Practice Essentials
Metastatic tumors of the omentum are common. In contrast, primary tumors of the omentum are very rare, [1] and the etiologic agents responsible for causing them are unknown.
The most common presentations of solid omental tumors include the following:
-
Abdominal discomfort
-
Abdominal mass
-
Abdominal distention
In addition to standard preoperative laboratory studies, workup may include the following:
-
Ultrasonography (US) - This is the first-line screening imaging study; it can indicate the presence of a mass in the midabdomen and can differentiate cystic from solid tumors but usually cannot identify the primary site and tumor characteristics
-
Computed tomography (CT) - This is the imaging study of choice in helping to diagnose omental tumors; it provides anatomic details and can usually identify the primary site, and it may also demonstrate displacement or compression on adjacent organs
-
Magnetic resonance imaging (MRI) - MRI can aid in differentiating cystic from solid tumors but is more time-consuming and expensive than other imaging modalities
-
Positron emission tomography (PET) - When a gastrointestinal (GI) stromal tumor (GIST) is suspected, this can complement contrast CT in helping to differentiate benign from malignant tissue and necrotic scar from active tumor; baseline PET is recommended before initiation of imatinib therapy
-
Angiography - Angiography can be helpful with a suspected omental tumor; knowledge of the vascular structures supplying the greater omentum helps in diagnosing these tumors
Needle biopsy has been controversial.
Complete surgical excision offers the best chance of cure. The role of adjuvant therapy in the management of malignant omental tumors is uncertain. Because of the rarity of these lesions, the effectiveness of chemotherapy and radiation therapy has not been established. Advances in these treatment modalities may improve future survival rates for patients with malignant primary omental tumors.
Anatomy
The greater omentum, where most omental tumors are located, is composed of a double layer of peritoneum extending from the greater curvature of the stomach toward the pelvis anterior to the small intestine before folding over itself and the transverse colon. The left margin is continuous with the gastrosplenic ligament; the right margin extends to the proximal duodenum. Consequently, tumors arising from the greater omentum generally displace the stomach upward and the transverse colon downward.
The normal omentum is thin and mainly composed of fat; therefore, it is usually not visualized on US or CT unless it is pathologically involved. Knowledge of the anatomic relations between the greater omentum and surrounding structures (see the image below) is essential for accurate diagnosis and safe resection of omental tumors.
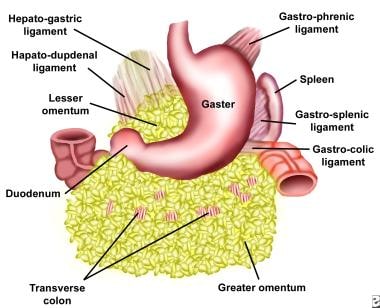 Diagram of subdivisions of the omentum. The greater omentum is attached to the caudal border of the greater curvature of the stomach and consists of the hepatoduodenal, gastrocolic, and gastrosplenic ligaments. The lesser omentum is divisible into 2 parts: the hepatogastric ligament and the hepatoduodenal ligament.
Diagram of subdivisions of the omentum. The greater omentum is attached to the caudal border of the greater curvature of the stomach and consists of the hepatoduodenal, gastrocolic, and gastrosplenic ligaments. The lesser omentum is divisible into 2 parts: the hepatogastric ligament and the hepatoduodenal ligament.
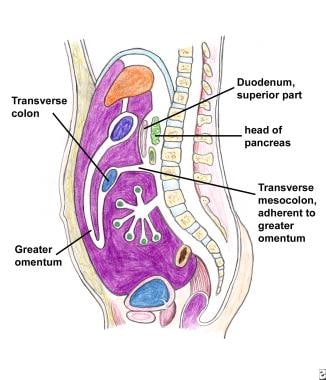 The anterior double-layered fold of the greater omentum descends from the stomach and the first part of the duodenum in front of the small intestine and ascends behind itself as far as the transverse colon.
