Practice Essentials
The brain is surrounded by cerebrospinal fluid (CSF), enclosed in meningeal covering, and protected inside the skull. Furthermore, the fascia and muscles of the scalp provide additional cushioning to the brain. Test results have shown that 10 times more force is required to fracture a cadaveric skull with overlaying scalp than the one without. [1] Although these layers play a protective role, meningeal attachments to the interior of the skull may limit the movement of the brain, transmitting shearing forces on the brain.
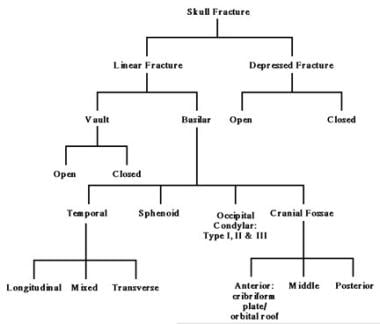
Fractures of the skull can be classified as linear or depressed. Linear fractures are either vault fractures or skull base fractures.Vault fractures and depressed fractures can be either closed or open (clean or dirty/contaminated). [2, 3]
A transverse temporal bone fracture is shown in the image below.
 Transverse temporal bone fracture (courtesy of Adam Flanders, MD, Thomas Jefferson University, Philadelphia, Pennsylvania)
Transverse temporal bone fracture (courtesy of Adam Flanders, MD, Thomas Jefferson University, Philadelphia, Pennsylvania)
CSF plays a major role in coup and countercoup injuries to the brain. A blow to a stationary but moveable head causes acceleration, and the brain floating in CSF lags behind, sustaining an injury directly underneath the point of impact (coup injury). When a moving head hits the floor, sudden deceleration results in an injury to the brain on the opposite side (countercoup injury).
CT scan is the criterion standard modality for aiding in the diagnosis of skull fractures. [4, 5, 6] Thinly sliced bone windows of up to 1-1.5 mm thick, with sagittal reconstruction, are useful in assessing injuries. Helical CT scan is helpful in occipital condylar fractures, but 3-dimensional reconstruction usually is not necessary. [7]
The American Colllege of Radiology Appropriateness Criteria for head trauma includes the following [8, 9] :
-
Skull radiography has been supplanted by CT in characterizing skull fractures in the setting of acute traumatic brain injury, though it may be useful in limited circumstances, such as radiopaque foreign bodies.
-
Contrast-enhanced MRI or CT may be helpful if posttraumatic infection is clinically suspected in patients with risk factors such as skull base fractures.
-
Traumatic dural sinus thrombosis is most commonly seen in patients with skull fractures that extend to a dural venous sinus or the jugular foramen.
-
Cerebrospinal fluid leak occurs in 10-30% of skull base fractures and most often presents with rhinorrhea (80% of cases) in the setting of frontobasal fracture.
-
In children, radiographs of the skull are known to have a low predictive value in determining intracranial injury. However, in contrast to accidental head trauma, where radiographs have largely been replaced by CT, skull radiographs are still often performed as part of the skeletal survey in evaluation of suspected nonaccidental trauma. It has been generally accepted that skull radiographs and head CT are complementary examinations, since fractures in the plane of the transaxial CT image may not be apparent on the head CT examination.
Adults with simple linear fractures who are neurologically intact do not require any intervention and may even be discharged home safely and asked to return if symptomatic. Infants with simple linear fractures should be admitted for overnight observation regardless of neurological status. [3]
The role of surgery is limited in the management of skull fractures. Infants and children with open depressed fractures require surgical intervention. Most surgeons prefer to elevate depressed skull fractures if the depressed segment is more than 5 mm below the inner table of adjacent bone. Indications for immediate elevation are gross contamination, dural tear with pneumocephalus, and an underlying hematoma.
A study of 66 skull fractures in children (mean age, 5.9 yr) supported previous evidence that routine skull radiographs are of little benefit in cases of minor head trauma and that additional CT scans are not indicated in symptomatic children with linear fractures. The authors noted that CT scans should be used only in cases in which neurologic symptoms are present. [10]
Anatomy of fracture
The causative forces and fracture pattern, type, extent, and position are important in assessing the sustained injury. The skull is thickened at the glabella, external occipital protuberance, mastoid processes, and external angular process and is joined by 3 arches on either side. The skull vault is composed of cancellous bone (diploë) sandwiched between 2 tablets, the lamina externa (1.5 mm), and the lamina interna (0.5 mm). The diploë does not form where the skull is covered with muscles, leaving the vault thin and prone to fracture.
The skull is prone to fracture at certain anatomic sites that include the thin squamous temporal and parietal bones over the temples and the sphenoid sinus, the foramen magnum, the petrous temporal ridge, and the inner parts of the sphenoid wings at the skull base. The middle cranial fossa is the weakest, with thin bones and multiple foramina. Other places prone to fracture include the cribriform plate and the roof of orbits in the anterior cranial fossa and the areas between the mastoid and dural sinuses in the posterior cranial fossa.
