemetered ECG tracing with surface lead II (top) and intracardiac electrograms (atrial electrogram [center] and ventricular electrogram [lower]) and marker channel (bottom) showing pacemaker-mediated tachycardia (PMT). The intracardiac markers indicate that the retrograde P waves, labeled AS for atrial-sensed event, occur 280 milliseconds after the ventricular-paced beats, labeled VP.
Pacemaker-Mediated Tachycardia. Telemetered ECG tracing with surface lead II (top) and intracardiac electrograms (atrial electrogram [center] and ventricular electrogram [lower]) and marker channel (bottom) showing pacemaker-mediated tachycardia (PMT). The intracardiac markers indicate that the retrograde P waves, labeled AS for atrial-sensed event, occur 280 milliseconds after the ventricular-paced beats, labeled VP.
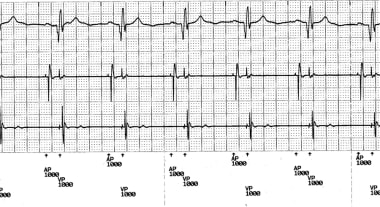 Pacemaker-Mediated Tachycardia. Telemetered ECG tracing showing atrioventricular (AV)–paced rhythm at 60/min after termination of the pacemaker-mediated tachycardia (PMT). The tracing, from top to bottom, shows lead II, atrial electrogram, ventricular electrogram, and marker channels. The intracardiac markers indicate the rhythm is atrial paced (AP) and ventricular paced (VP). Note that the VP beats are ventricular pseudofusion beats.
Pacemaker-Mediated Tachycardia. Telemetered ECG tracing showing atrioventricular (AV)–paced rhythm at 60/min after termination of the pacemaker-mediated tachycardia (PMT). The tracing, from top to bottom, shows lead II, atrial electrogram, ventricular electrogram, and marker channels. The intracardiac markers indicate the rhythm is atrial paced (AP) and ventricular paced (VP). Note that the VP beats are ventricular pseudofusion beats.
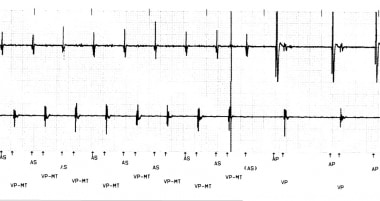 Pacemaker-Mediated Tachycardia. This is a typical example of PMT with ventricular pacing at maximum tracking rate (VP-MT) and then termination of the tachycardia as the atrial sensing (AS) is in the postventricular atrial refractory period (PVARP). This is due to PVARP extension, which is a feature of this particular pacemaker. The solid line indicates where PMT is detected and this is the point at which PVARP extension occurs. As this electrogram was detected, but not sensed to be acted upon, the ventricular tracking stopped and the tachycardia terminated. In some cases, pacemakers have a program to lengthen the PVARP after PMT detection to potentially stop the tachycardia. Alternatively, prevention of one ventricular paced beat can also stop the tachycardia. Some pacemakers use this algorithm.
Pacemaker-Mediated Tachycardia. This is a typical example of PMT with ventricular pacing at maximum tracking rate (VP-MT) and then termination of the tachycardia as the atrial sensing (AS) is in the postventricular atrial refractory period (PVARP). This is due to PVARP extension, which is a feature of this particular pacemaker. The solid line indicates where PMT is detected and this is the point at which PVARP extension occurs. As this electrogram was detected, but not sensed to be acted upon, the ventricular tracking stopped and the tachycardia terminated. In some cases, pacemakers have a program to lengthen the PVARP after PMT detection to potentially stop the tachycardia. Alternatively, prevention of one ventricular paced beat can also stop the tachycardia. Some pacemakers use this algorithm.
Repetitive nonreentrant ventriculoatrial synchrony (RNRVAS) is a ventriculoatrial synchrony pacemaker-mediated arrhythmia that only occurs in the presence of retrograde VA conduction and dual-chamber or cardiac resynchronization devices with tracking (eg, DDD, DDDR) or nontracking pacing modes that allow AV-sequential pacing (eg, DDI, DDIR). [3]
Gjermeni et al recently reported a novel pacemaker-mediated arrhythmia that closely mimics RNRVAS but exhibits a different mechanism and was independent of VA conduction (pseudo-RNRVAS). [4] The investigators interrogated 840 dual-chamber or biventricular devices and identified 9 patients with this arrhythmia. The authors conclude that pseudo-RNRVAS is underrecognized because there are no specific device algorithms to detect and store them. [4]
Pathophysiology
The following is the most common scenario causing pacemaker-mediated tachycardia (PMT). A dual-chamber pacemaker programmed DDD or VAT, but not DDI, is implanted. The patient must have retrograde (V→A) conduction with an atrial activation time that is longer than the programmed postventricular atrial refractory period (PVARP). A ventricular-paced beat or a properly timed premature ventricular contraction (PVC) conducts retrograde via the AV node (or an accessory pathway, if present) to the atrium. If the atrial depolarization occurs after the set PVARP, but before the next timed atrial-paced beat, ventricular pacing will be triggered at the programmed AV interval.