The anterior double-layered fold of the greater omentum descends from the stomach and the first part of the duodenum in front of the small intestine and ascends behind itself as far as the transverse colon.
Pathophysiology
The omentum is composed of a trabecular connective-tissue structure carrying arteries, veins, lymphatics, and fat pads. The lining of the omentum is composed of two layers of mesothelial cells. The stroma of the omentum contains fibroblast, pericytes, lipocytes, and lymphoreticular bodies.
The pathologic spectrum of primary omental tumors is diverse. Although the greater omentum is mainly composed of adipose, vascular, and lymphatic tissue, omental tumors have predominantly consisted of smooth-muscle tissue tumors.
The most common malignant lesions are leiomyosarcomas, hemangiopericytomas, [2] and fibrosarcomas; liposarcomas [3, 4] have been reported as well. The most common benign tumors include gastrointestinal (GI) stromal tumors (GISTs; these have malignant potential dependent on tumor size, mitotic activity, cellularity, and invasive growth), leiomyomas, lipomas, [5] and fibromas. A few cases of perivascular epithelioid cell tumor (PEComa) of the greater omentum have been described. [6] A primary omental neuroendocrine tumor (NET) was described in a 2021 case report. [7]
A GIST is the most common mesenchymal tumor of the GI tract, with reports of GISTs originating in the omentum. [8, 9, 10, 11]
Leiomyosarcoma is the most common type of primary omental tumor that originates in smooth muscle, usually in the GI tract, retroperitoneum, and genitourinary tract. [12, 13, 14]
Hemangiopericytoma is a vascular tumor arising from the pericytes that surround capillaries. [15, 16] Typically, large staghorn vessels are seen within the tumor. Reticulin stain shows tumor cells external to the basement membrane of the vessels, distinguishing hemangiopericytoma from angiosarcoma. The tumor can be classified as benign or malignant. Although differentiating benign tumors from malignant tumors can be difficult, some authors have suggested that the degree of anaplasia and foci of necrosis are indicative of malignant potential.
Fibrosarcoma is a tumor that most commonly arises from the soft tissues of the extremities and trunk. Rare cases of intra-abdominal fibrosarcomas have been reported arising from the viscera, retroperitoneum, mesocolon, and greater omentum. [17] Fibrosarcomas exhibit varying degrees of differentiation, ranging from moderately differentiated regions comprised of fusiform cells arranged in a fasciculated pattern and associated with bands of collagen and reticulin to predominantly poorly differentiated areas comprised of solid areas devoid of reticulin. Histologic differentiation has been shown to be a useful prognostic indicator with soft-tissue fibrosarcomas.
Lipoblastoma is a benign soft-tissue solid tumor consisting of immature embryonal fat tissue. Only a few cases of omental lipoblastoma have been reported in the literature. [18] Differentiating lipoblastoma from liposarcoma may be difficult; however, several cytogenetic analysis and immunohistochemical markers have been reported as useful adjuncts in distinguishing between them. Reciprocal translocations involving band 8q11-8q13 and chromosome 2 have been reported as markers for use in deciphering lipoblastoma from myxoid liposarcoma.
Glomus tumors resemble the modified smooth-muscle cells of the glomus body, which consists of a specialized form of arteriovenous anastomosis whose function is thermal regulation. Only a few cases have been reported in the literature. Immunohistochemically, these tumors stain positive for alpha-smooth muscle actin, muscle-specific actin (HHF35), and vimentin. [19]
Teratomas are derived from all three germ layers: ectoderm, endoderm, and mesoderm. They range from benign, well-differentiated (mature) cystic lesions to those that are solid and malignant (immature). They are classified as either mature (well differentiated) or immature as a reflection of their benign or malignant nature, respectively. [20, 21, 22]
Epidemiology
United States and international statistics
Because of the rarity of omental tumors and the paucity of available information, the incidence of these tumors is unknown, both in the United States and worldwide. Most of the information in the medical literature has come from case reports. [23, 12, 24, 25, 20, 26, 27, 28, 19, 29, 30, 31, 10, 32, 33, 34, 35] From a group of 131 cases identified in the literature, the authors determined the distribution shown in Table 1 below.