History of the Procedure
Skull fracture is described in Edwin Smith's papyrus, the oldest known surgical paper. [11] The papyrus describes a conservative and expectant approach to skull trauma, with better results compared with a more aggressive and less favorable approach described in Hippocratic medicine. [12]
An extensive discussion of skull fractures and their management is available in the eleventh century manuscript, "Al-Qanun Fil-Tibb" by Ibn-Sina (Avicenna). This book was a predecessor to the modern medicine literature. [13]
The 15th century management of pediatric skull fractures is illustrated by a Turkish physician of the Ottoman Empire, Serefeddin Sabuncuoğlu (1385-1468) in his textbook "Cerrahiyyetu'l Haniyye" (Imperial Surgery). [14]
Charles Bell first described occipital condylar fracture in 1817 based on an autopsy finding. [15] The same fracture was described for the first time as a radiograph finding in 1962 and by computed tomography (CT) in 1983. [1, 16]
Problem
Skull fractures are classified in the image below.
Linear skull fracture
Linear fracture results from low-energy blunt trauma over a wide surface area of the skull. It runs through the entire thickness of the bone and, by itself, is of little significance except when it runs through a vascular channel, venous sinus groove, or a suture. In these situations, it may cause epidural hematoma, venous sinus thrombosis and occlusion, and sutural diastasis, respectively. Differences between sutures and fractures are summarized in Table 1.
Table 1. Differences Between Skull Fractures and Sutures (Open Table in a new window)
Fractures |
Sutures |
|
|
Basilar skull fracture
In essence, a basilar fracture is a linear fracture at the base of the skull. It is usually associated with a dural tear and is found at specific points on the skull base.
Temporal fracture
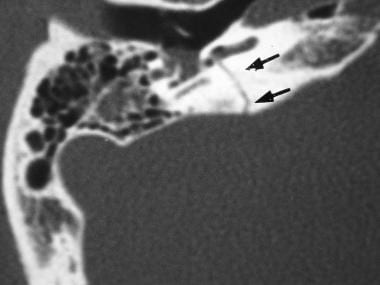
Temporal bone fracture is encountered in 75% of all skull base fractures. The 3 subtypes of temporal fractures are longitudinal, transverse, and mixed. [17] A transverse temporal bone fracture and a longitudinal temporal bone fracture are shown below.
Transverse temporal bone fracture (courtesy of Adam Flanders, MD, Thomas Jefferson University, Philadelphia, Pennsylvania)
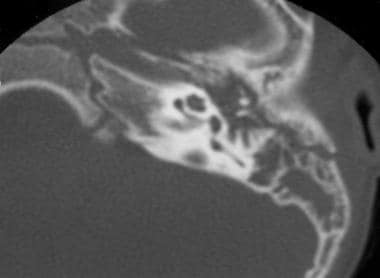 Longitudinal temporal bone fracture (courtesy of Adam Flanders, MD, Thomas Jefferson University, Philadelphia, Pennsylvania)
Longitudinal temporal bone fracture (courtesy of Adam Flanders, MD, Thomas Jefferson University, Philadelphia, Pennsylvania)
Longitudinal fracture occurs in the temporoparietal region and involves the squamous portion of the temporal bone, the superior wall of the external auditory canal, and the tegmen tympani. These fractures may run either anterior or posterior to the cochlea and labyrinthine capsule, ending in the middle cranial fossa near the foramen spinosum or in the mastoid air cells, respectively. Longitudinal fracture is the most common of the 3 subtypes (70-90%).
Transverse fractures begin at the foramen magnum and extend through the cochlea and labyrinth, ending in the middle cranial fossa (5-30%).
Mixed fractures have elements of both longitudinal and transverse fractures.
Yet another classification system of temporal bone fractures has been proposed. This system divides temporal bone fractures into petrous and nonpetrous fractures; the latter includes fractures that involve mastoid air cells. These fractures do not present with cranial nerve deficits. [2]
Occipital condylar fracture
Occipital condylar fracture results from a high-energy blunt trauma with axial compression, lateral bending, or rotational injury to the alar ligament. These fractures are subdivided into 3 types based on the morphology and mechanism of injury. [18] An alternative classification divides these fractures into displaced and stable, ie, with and without ligamentous injury. [19]
Type I fracture is secondary to axial compression resulting in comminution of the occipital condyle. This is a stable injury.
Type II fracture results from a direct blow, and, despite being a more extensive basioccipital fracture, type II fracture is classified as stable because of the preserved alar ligament and tectorial membrane.
Type III fracture is an avulsion injury as a result of forced rotation and lateral bending. This is potentially an unstable fracture.
Clivus fractures
Fractures of the clivus are described as a result of high-energy impact sustained in motor vehicle accidents. Longitudinal, transverse, and oblique types have been described in the literature. A longitudinal fracture carries the worst prognosis, especially when it involves the vertebrobasilar system. Cranial nerves VI and VII deficits are usually coined with this fracture type. [20]
Depressed skull fracture
Depressed skull fractures, as shown in the image below, result from a high-energy direct blow to a small surface area of the skull with a blunt object such as a baseball bat. Comminution of fragments starts from the point of maximum impact and spreads centrifugally. Most of the depressed fractures are over the frontoparietal region because the bone is thin and the specific location is prone to an assailant's attack. A free piece of bone should be depressed greater than the adjacent inner table of the skull to be of clinical significance and requiring elevation.