PMT tends to occur at or near the programmed upper rate limit and depend upon the programmed AV delay and the PVARP. This generates an incessant reentrant arrhythmia circuit that persists as long as there is continuous VA conduction with atrial activation outside the PVARP. The pacemaker forms the antegrade limb of the circuit and VA conduction forms the retrograde limb as the essential critical components. [2] In many instances, the PVARP varies so that it shortens with rate. This can make PMT more likely. The AV interval can be programmed to change with the rate. This tends to reduce the risk of PMT. Depending on the pacemaker programming and the VA conduction, the rate of the PMT may vary, but it is bounded by (and generally occurs near or at) the programmed upper rate limit.
Although PMT is commonly initiated by an isolated ventricular ectopic beat, it can also be initiated by failure to capture the atrium with a paced beat followed by a ventricular paced beat. If this occurs, the atrium is then amenable to depolarization by the impulse conducted retrograde from the ventricle. The tachycardia continues until retrograde conduction ends or the atrium becomes refractory. Specific pacemaker algorithms may also terminate PMT if tracked rates persist at the upper rate limit. The pacemaker can be programmed to lengthen the PVARP after a PVC or with an incessant tachycardia at the upper rate limit or prevent one atrial sensed event from being tracked. Up to one third of patients with antegrade complete AV block have intact (or intermittent) retrograde (V→A) conduction. It has been recommended that testing for retrograde conduction be performed in all patients with AV block in order to optimize device programming and prevent PMTs. [5]
Other situations that can result in PMT include intermittent atrial undersensing. An atrial premature beat with a long A sense-V pace interval (due to a long programmed AV interval) in a patient with heart block can also initiate PMT as any antegrade concealed depolarization otherwise present cannot prevent VA conduction in this instance. [6]
Prognosis
Prognosis is not directly altered by an episode of pacemaker-mediated tachycardia (PMT) and is defined by the patient's underlying cardiac or medical condition.
Indirectly, in a rare event such as PMT-induced syncope, a patient could sustain injury as a result of the syncope.
Persistent PMT can cause hypotension and heart failure symptoms.
Morbidity/mortality
Patients may experience palpitations, rapid heart rates, lightheadedness, syncope, or chest discomfort.
Complications
PMT rarely is associated with any serious complications such as presyncope or syncope.
In many patients, the condition may be asymptomatic and is noted only with ECG or Holter monitoring.
With the appropriate programming interventions described above, the problem usually is resolved, and, in most modern pacemakers, it can be detected and treated by the device itself.
In patients who develop chest pain (angina pectoris) associated with the rapid pacing rate, consider a stress test to evaluate for coronary artery disease.
-
Pacemaker-Mediated Tachycardia. Telemetered ECG tracing with surface lead II (top) and intracardiac electrograms (atrial electrogram [center] and ventricular electrogram [lower]) and marker channel (bottom) showing pacemaker-mediated tachycardia (PMT). The intracardiac markers indicate that the retrograde P waves, labeled AS for atrial-sensed event, occur 280 milliseconds after the ventricular-paced beats, labeled VP.
-
Pacemaker-Mediated Tachycardia. Telemetered ECG tracing showing atrioventricular (AV)–paced rhythm at 60/min after termination of the pacemaker-mediated tachycardia (PMT). The tracing, from top to bottom, shows lead II, atrial electrogram, ventricular electrogram, and marker channels. The intracardiac markers indicate the rhythm is atrial paced (AP) and ventricular paced (VP). Note that the VP beats are ventricular pseudofusion beats.
-
Pacemaker-Mediated Tachycardia. This is a typical example of PMT with ventricular pacing at maximum tracking rate (VP-MT) and then termination of the tachycardia as the atrial sensing (AS) is in the postventricular atrial refractory period (PVARP). This is due to PVARP extension, which is a feature of this particular pacemaker. The solid line indicates where PMT is detected and this is the point at which PVARP extension occurs. As this electrogram was detected, but not sensed to be acted upon, the ventricular tracking stopped and the tachycardia terminated. In some cases, pacemakers have a program to lengthen the PVARP after PMT detection to potentially stop the tachycardia. Alternatively, prevention of one ventricular paced beat can also stop the tachycardia. Some pacemakers use this algorithm.





