Practice Essentials
Lower gastrointestinal bleeding (LGIB) is a frequent cause of hospital admission and is a factor in hospital morbidity and mortality. LGIB is distinct from upper GI bleeding (UGIB) in epidemiology, management, and prognosis. The image below illustrates the different types of LGIB.
Signs and symptoms
The clinical presentation of LGIB varies with the anatomical source of the bleeding, as follows:
-
Maroon stools, with LGIB from the right side of the colon
-
Bright red blood per rectum with LGIB from the left side of the colon
-
Melena with cecal bleeding
In practice, however, patients with UGIB and right-sided colonic bleeding may also present with bright red blood per rectum if the bleeding is brisk and massive.
The presentation of LGIB can also vary depending on the etiology. A young patient with infectious or noninfectious (idiopathic) colitis may present with the following:
-
Fever
-
Dehydration
-
Abdominal cramps
-
Hematochezia
An older patient with diverticular bleeding or angiodysplasia may present with painless bleeding and minimal symptoms. Ischemic colitis, abdominal pain, and varying degrees of bleeding are usually observed in patients with multiple comorbidities such as congestive heart failure (CHF), atrial fibrillation, or chronic renal failure (CRF). LGIB can be mild and intermittent, as often is the case of angiodysplasia and colon carcinoma, or moderate or severe, as may be the situation in diverticula-related bleeding. Colon carcinoma rarely causes significant LGIB.
Massive LGIB usually occurs in patients aged 65 years and older who have multiple medical problems, and it produces the following manifestations:
-
Systolic blood pressure of less than 90 mm Hg
-
Hemoglobin (Hb) level of 6 g/dL or less
-
The passage of maroon stools or bright red blood from the rectum
See Presentation for more detail.
Diagnosis
Nonsurgical modalities used to diagnose LGIB include the following:
-
Radionuclide scans
-
Angiography
Fiberoptic flexible colonoscopy is the initial diagnostic method of choice in most patients who are hemodynamically stable. Colonoscopy should be performed following a rapid bowel preparation (“prep”) with volume cathartic agents. Rapid bowel prep colonoscopy has higher diagnostic and therapeutic yields compared to unprepped colonoscopic evaluation. In hemodynamically unstable patients and in those with brisk ongoing LGIB, angiography with or without a preceding radionuclide scan can be performed. Angiography is also performed if colonoscopy has failed to identify a bleeding site. Rarely, exploratory laparotomy and intraoperative push enteroscopy can be performed in truly hemodynamically unstable patients owing to the speed and the volume of the bleeding.
Appropriate routine blood tests include the following:
-
Complete blood cell (CBC) count
-
Serum electrolytes levels (eg, sequential multiple analysis 7 [SMA7])
-
Coagulation profile, including activated partial thromboplastin time (aPTT), prothrombin time (PT), platelet count, and/or bleeding time (bleeding time is only recommended in patients with bleeding disorders and in those using antiplatelet agents)
Helical computed tomography (CT) scanning of the abdomen and pelvis can be used when a routine workup fails to determine the cause of active GI bleeding. Multiple criteria are used for establishing the bleeding site, including the following [1, 2] :
-
Vascular extravasation of the contrast medium
-
Contrast enhancement of the bowel wall
-
Thickening of the bowel wall
-
Spontaneous hyperdensity of the peri-intestinal fat
-
Vascular dilatations
Patients who have experienced multiple episodes of LGIB without a known source or diagnosis should undergo the following:
-
Elective mesenteric angiography
-
Upper and lower endoscopy
-
Meckel scanning
-
Upper GI imaging series with small bowel assessment
-
Enteroclysis
See Workup for more detail.
Management
The management of LGIB has three components, as follows:
-
Resuscitation and initial assessment
-
Localization of the bleeding site
-
Therapeutic intervention to stop bleeding at the site
Resuscitation and initial assessment
Initial resuscitation involves establishing large-bore intravenous (IV) access and administration of normal saline. The patient's blood loss and hemodynamic status should be ascertained and, in cases of severe bleeding, the patient may require invasive hemodynamic monitoring to direct therapy.
