Practice Essentials
Although prostatitis is the most common urologic diagnosis in males younger than 50 years and the third most common diagnosis in men older than 50 years (after benign prostatic hyperplasia [BPH] and prostate cancer), acute prostatitis is rare. Acute prostatitis is easier to identify than chronic prostatitis, however, because of its more uniform clinical presentation.
Acute prostatitis presents as an acute urinary tract infection (UTI). It is usually associated with predisposing risk factors, including bladder outlet obstruction secondary to BPH or an immunosuppressed state. [1] Approximately 5% of cases of acute bacterial prostatitis (ABP) progress to chronic prostatitis. [2]
Pathologic definition of prostatitis
Pathologically, prostatitis is defined as an increased number of inflammatory cells within the prostate gland. The inflammatory process may be infectious or inflammatory in origin. The most common histologic pattern is a lymphocytic infiltrate in the stroma immediately adjacent to the prostatic acini (see the image below). [3]
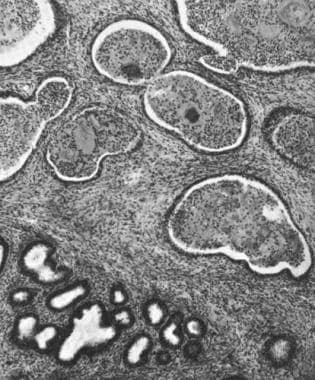 Leukocytic infiltration of the stroma and glandular lumina during acute bacterial prostatitis (ABP).
Leukocytic infiltration of the stroma and glandular lumina during acute bacterial prostatitis (ABP).
Prostatitis occurs in distinct forms that have separate causes, clinical features, and outcomes. Four clinical entities have been described: acute bacterial prostatitis, chronic bacterial prostatitis, nonbacterial or abacterial prostatitis, and prostatodynia.
NIH classification and definition of prostatitis
The National Institutes of Health (NIH) classification and definition of the categories of prostatitis are as follows:
-
Category I – Acute bacterial prostatitis (ie, acute infection of the prostate)
-
Category II – Chronic bacterial prostatitis (ie, recurrent urinary tract infection and/or chronic infection of the prostate)
-
Category III – Chronic abacterial prostatitis/chronic pelvic pain syndrome (ie, discomfort or pain in the pelvic region for at least 3 mo with variable voiding and sexual symptoms and/or no demonstrable infection; by definition, the syndrome becomes chronic after 3 mo)
-
Category IIIA – Inflammatory chronic pelvic pain syndrome (ie, white blood cells in semen and/or expressed prostatic secretions and/or third midstream bladder specimen)
-
Category IIIB – Noninflammatory chronic pelvic pain syndrome (ie, no white blood cells in semen and/or expressed prostatic secretions)
-
Category IV – Asymptomatic inflammatory prostatitis (ie, evidence of inflammation in biopsy samples, semen and/or expressed prostatic secretions, but no symptoms)
Historical and epidemiologic data
In 1978-1979, symptoms due to acute and chronic prostatitis accounted for 25% of outpatient urinary conditions in the United States. In 1985, according to Nickel, acute and chronic prostatitis accounted for more office visits than BPH or prostate cancer. Most of these visits were for chronic prostatitis. In the early 1990s, the diagnosis of prostatitis resulted in slightly more than 2 million office visits per year. [4]
The international prevalence rate of prostatitis is similar to that in the United States. In one report, of 600 men diagnosed with prostatitis, 5% had bacterial prostatitis, 64% had nonbacterial prostatitis, and 31% had pelvic-perineal pain syndrome or prostatodynia.
Relevant anatomy
The prostate is an extraperitoneal organ that encircles the neck of the bladder and urethra. In an adult, this organ is divided into four distinct zones or regions: periurethral, central, transitional, and peripheral. Prostate carcinoma arises more often in the peripheral zone than the other zones. However, the distribution of prostatic inflammation among the various zones is not clear.
A normal prostate gland is approximately 20 g in volume, 3 cm in length, 4 cm wide, and 2 cm in depth. As men get older, the prostate gland often enlarges because of BPH.
The gland is located posterior to the pubic symphysis, superior to the perineal membrane, inferior to the bladder, and anterior to the rectum. The base of the prostate is in continuity with the bladder and the prostate ends at the apex before becoming the striated external urethral sphincter. The sphincter is a vertically oriented tubular sheath that surrounds the membranous urethra and prostate.
See Prostate Anatomy for more information.
Additional Resources
For patient education information, see the Men's Health Center, as well as The Male Anatomy, and Prostate Infections (Prostatitis).