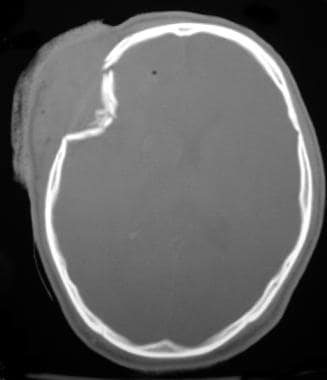 Depressed skull fracture (courtesy of Adam Flanders, MD, Thomas Jefferson University, Philadelphia, Pennsylvania)
Depressed skull fracture (courtesy of Adam Flanders, MD, Thomas Jefferson University, Philadelphia, Pennsylvania)
A depressed fracture may be open or closed. Open fractures, by definition, have either a skin laceration over the fracture or the fracture runs through the paranasal sinuses and the middle ear structures, resulting in communication between the external environment and the cranial cavity. Open fractures may be clean or contaminated/dirty.
Epidemiology
Simple linear fracture is by far the most common type of fracture, especially in children younger than 5 years. Temporal bone fractures represent 15-48% of all skull fractures, and basilar skull fractures constitute 19-21% of all skull fractures. Depressed fractures are frontoparietal (75%), temporal (10%), occipital (5%), and other (10%). Most of the depressed fractures are open fractures (75-90%). Skull fractures are currently estimated to occur in 3% of births (ie, occurring during birth). Such fractures could be due to forceps, vacuum, or even normal vaginal delivery as a result of pressure against the maternal pelvic bones. [21]
In a study (using the Pediatric Health Information System database) of 3915 patients younger than 19 years with isolated skull fractures, 78% were found to be hospitalized, and 60% of all patients were identified as male. Of the hospitalized children, 85% were discharged within 1 day, and 95% within 2 days. [22]
Etiology
In newborns, "ping-pong" depressed fractures are secondary to the baby's head impinging against the mother's sacral promontory during uterine contractions. [23] The use of forceps also may cause injury to the skull, but this is rare.
Skull fractures in infants originate from neglect, fall, or abuse. Most of the fractures seen in children are a result of falls and bicycle accidents. In adults, fractures typically occur from motor vehicle accidents or violence.
Presentation
Linear skull fracture
Most patients with linear skull fractures are asymptomatic and present without loss of consciousness. Swelling occurs at the site of impact, and the skin may or may not be breached.
Basilar skull fracture
Patients with fractures of the petrous temporal bone present with CSF otorrhea and bruising over the mastoids, ie, Battle sign. Presentation with anterior cranial fossa fractures is with CSF rhinorrhea and bruising around the eyes, ie, "raccoon eyes." Loss of consciousness and Glasgow Coma Score may vary depending on an associated intracranial pathologic condition.
Longitudinal temporal bone fractures result in ossicular chain disruption and conductive deafness of greater than 30 dB that lasts longer than 6-7 weeks. Temporary deafness that resolves in less than 3 weeks is due to hemotympanum and mucosal edema in the middle ear fossa. Facial palsy, nystagmus, and facial numbness are secondary to involvement of the VII, VI, and V cranial nerves, respectively. Transverse temporal bone fractures involve the VIII cranial nerve and the labyrinth, resulting in nystagmus, ataxia, and permanent neural hearing loss.
Occipital condylar fracture is a very rare and serious injury. [24] Most of the patients with occipital condylar fracture, especially with type III, are in a coma and have other associated cervical spinal injuries. These patients may also present with other lower cranial nerve injuries and hemiplegia or quadriplegia.
Vernet syndrome or jugular foramen syndrome is involvement of the IX, X, and XI cranial nerves with the fracture. Patients present with difficulty in phonation and aspiration and ipsilateral motor paralysis of the vocal cord, soft palate (curtain sign), superior pharyngeal constrictor, sternocleidomastoid, and trapezius.
Collet-Sicard syndrome is occipital condylar fracture with IX, X, XI, and XII cranial nerve involvement. [25, 26, 27]
Depressed skull fracture
Approximately 25% of patients with depressed skull fracture do not report loss of consciousness, and another 25% lose consciousness for less than an hour. The presentation may vary depending on other associated intracranial injuries, such as epidural hematoma, dural tears, and seizures.
-
Classification of skull fractures
-
Transverse temporal bone fracture (courtesy of Adam Flanders, MD, Thomas Jefferson University, Philadelphia, Pennsylvania)
-
Longitudinal temporal bone fracture (courtesy of Adam Flanders, MD, Thomas Jefferson University, Philadelphia, Pennsylvania)
-
Depressed skull fracture (courtesy of Adam Flanders, MD, Thomas Jefferson University, Philadelphia, Pennsylvania)
Tables
Fractures |
Sutures |
|
|