Hemostasis
Once the bleeding site is localized, nonsurgical therapeutic options that may be considered include the following:
-
Diverticular bleeding: Colonoscopy with bipolar probe coagulation, epinephrine injection, or metallic clips
-
Recurrent bleeding: Resection of the affected bowel segment
-
Angiodysplasia: Thermal therapy (eg, electrocoagulation, argon plasma coagulation)
-
Conservative management, including nothing by mouth (NPO) and IV hydration in patients with ischemic colitis
In patients in whom the bleeding site cannot be determined, vasoconstrictive agents such as vasopressin (Pitressin) can be used. If vasopressin is unsuccessful or contraindicated, superselective embolization is useful.
Surgery
Indications for surgery include the following:
-
Active persistent bleeding with hemodynamic instability that is refractory to aggressive resuscitation
-
Persistent, recurrent bleeding
-
Transfusion of more than 4 units of packed red blood cells (PRBCs) in a 24-hour period, with active or recurrent bleeding
-
Transfusion of more than 6 units of PRBCs during the same hospitalization
See Treatment and Medication for more detail.
Background
Lower gastrointestinal bleeding (LGIB) accounts for approximately 20%-33% of episodes of gastrointestinal (GI) hemorrhage, with an annual incidence of about 20-27 cases per 100,000 population in Western countries. However, although LGIB is statistically less common than upper GI bleeding (UGIB), it has been suggested that LGIB is underreported because a higher percentage of affected patients do not seek medical attention. [3] Indeed, LGIB continues to be a frequent cause of hospital admission and is a factor in hospital morbidity and mortality, particularly among elderly patients. [4] LGIB is distinct from UGIB in epidemiology, management, and prognosis. [5]
LGIB encompasses a wide spectrum of symptoms/signs, ranging from relatively trivial hematochezia to massive hemorrhage with shock. [6] Acute LGIB has been defined as bleeding that is of recent duration, originates beyond the ligament of Treitz, results in instability of vital signs, and is associated with signs of anemia with or without the need for blood transfusion. The definition of LGIB from the American College of College of Gastroenterology clinical guideline is "the onset of hematochezia originating from either the colon or the rectum." [5]
LGIB is generally classified under three groups according to the amount of bleeding, as shown in the image below. Massive hemorrhage is a life-threatening condition [4] and requires transfusion of at least 4 units (U) of blood within 1 hour.
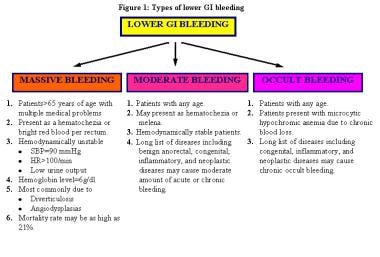 Types of lower gastrointestinal (GI) bleeding. HR = heart rate, SBP = systolic blood pressure.
Types of lower gastrointestinal (GI) bleeding. HR = heart rate, SBP = systolic blood pressure.
Massive LGIB is defined as follows:
Note the following:
-
Passage of a large volume of red or maroon blood through the rectum
-
Hemodynamic instability and shock
-
Initial decrease in hematocrit (Hct) level of 6 g/dL or less
-
Transfusion of at least 4 U of packed red blood cells (PRBCs)
-
Bleeding that continues for 3 days
-
Significant rebleeding in 1 week
LGIB has a mortality rate ranging from about 10% to 20%, with risk factors for poor outcomes including creatinine levels above 150 μM, initial hematocrit level below 35%, patients of advanced age (>60 y), abnormal vital signs after 1 hour, and gross blood on initial rectal examination. [5] Patients with comorbid conditions (eg, multiorgan system disease, transfusion requirements in excess of 5 U, need for operation, and recent stress, such as surgery, trauma, and sepsis) are also at great risk for poor outcomes. LGIB is more likely in the elderly because of a higher incidence of diverticulosis and vascular disease in these groups. The incidence of LGIB is higher in men than in women.