Table 1. Distribution of Primary Omental Tumors (Open Table in a new window)
Tumor Histology |
Number of Cases |
% of Total |
Leiomyosarcoma |
22 |
17 |
Hemangiopericytoma |
8 |
6 |
Sarcoma |
3 |
2 |
Myosarcoma |
2 |
1.5 |
Fibrosarcoma |
3 |
2 |
Reticulosarcoma |
1 |
1 |
Spindle cell sarcoma |
1 |
1 |
Liposarcoma |
1 |
1 |
Rhabdomyosarcoma |
1 |
1 |
Leiomyoma/leiomyoblastoma |
14 |
11 |
Lipoma |
5 |
4 |
Fibroma |
3 |
2 |
Fibromatosis |
2 |
1.5 |
Mesothelioma |
2 |
1.5 |
Endothelioma |
1 |
1 |
Myxoma |
1 |
1 |
Neurofibroma |
1 |
1 |
Malignant fibrous histiocytoma |
1 |
1 |
Gastrointestinal stromal tumor (GIST) |
21 |
16 |
Glomus tumor |
2 |
1.5 |
Teratoma |
28 |
21 |
Lipoblastoma |
8 |
6 |
Total |
131 |
100 |
Age- and sex-related demographics
Collected studies indicate that these tumors are found in all ages but are diagnosed most frequently in the fifth to sixth decades of life. [13, 36, 37, 21]
Because of the limited number of reported cases in some pathologic categories, epidemiologic information is sparse. A slight male predominance has been suggested. In the authors' series, 35 of 66 patients (53%) with primary omental tumor were males. [13, 21]
Prognosis
Patients with primary malignant tumors of the omentum have a median survival time of only 6 months. Only 10-20% of patients are alive 2 years after surgical excision. The reason for this grave prognosis is not clear, given that only a minority of these patients have distant metastasis at initial diagnosis.
Benign omental tumors are associated with long-term survival after surgical resection. In one series, patients with benign tumors demonstrated a 5-year survival rate of 75%. Patients with liposarcomas showed a 5-year survival rate of 59-70%. Survival depends on histology types. Round cell liposarcomas are poorly differentiated tumors with frequent metastasis and are associated with shorter 5-year survival rates.
-
Diagram of subdivisions of the omentum. The greater omentum is attached to the caudal border of the greater curvature of the stomach and consists of the hepatoduodenal, gastrocolic, and gastrosplenic ligaments. The lesser omentum is divisible into 2 parts: the hepatogastric ligament and the hepatoduodenal ligament.
-
The anterior double-layered fold of the greater omentum descends from the stomach and the first part of the duodenum in front of the small intestine and ascends behind itself as far as the transverse colon.
Tables
Tumor Histology |
Number of Cases |
% of Total |
Leiomyosarcoma |
22 |
17 |
Hemangiopericytoma |
8 |
6 |
Sarcoma |
3 |
2 |
Myosarcoma |
2 |
1.5 |
Fibrosarcoma |
3 |
2 |
Reticulosarcoma |
1 |
1 |
Spindle cell sarcoma |
1 |
1 |
Liposarcoma |
1 |
1 |
Rhabdomyosarcoma |
1 |
1 |
Leiomyoma/leiomyoblastoma |
14 |
11 |
Lipoma |
5 |
4 |
Fibroma |
3 |
2 |
Fibromatosis |
2 |
1.5 |
Mesothelioma |
2 |
1.5 |
Endothelioma |
1 |
1 |
Myxoma |
1 |
1 |
Neurofibroma |
1 |
1 |
Malignant fibrous histiocytoma |
1 |
1 |
Gastrointestinal stromal tumor (GIST) |
21 |
16 |
Glomus tumor |
2 |
1.5 |
Teratoma |
28 |
21 |
Lipoblastoma |
8 |
6 |
Total |
131 |
100 |



