Practice Essentials
Paraphimosis is a urologic emergency in which the retracted foreskin of an uncircumcised male cannot be returned to its normal anatomic position (see the image below). Prompt recognition and treatment of this condition is important, as it can otherwise result in gangrene and amputation of the glans penis. Prompt urologic intervention is indicated.
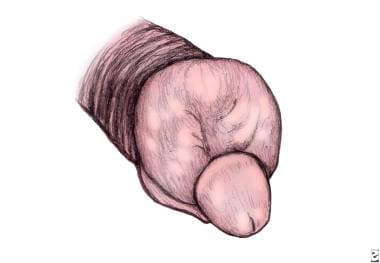 Illustration of paraphimosis. The foreskin is swollen and edematous. A constricting collar or band is present behind the glans penis.
Illustration of paraphimosis. The foreskin is swollen and edematous. A constricting collar or band is present behind the glans penis.
Paraphimosis occurs when the foreskin of an uncircumcised or partially circumcised male is retracted for an extended period of time. This causes venous occlusion, edema, and eventual arterial occlusion. The progressive edema hinders reduction of the foreskin over the glans, and the compromise of arterial flow can lead to necrosis of the glans penis.
Paraphimosis differs from phimosis, a nonemergent condition in which the foreskin cannot be retracted behind the glans penis. Paraphimosis occurs only in uncircumcised or partially circumcised males. [1]
Paraphimosis is almost always iatrogenically or inadvertently induced. It is often caused by well-meaning health professionals who have retracted the foreskin to perform penile examination or urethral instrumentation. Consequently, simple education and clarification of proper prepuce care to parents, the individuals themselves, and health care professionals may be all that is required to prevent it.
When paraphimosis is suspected, immediately obtain a urology consult for proper evaluation and diagnosis. Prompt treatment of this emergency should lead to a favorable outcome.
For patient education information, see Foreskin Problems.
Relevant Anatomy
The penis is divided into the following three parts:
-
The root of the penis lies under the pubic bone and provides stability when the penis is erect.
-
The body of the penis constitutes the major portion of the penis and is composed of two cavernosal bodies (ie, corpora cavernosa) and a corpus spongiosum (ie, head of the penis). The urethra traverses through the corpus spongiosum and exits from the meatus. The cavernosal bodies produce an erection when filled with blood.
-
The glans is the distal expansion of the corpus spongiosum usually covered by the loose skin of the prepuce in uncircumcised individuals. A collar of tissue immediately behind the glans penis is known as the coronal sulcus.
The penis is innervated by the left and right dorsal nerves (main sensory nerve supply), which are branches of the pudendal nerve.
The penis is a highly vascular organ supplied by the internal pudendal artery, which arises from the internal iliac artery and then branches into the deep penile artery, the bulbar artery, and the urethral artery.
The deep penile artery becomes the cavernosal arteries, which supply the entire corpus cavernosum. The urethral artery supplies the glans penis and the corpus spongiosum. The bulbar artery nourishes the bulbar urethra and the bulbospongiosus muscle.
Pathophysiology
When the foreskin becomes trapped behind the corona for a prolonged period, it forms a tight band of tissue around the penis. This constricting ring initially impairs venous blood and lymphatic flow from the glans penis and prepuce, in turn causing edema of the glans. As the edema worsens, arterial blood flow becomes compromised. The ensuing tissue ischemia and vascular engorgement cause painful swelling of the glans and prepuce and may eventually lead to gangrene or autoamputation of the distal penis.
Etiology
Paraphimosis can occur after retraction of the foreskin during detailed penile examination, urethral catheterization, or cystoscopy. Healthcare providers and patients need to appreciate the vital importance of replacing the foreskin to the anatomic position covering the glans, after retracting the foreskin for any intervention or examination.
Outside the medical setting, paraphimosis may develop when the individual or a parent retracts the prepuce for cleaning of the glans penis and then inadvertently leaves it in its retracted position. In most cases, the foreskin reduces on its own and therefore precludes paraphimosis; however, if the slightest resistance to retraction of the prepuce is present, leaving it in this state predisposes it to paraphimosis. As edema accumulates, the condition worsens.
Development of paraphimosis after catheterization is not uncommon. Before the insertion of a urethral catheter, health professionals retract the foreskin to sterilely prepare and drape the glans penis. The retracted foreskin may be left in that manner for several hours to days. The failure to restore the prepuce to its original position sometimes leads to the development of paraphimosis.
Paraphimosis associated with calcific uremic arteriopathy (calciphylasis) has been reported in patients with diabetes mellitius or chronic kidney disease. [2]
More unusual causes of paraphimosis include the following:
-
Placement of a preputial bead
-
Erotic dancing [7]
-
P lasmodium falciparum infection [8]
-
Contact dermatitis (eg, from the application of celandine juice to the foreskin [9] )
-
Haemophilus ducreyi infection (chancroid) [10]
-
Lichen sclerosus [11]
-
Vigorous sexual intercourse [12]
In 2022, a number of cases of paraphimosis in patients with monkeypox infection were reported. [13, 14, 15, 16]
Epidemiology
Paraphimosis is a relatively uncommon condition. It is less common than phimosis.
Paraphimosis is almost always an iatrogenically or inadvertently induced condition. Paraphimosis occurs more often in hospitals and nursing homes than in the community.
A large minority of males in the United States are uncircumcised, and thus are susceptible to paraphimosis. According to the National Hospital Discharge Survey (NHDS), circumcision rates in the US declined from an all-time high of 78-80% in the mid-to-late 1960s to 55%-60% in 2003.The NHDS found that in 2010, 58.3% of newborn boys were circumcised. Actual rates were presumably somewhat higher, however, as this figure does not include circumcisions performed in the community. [17]
Prognosis
Complications of paraphimosis include pain, infection, and swelling of the glans penis. The distal portion of the penis can become ischemic and even necrotic. [18] Penile glans necrosis is treated with partial penectomy, glansectomy, or excision of the necrotic area. [19]
Paraphimosis does not recur after a proper circumcision. Outcome after a dorsal slit procedure or a circumcision is excellent. Sometimes, patients with a favorable outcome from dorsal slit procedures decline circumcision.
-
Illustration of paraphimosis. The foreskin is swollen and edematous. A constricting collar or band is present behind the glans penis.
-
Mild-to-moderate form of paraphimosis. The treatment involves manual reduction, puncture technique, or medical therapy.
-
Severe form of paraphimosis. The distal penis has begun the process of autoamputation.
-
This demonstrates the technique of manually reducing the paraphimotic foreskin.
-
The puncture method to relieve preputial edema resulting from paraphimosis. Using a needle, several punctures are made in the foreskin to relieve the trapped fluid.