Advances in diagnostic and therapeutic colonoscopy and in interventional angiography have resulted in a shift away from the need for surgical treatment (see the image below). Effective management with less invasive modalities has also reduced healthcare costs and, more importantly, patient morbidity and mortality.
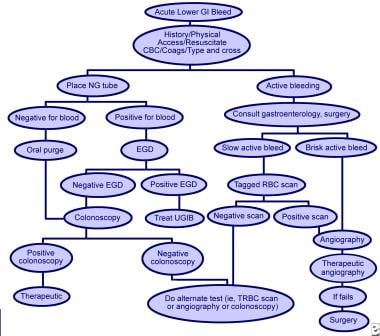 Methods used to treat lower gastrointestinal (GI) bleeding. CBC = complete blood cell count, coags = coagulation studies, EGD = esophagogastroduodenoscopy, NG = nasogastric, RBC = red blood cell, TRBC = tagged RBC, UGIB = upper GI bleeding.
Methods used to treat lower gastrointestinal (GI) bleeding. CBC = complete blood cell count, coags = coagulation studies, EGD = esophagogastroduodenoscopy, NG = nasogastric, RBC = red blood cell, TRBC = tagged RBC, UGIB = upper GI bleeding.
Historical details
Understanding of the pathogenesis, diagnosis, and treatment of LGIB has drastically changed during the last 50 years. In the first half of the 20th century, large intestinal neoplasms were believed to be the most common cause of LGIB. In the 1950s, this condition was commonly attributed to diverticulosis; surgical treatment consisted of blind segmental bowel resections, with disappointing results. Patients who underwent these procedures suffered from a prohibitively high rebleeding rate (up to 75%), morbidity (up to 83%), and mortality (up to 60%).
Over several decades, diagnostic methods for locating the precise bleeding point greatly improved. The flexible endoscope was developed in 1954. The full-length colonoscope was developed in 1965 in Japan. Also in 1965, Baum et al described selective mesenteric angiography, which permitted the identification of vascular abnormalities and the precise bleeding point. [7] The first anal colonoscopy was performed in 1969.
Experience with mesenteric angiography in the late 1960s and 1970s suggested that angiodysplasias and diverticulosis were the most common reasons for LGIB. Since its discovery, mesenteric angiography remains the criterion standard in precise localization of the bleeding site.
Rosch et al described superselective visceral arteriography for infusion of vasoconstrictors in 1971 and superselective embolization of the mesenteric vessels as an alternative technique to treat massive LGIB in 1972. [8, 9] The most feared complication of embolization of the mesenteric vessels is ischemic colitis, which has limited its use in GI bleeding.
The initial experience with vasopressin infusion was reported in 1973-1974. Vasopressin causes vasoconstriction and arrests the bleeding in 36%-100% of patients. The recurrence rate following completion of vasopressin infusion can be as high as 71%; therefore, vasopressin is used to temporize the acute event and to stabilize patients before surgery.
Endoscopic control of bleeding with thermal modalities or sclerosing agents has been in use since the 1980s. One of the advantages of upper (or lower) endoscopic evaluation is that it provides a means to administer therapy in patients with GI bleeding. Nuclear scintigraphy has been used since the early 1980s as a very sensitive diagnostic tool to evaluate bleeding from the GI tract; this modality can detect hemorrhage at rates as low as 0.1 mL/min.
Key points
Note the following:
-
The physical examination should be thorough and include the skin, oropharynx, nasopharynx, abdomen, perineum, and anorectum. Therefore, nasogastric tube insertion, digital rectal examination, and anoscopy/proctoscopy should be part of the initial physical examination in all patients.
-
In most patients with LGIB, colonoscopy is the initial diagnostic method of choice. Colonoscopy is successfully used to identify the site of severe LGIB in approximately 80%-90% of patients.
-
Nuclear scintigraphy is a sensitive diagnostic tool and can detect hemorrhage at rates as low as 0.1 mL/min (0.1-0.5 mL/min), as opposed to angiography, which detects bleeding at rates of 1-1.5 mL/min.