See also the following:
Pathophysiology
Theories regarding the pathogenesis of acute bacterial prostatitis include the following:
-
Intraprostatic urinary reflux
-
Ascending urethral infection
-
Direct invasion or lymphogenous spread from the rectum
-
Direct hematogenous infection
Intraprostatic urinary reflux is the most widely accepted theory. In this scenario, infected urine refluxes into the ejaculatory and prostatic ducts that empty into the posterior urethra. Because of the anatomy of the prostate gland, ducts that drain glands in the large peripheral zone are positioned more horizontally than other prostatic ducts and, thus, facilitate the reflux of urine into the prostate. Consequently, most infections occur in the peripheral zone.
In younger men, ascending urethral infection may occur following sexual intercourse. Meatal inoculation may occur during unprotected anal intercourse, instrumentation, and prolonged catheterization.
Etiology
The organisms primarily responsible for acute bacterial prostatitis (ABP) are also those responsible for most urinary tract infections; these include gram-negative members of the Enterobacteriaceae family such as Escherichia coli, Proteus mirabilis, Klebsiella species, Enterobacter species, Pseudomonas aeruginosa, and Serratia species. Of these, E coli is involved most often and has been shown to increase biofilm formation. [5] Most prostatic infections (82%) involve only a single bacterial organism. In some cases, two or three strains of bacteria may be involved.
Obligate anaerobic bacteria and gram-positive bacteria other than enterococci rarely cause acute bacterial prostatitis. Enterococci account for 5-10% of documented prostate infections. [6] Staphylococcus aureus infection due to prolonged catheterization may occur in the hospital. Other occasional causative organisms include Neisseria gonorrhoeae,Mycobacterium tuberculosis,Salmonella species, Clostridium species, and parasitic or mycotic organisms. N gonorrhoeae should be suspected in sexually active men younger than 35 years.
If recurrent urinary tract infections are confirmed, patients need to be evaluated for any structural abnormality.
Prostate biopsy
Another source of acute prostatitis is following transrectal ultrasound-guided prostate needle biopsy. In this instance, the acute prostatitis is iatrogenic in nature but presents similarly and is treated as acute bacterial prostatitis. In a French study, acute bacterial prostatitis occurred 1–7 days after 21-core prostate biopsy in 20 of 3000 patients (0.67%). All the patients had received fluoroquinolone prophylaxis, but on antibiotic susceptibility testing, 95% of samples were resistant to fluroquinolones and amoxicillin. Escherichia coli was the only bacterium isolated. [7]
A study comparing the multiresistant ST131 E coli pathogen found after transrectal ultrasound-guided prostate biopsy to non-ST131 E coli from patients with spontaneous urosepsis showed that the ST131 E coli had fewer virulence-associated genes than the non-ST131 group. The finds suggest that antimicrobial resistance, rather than virulence genotype, is the most important trait associated with an increased risk of infection following transrectal biopsy. [8]
Risk factors
The following are risk factors for acute bacterial prostatitis (all allow bacterial colonization):
-
Intraprostatic ductal reflux
-
Phimosis and redundant foreskin
-
Specific blood groups [9]
-
Unprotected anal intercourse
-
Urinary tract infections
-
Acute epididymitis
-
Indwelling Foley catheter and condom catheter
-
Transurethral surgery
-
Altered prostatic secretions
-
Recent transrectal ultrasound-guided prostate needle biopsy
In the pediatric population, acute bacterial prostatitis has been associated with septicemic seeding, abnormal bladder dysfunction, congenital abnormalities of the ureter, and sexual abuse. A case report describes acute bacterial prostatitis in an adolescent after blunt trauma to the lower abdomen. [10]
Prognosis
If the initial response to medical therapy for acute bacterial prostatitis is favorable, the patient's prognosis is very good. Decreased fertility has been reported, but only in cases of massive bacterial inoculation. Decreased sperm viability, including impaired motility and agglutination, has been reported in samples that contained more than 106 colony-forming units (CFU)/mL of bacteria.
Prostatic abscess is an uncommon but well-described complication of acute bacterial prostatitis. Although very rare, it usually occurs in patients who are immunocompromised, who have diabetes, who have urethral instrumentation or a prolonged indwelling urethral catheters, or who are on maintenance dialysis. Coliform bacteria, especially E coli, cause more than 70% of prostatic abscesses.
Other potential sequelae of acute bacterial prostatitis include progression to chronic prostatitis, septicemia, pyelonephritis, and epididymitis. Nearly 10% of patients with acute bacterial prostatitis develop chronic prostatitis and another 10% develop chronic pelvic pain syndrome. [11]
-
Leukocytic infiltration of the stroma and glandular lumina during acute bacterial prostatitis (ABP).








