Practice Essentials
Acute mesenteric ischemia (AMI) is a syndrome caused by inadequate blood flow through the mesenteric vessels, resulting in ischemia and eventual gangrene of the bowel wall. Although relatively rare, it is a potentially life-threatening condition.
Broadly, AMI may be classified as either arterial or venous. AMI as arterial disease may be subdivided into nonocclusive mesenteric ischemia (NOMI) and occlusive mesenteric arterial ischemia (OMAI); OMAI may be further subdivided into acute mesenteric arterial embolism (AMAE) and acute mesenteric arterial thrombosis (AMAT). AMI as venous disease takes the form of mesenteric venous thrombosis (MVT). Thus, for practical purposes, AMI comprises four different primary clinical entities, as follows:
-
NOMI
-
AMAE
-
AMAT
-
MVT
The four types of AMI have somewhat different predisposing factors, clinical pictures, and prognoses. A secondary clinical entity of mesenteric ischemia occurs as a consequence of mechanical obstruction (eg, from internal hernia with strangulation, volvulus, or intussusception). Tumor compression, aortic dissection and postangiography thrombosis [1] are other reported causes. Occasionally, blunt trauma may cause isolated dissection of the superior mesenteric artery (SMA) and lead to intestinal infarction.
Because the four types of AMI share similarities and a final common pathway (ie, bowel infarction and death, if not properly treated), they may usefully be discussed together.
In 1930, Cokkinis remarked, “Occlusion of the mesenteric vessels is apt to be regarded as one of those conditions of which the diagnosis is impossible, the prognosis hopeless, and the treatment almost useless.” [2] This quote indicates some of the extreme difficulties faced by physicians treating AMI. Symptoms are nonspecific initially, before evidence of peritonitis presents. Thus, diagnosis and treatment are often delayed until the disease is advanced. [3, 4]
Fortunately, since 1930, many advances (eg, in magnetic resonance imaging [MRI] and Doppler flowmetry [5] ) have been made that allow earlier diagnosis and treatment. Whereas the prognosis remains grave for patients in whom the diagnosis is delayed until bowel infarction has already occurred, patients who receive the appropriate treatment in a timely manner are much more likely to recover. [6]
Treatment options for acute thrombosis focus on surgical methods, which have changed little since the late 20th century. Some patients may be good candidates for percutaneous transluminal angioplasty with stenting. [7, 8, 9, 10, 11, 12] Some authors recommend a trial of thrombolytic therapy if patients can be treated within 8 hours of presentation and do not have signs of bowel necrosis or peritonitis. [13] If no evidence of improvement is noted within 4 hours, patients should undergo exploration.
Because of the high mortality and the difficulty of diagnosis, mesenteric ischemia poses a substantial legal risk. This risk can be reduced by a high degree of clinical suspicion, early and aggressive diagnostic imaging, and early surgical consultation with clear documentation of timing. One review of 180 consecutive malpractice claims found seven cases involving AMI, with allegations of failure to make a timely diagnosis in five, failure to administer anticoagulation in one, and failure to prevent NOMI in one. [14]
Guidelines for the management of AMI have been published by the World Society of Emergency Surgery (WSES). [15] (See Guidelines.)
Anatomy
Mastery of the anatomy of the mesenteric vessels is the key to understanding and treating patients with mesenteric ischemia. However, the endless array of vascular variations can make this difficult.
The celiac axis, the SMA, and the inferior mesenteric artery (IMA) supply the foregut, midgut, and hindgut, respectively. [16] The celiac axis arises from the ventral surface of the aorta at the T12-L1 vertebral body. It courses anteroinferiorly before branching into the common hepatic, splenic, and left gastric arteries. The possible variations are too numerous to describe in this article.
The hepatic artery gives off the gastroduodenal artery, which branches further to the right gastroepiploic artery and the anterosuperior and posterosuperior pancreaticoduodenal arteries. The right gastroepiploic artery communicates with the left gastroepiploic artery, which is an immediate branch of the splenic artery. The anterosuperior and posterosuperior pancreaticoduodenal arteries communicate with the corresponding inferior branches from the SMA.