-
Because of the high false-localization rate (10%-60%) for the bleeding site, performing segmental resections based solely on scintigraphy results is not recommended unless an immediate blush can be identified at the start of the study.
-
Emergency angiography as an initial study is indicated in a highly select group of patients with massive ongoing LGIB.
-
Segmental bowel resection following precise localization of the bleeding point is the preferred treatment because of its low postoperative morbidity and mortality when compared with subtotal colectomy.
-
Subtotal (total abdominal) colectomy with temporary end ileostomy is the procedure of choice in patients who are actively bleeding from an unknown source.
-
Blind segmental resection should not be performed because of a prohibitively high rebleeding rate, morbidity, and mortality rate.
For patient education information, see Digestive Disorders Center, as well as Gastrointestinal Bleeding (GI Bleeding), Rectal Bleeding, Inflammatory Bowel Disease (IBD), Diverticulitis and Diverticulosis, and Anal Abscess.
Anatomy
The average length of the large intestine is 135-150 cm. Ascending and descending segments of the colon are fixed to the retroperitoneum. However, the transverse and sigmoid colon are supported by a mesentery. A comprehensive understanding of the small bowel and colonic vascular anatomy is essential for any physician performing a primary lower gastrointestinal procedure for hemorrhage or other conditions.
The ileocolic, right colic, and middle colic branches of the superior mesenteric artery supply blood to the cecum, ascending, and proximal transverse colon, respectively. The superior mesenteric vein drains the right side of the colon, joining the splenic vein to form the portal vein. The inferior mesenteric artery supplies blood to the distal transverse, descending, and sigmoid colon. The inferior mesenteric vein carries blood from the left side of the colon to the splenic vein. A rich network of vessels from the superior, middle, and inferior hemorrhoidal vessels supplies the rectosigmoid junction and rectum.
Pathophysiology
Diverticulosis, angiodysplasia, colitis, carcinoma, and anorectal disease play roles in the pathophysiology of lower gastrointestinal bleeding (LGIB). [6, 10] They are briefly discussed in this section.
Diverticulosis
Diverticulosis is a common acquired condition in Western societies; approximately 50% of adults older than 60 years have radiologic evidence of this disease. A diverticulum is a saclike protrusion of the colonic wall that develops at a small point of weakness where the penetrating vessel has perforated through the circular muscle fibers. The vessel becomes draped over the dome of the diverticulum, separated from the bowel lumen only by the mucosa. Subsequent chronic trauma to the vasa recta along the luminal aspect, as well as contraction and relaxation of the surrounding muscularis propria, leads to an eccentric thinning of the media. Ultimately, erosion of the vessel and bleeding can occur.
Diverticula are most commonly located in the sigmoid and descending colon, and diverticular bleeding originates from vasa rectae located in the submucosa, which can rupture at the dome or the neck of the diverticulum. [11] Up to 20% of patients with diverticular disease experience bleeding, which stops spontaneously in 80% of patients; however, in 5% of patients with diverticular disease, the bleeding from diverticular disease can be massive.
Although about 75% of the diverticula occur on the left side of the colon, right-sided diverticula are responsible for approximately 50%-90% of the bleeding. [11] This may be because false right-sided diverticula have wider necks and domes, which expose the vasa recta to injury over a greater length. The incidence of true right-sided diverticula is uncommon (1%-2%) in the United States, unlike in Asian populations. True right-sided diverticula are usually solitary and originate in the anterior cecum adjacent to the ileocecal valve. Often, true right-sided diverticula cause right-sided diverticulitis and are misdiagnosed as appendicitis.
Angiodysplasia
Colonic angiodysplasias are arteriovenous malformations (AVMs) located in the cecum and ascending colon; these are acquired lesions that affect elderly persons older than 60 years. Most colonic angiodysplasias are degenerative lesions that arise from chronic, intermittent, low-grade colonic contraction that obstructs the mucosal venous drainage. Over time, mucosal capillaries dilate, become incompetent, and form an AVM.
Colitis
Massive hemorrhage due to inflammatory bowel disease (IBD) is rare. Ulcerative colitis causes bloody diarrhea in most cases. In up to 50% of patients with ulcerative colitis, mild to moderate LGIB occurs, and approximately 4% of patients with ulcerative colitis have massive hemorrhage.
LGIB in patients with Crohn disease is not as common as in patients with ulcerative colitis; 1%-2% of patients with Crohn disease may experience massive bleeding. The frequency of bleeding in patients with Crohn disease is significantly more common with colonic involvement than with small bowel involvement alone. The mucosal pattern of injury is similar to that found in patients with infectious and ischemic colitis, with the mucosa appearing friable, erythematous, edematous, and ulcerated. In severe Crohn disease, the inflammatory process may extend into the serosa, leading to colonic perforation.
Ischemic colitis is a disease of the elderly population and is commonly observed after the sixth decade of life. This condition is the most common form of ischemic injury to the digestive system, frequently involves the watershed areas, including the splenic flexure and the rectosigmoid junction. Ischemia causes mucosal and partial-thickness colonic wall sloughing, edema, and bleeding. In most cases, the precipitating event cannot be identified. However, although abdominal pain and bloody diarrhea are the main clinical manifestations, ischemic colitis is not associated with significant blood loss or hematochezia.
The pathophysiologic mechanism of infectious colitis may be due to either colonic tissue invasion by bacteria, such as Salmonella and Shigella, or toxin-mediated damage, as with Escherichia coli 0157:H7.
Colon carcinoma
Colorectal adenocarcinoma is the third most common cancer in the United States for men and women. [12] Colorectal carcinoma causes occult bleeding as a result of mucosal ulceration or erosion, but the incidence of massive bleeding due to colorectal carcinoma varies from 5% to 20% in different case series.
Other diseases
Benign anorectal disease (eg, hemorrhoids, anal fissures, anorectal fistulas) can cause intermittent rectal bleeding. Massive rectal bleeding due to benign anorectal disease has also been reported. A review of the Department of Veterans Affairs (VA) database revealed that 11% of patients with LGIB had hemorrhage from anorectal disease. [13]
Postpolypectomy hemorrhage is reported to occur in 0.1%-3% of patients up to 1 month following colonoscopic polyp resection.
Various small intestinal conditions, such as Crohn disease, Peutz-Jeghers syndrome, hemangiomas, and small intestinal adenocarcinomas, may cause small intestinal bleeding, but these hemorrhages are usually occult in nature.
Etiology
Comprehensive knowledge of the etiology of lower gastrointestinal bleeding (LGIB) is essential for patient management and, ultimately, for patient outcome. Colorectal polyps/neoplasms, Dieulafoy lesion, inflammatory bowel disease (IBD), and anorectal conditions are the most common etiologies of acute severe LGIB.
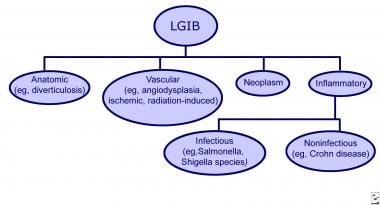
The diagram below provides an outline of the most common causes of LGIB, including anatomic (eg, diverticular bleeding), vascular (eg, angiodysplasia, ischemic colitis, radiation-induced colitis), neoplasms, and inflammatory.
In a retrospective review of medical records from approximately 1100 patients with acute LGIB, all of whom were admitted to the surgical service of a single urban emergency hospital, Gayer et al determined that the most common etiologies for bleeding in these patients were diverticulosis (33.5%), hemorrhoids (22.5%), and carcinoma (12.7%). [14] The investigators also found that most patients in the study (55.5%) presented with hematochezia, with the next most frequent presentations being maroon stools (16.7%) and melena (11%).
In a review by Vernava and colleagues, patients with LGIB made up only 0.7% of all hospital admissions (17,941 patients); among the patients who underwent a diagnostic workup (4410 [24%]), the most common causes of bleeding were diverticular disease (60%), IBD (13%), and anorectal diseases (11%) (see Table 1 below). [13] These figures differ somewhat from the study by Gayer et al. Although some publications have reported arteriovenous malformations (AVMs) as a common cause of LGIB, Vernava et al reported the true incidence of these lesions at 3%. [15]
Table 1. Common Causes of Lower Gastrointestinal Bleeding in Adults (Open Table in a new window)
Lower Gastrointestinal Bleeding in Adults |
Patients (%) |
Diverticular disease
|
60% |
Inflammatory bowel disease
|
13% |
Benign anorectal diseases
|
11% |
Neoplasia
|
9% |
Coagulopathy |
4% |
Arteriovenous malformations (AVMs) |
3% |
TOTAL |
100% |
Source: Vernava AM, Longo WE, Virgo KS. A nationwide study of the incidence and etiology of lower gastrointestinal bleeding. Surg Res Commun. 1996;18:113-20. [13] |
|
Longstreth reviewed the discharge summary and colonoscopy data from a large health maintenance organization with members in the San Diego, California, area; of 235 hospital admissions for 219 patients, the estimated hospital admission rate for LGIB was found to be 20 patients per 100,000 admissions, with bleeding from diverticular disease the most common reason (42%), followed by colorectal malignancies (9%) and ischemic colitis (8.7%). [16] The incidence of LGIB due to colonic angiodysplasias was 6%. These findings were consistent with those of the Veterans Administration database study by Vernava et al, although that study was limited to males.
The common causes of LGIB in infants, children, and adolescents differ from those found in adults. Meckel diverticulum, intussusception, polyposis syndromes, and IBD are the common causes in this population (see Table 2 below).
Table 2. Common Causes of Lower Gastrointestinal Bleeding in Children and Adolescents (Open Table in a new window)
Lower Gastrointestinal Bleeding in Children and Adolescents |
Intussusception |
Polyps and polyposis syndromes
|
Inflammatory
|
Meckel diverticulum |
Diverticulosis
Diverticulosis is the dominant etiology of LGIB, reported as the most common reason for massive LGIB in most single-institution publications. Most diverticular bleeding occurs without concomitant diverticulitis, and diverticulitis does not increase the risk of bleeding. Risk factors for diverticular bleeding include lack of dietary fiber, constipation, advanced age, and the use of nonsteroidal anti-inflammatory drugs (NSAIDs) and aspirin.
Angiodysplasia
Angiodysplasia is by far the most common vascular anomaly found in the GI tract. Although the lesions can occur anywhere in the GI tract, they occur most often in the proximal colon. Because bleeding from angiodysplasia is venocapillary in origin, it is generally less vigorous than diverticular bleeding. However, in contrast to diverticular bleeding, about 80% of patients with resolved but untreated angiodysplasia bleeding experience rebleeding. [17]
Saperas et al found that earlier bleeding with a high bleeding rate, overanticoagulation, and multiple angiodysplastic lesions predict an increased risk of recurrent bleeding due to angiodysplasia. [18] The investigators also noted that although there was a better trend for management and prevention of such recurrent bleeding with endoscopic argon plasma coagulation, this therapy was not predictive of a lower rate of hemorrhage recurrence. [18]
Angiodysplasia is believed to be associated with a number of medical conditions, including aortic stenosis, von Willebrand disease, and chronic renal failure. The incidence of angiodysplasia increases with age owing to the degeneration of the vascular walls. Angiodysplasia was previously believed to be associated with the presence of aortic stenosis, but data supporting this relationship are lacking.
Ischemic and radiation-induced colitis and other vascular causes
Ischemic colitis is rarely a cause of significant blood loss; thus, large-volume or brisk bleeding should prompt a search for an alternate etiology. Tissue injury is typically caused by hypotension and vasoconstriction, which leads to mucosal friability and endoscopic findings often resembling the changes of IBD. Ischemic colitis usually involves the left side of the colon with rectal sparing. Elderly patients with comorbidities, such as heart failure and arrhythmia, are more susceptible.
Radiation therapy can cause inflammatory changes in the bowel resulting in mucosal telangiectasias that bleed. When this treatment is used for abdominal and pelvic cancers, bleeding due to mucosal damage in the colon can lead to complications of acute colitis or ulceration. Complications can occur early or late, with a median time of occurrence from 9 to 15 months. Risk factors for radiation-induced LGIB include arteriosclerosis and concomitant chemotherapy.
Other vasculitic entities, such as polyarteritis nodosa and Wegener granulomatosis, can also cause LGIB because of the underlying necrotic process that causes sloughing of the mucosa. Bleeding may also occur secondary to immunosuppressive therapy, which can cause thrombocytopenia. Aortocolonic fistulas, which rarely develop after aortic-graft surgery, can cause LGIB as long as 10-20 years after surgery.
Infectious colitis
The most common infectious causes of colitis worldwide are Salmonella, Shigella, Campylobacter jejuni, E coli 0157:H7, and Entamoeba histolytica. In the United States, Salmonella, Shigella, and Campylobacter are the most common causative pathogens; such microbial agents cause an inflammatory diarrhea characterized by fever, bloody diarrhea, lower quadrant cramps, and tenesmus.
Noninfectious (idiopathic) colitis
Although IBD due to Crohn disease or ulcerative colitis causes LGIB, it is rarely a massive hemorrhage. Ulcerative colitis can cause mild to moderate bloody diarrhea in about 50% of patients, with an estimated 4% of patients experiencing massive bleeding. In Crohn disease, massive bleeding is less common, occurring in about 2% of patients with Crohn colitis.
Neoplasm
Neoplastic bleeding can be from a polyp or carcinoma. Colon cancer is the predominant cause of neoplastic bleeding and is responsible for around 10% of rectal bleeding in patients older than 50 years. The bleeding is usually low grade and recurrent, occurring as a result of mucosal ulceration or erosion. Although neoplastic bleeding can present as bright red blood per rectum, it is unusual for it to cause massive colonic bleeding.
Postpolypectomy bleeding occurs in approximately 0.1%-3% of patients, is more often arterial, and can produce significant bleeding. Bleeding can occur at the time of polypectomy, but it can also manifest several hours to a few weeks after the procedure.
Anorectal disease
Anorectal diseases, such as hemorrhoids, fistulas, and fissures, typically cause intermittent rectal bleeding.
Other causes of LGIB
Infection with human immunodeficiency virus (HIV) is an infrequent cause of LGIB. Most of the LGIB in such cases is caused by HIV-related opportunistic infections and associated etiologies, including cytomegalovirus (CMV) colitis, idiopathic colon ulcers, Kaposi sarcoma, and lymphoma. [19] Patients with HIV can also bleed from hemorrhoids and anal fissures, in which situations there is an increased likelihood of bleeding due to concomitant coagulopathy.
Drug-induced bleeding is caused mainly by NSAID and aspirin use, and it is more common in the elderly. Although the risk of bleeding increases at higher doses of these agents, even low-dose aspirin given for cardiovascular prophylaxis can produce bleeding. Using the lowest effective dose for both short and long-term users is recommended. [20] Aspirin or anticoagulants can potentiate or aggravate hemorrhage from preexisting lesions. Oral anticoagulants, antiplatelet agents, and NSAIDs should be used with caution in patients at risk of GIB. [5]
Benign small intestinal neoplasms are usually asymptomatic, but up to 10% may cause small intestinal bleeding. Small intestinal adenomatous polyps, leiomyomas, Peutz-Jeghers syndrome, and hemangiomas may cause occult or frank LGIB.
Other uncommon causes of LGIB include stercoral ulcers.
Epidemiology
Lower gastrointestinal bleeding (LGIB) that requires hospitalization represents less than 1% of all hospital admissions in the United States. [13] In one study, the estimated annual incidence rate was 20.5 patients per 100,000 (24.2 in males vs 17.2 in females); however, in individuals in the third to the ninth decades of life, the incidence rate of LGIB increased more than 200-fold. [16] LGIB is somewhat more common in men than in women, because diverticulosis and vascular disease are more common in men. [5]
Worldwide, acute LBIG accounts for 1%-2% of hospital emergencies, with 15% of these presenting as massive bleeding and about 5% requiring operative intervention. [21] The small bowel represents 5% of all LGIB bleeding sites, but it is the most common site of obscure bleeding. [21, 22]
The leading causes of significant LGIB are diverticulosis and angiodysplasia. [6, 10] Colonic diverticular disease is the most common cause of LGIB. [23] Diverticulosis accounts for around 30%-50% of the cases of hemodynamically significant LGIB, whereas angiodysplasia accounts for about 20%-30% of cases. LGIB is more common in the elderly than in younger people, because diverticulosis and vascular disease are more common in these groups. Some experts believe that angiodysplasia is the most frequent cause of LGIB in patients older than 65 years.
Hemorrhoids are the most common cause of LGIB in patients younger than 50 years, but the bleeding is usually minor and it is rarely the cause of significant LGIB. According to a review of seven series of patients with LGIB, the most common cause of LGIB was diverticulosis, accounting for approximately 33% of cases, followed by cancer and polyps, which accounted for about 19% of cases. [24]
Prognosis
Lower gastrointestinal bleeding ranges from relatively trivial hematochezia to massive hemorrhage with shock, and it accounts for up to 24% of all cases of GI bleeding. This condition is associated with significant morbidity and mortality (10%-20%). Patients of advanced age and patients with comorbid conditions are at the greatest risk. [4] Identification of the bleeding site is the most important initial step in treatment; once the bleeding point is localized, the treatment options are generally straightforward and curative.
The evolution of more sophisticated diagnostic imaging (eg, angiography, bleeding scanning, flexible fiberoptic colonoscopy) offers the promise of precise localization of the bleeding site. These advances also provide nonoperative and less invasive control of bleeding using angiographic techniques or colonoscopy. Pharmacologic discoveries are also improving patient care and outcome. Therefore, the therapeutic armamentaria have expanded greatly in the last several decades.
-
Types of lower gastrointestinal bleeding (LGIB).
-
Methods used to treat lower gastrointestinal (GI) bleeding. CBC = complete blood cell count, coags = coagulation studies, EGD = esophagogastroduodenoscopy, NG = nasogastric, RBC = red blood cell, TRBC = tagged RBC, UGIB = upper GI bleeding.
-
Types of lower gastrointestinal (GI) bleeding. HR = heart rate, SBP = systolic blood pressure.
-
Algorithm for massive lower gastrointestinal (GI) bleeding, surgical perspective. EGD = esophagogastroduodenoscopy; NG = nasogastric; 99mTc RBC = technetium-99m pertechnetate–labeled autologous RBC.
Tables
Lower Gastrointestinal Bleeding in Adults |
Patients (%) |
Diverticular disease
|
60% |
Inflammatory bowel disease
|
13% |
Benign anorectal diseases
|
11% |
Neoplasia
|
9% |
Coagulopathy |
4% |
Arteriovenous malformations (AVMs) |
3% |
TOTAL |
100% |
Source: Vernava AM, Longo WE, Virgo KS. A nationwide study of the incidence and etiology of lower gastrointestinal bleeding. Surg Res Commun. 1996;18:113-20. [13] |
|
Lower Gastrointestinal Bleeding in Children and Adolescents |
Intussusception |
Polyps and polyposis syndromes
|
Inflammatory
|
Meckel diverticulum |

What would you like to print?
- Overview
- Presentation
- DDx
- Workup
- Treatment
- Approach Considerations
- Resuscitation and Initial Assessment
- Localization of the Bleeding Site
- Initial Approach to Hemostasis
- Therapeutic Colonoscopy
- Vasoconstrictive Therapy
- Superselective Embolization
- Endoscopic Therapies
- Emergent Surgery
- Preoperative Details
- Intraoperative Details
- Postoperative Details
- Complications of Lower GI Bleeding
- Transfusion-Free Management of Lower GI Bleeding
- Long Term Monitoring
- Show All
- Guidelines
- Medication
- Questions & Answers
- Media Gallery
- Tables
- References