The splenic artery gives off the left gastroepiploic artery, as well as the dorsal pancreatic artery, which supplies the body and tail of the pancreas and communicates with the anterosuperior pancreaticoduodenal and gastroduodenal arteries and sometimes with the middle colic artery or SMA.
The left gastric artery, the third important branch of the celiac axis, communicates with the right gastric artery along the posterior aspect of the lesser curvature of the stomach. The celiac artery supplies most of the blood to the lower esophagus, stomach, duodenum, liver, pancreas, and spleen.
The SMA comes off the ventral aorta and supplies the midgut by giving off the inferior pancreaticoduodenal artery, middle colic, right colic, and jejunal and ileal branches.
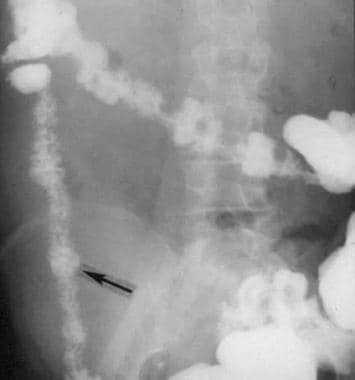
The inferior pancreaticoduodenal artery gives rise to the corresponding anteroinferior and posteroinferior branches, which anastomose with their superior counterparts. This communication is an important connection that helps to maintain bowel perfusion in times of atherosclerosis of the mesenteric vessels. (For an illustration of a meandering artery, see the image below.)
The ileocolic artery supplies the ileum, cecum, and ascending colon, whereas the middle colic supplies the transverse colon and communicates with the IMA. The right colic artery typically branches at the same level as the middle colic artery. The right and middle colic arteries provide an important supply of blood to the marginal artery of Drummond and give rise to the terminal vasa recta, which provide blood to the colon.
The IMA, the smallest mesenteric vessel, also comes off the anterior aorta. It supplies the distal transverse, descending, and sigmoid colon, as well as the rectum. Many communications to the SMA exist within the mesentery, and rectal branches offer communication between the visceral blood supply and the common supply. The “watershed area” near the splenic flexure was once believed more susceptible to ischemia secondary to poor arterial flow; however, it is now thought that the poor development of this area results in an increased propensity for ischemia.
The venous system, for the most part, parallels the arterial system. The superior mesenteric vein (SMV) is formed by the jejunal, ileal, ileocolic, right colic, and middle colic veins, which drain the small intestine, cecum, ascending colon, and transverse colon. The right gastroepiploic vein drains the stomach to the SMV, whereas the inferior pancreaticoduodenal vein drains the pancreas and duodenum.
The inferior mesenteric vein (IMV) drains the descending colon, the sigmoid colon, and the rectum through the left colic vein, the sigmoid branches, and the superior rectal vein, respectively. The IMV joins the splenic vein, which then joins the SMV to form the portal vein. The portal vein enters the liver.
Pathophysiology
Insufficient blood perfusion of the small bowel and colon may result from embolic or thrombotic arterial occlusion (AMAE or AMAT), thrombotic venous occlusion (ie, MVT), or nonocclusive processes such as vasospasm or low cardiac output (NOMI). [17, 18, 19] Embolic phenomena account for approximately 50% of all clinical cases, arterial thrombosis for about 25%, NOMI for roughly 20%, and MVT for fewer than 10%.
Rarely, isolated spontaneous dissections of the SMA have been reported. [20, 21, 22, 23] Whether the occlusion is arterial or venous, hemorrhagic infarction leading to perforation is the common pathologic pathway.
Injury severity is inversely proportional to the mesenteric blood flow and is influenced by the number of vessels involved, systemic mean blood pressure, duration of ischemia, and collateral circulation. The superior mesenteric vessels are involved more frequently than the inferior mesenteric vessels, with blockage of the latter often being silent because of better collateral circulation.
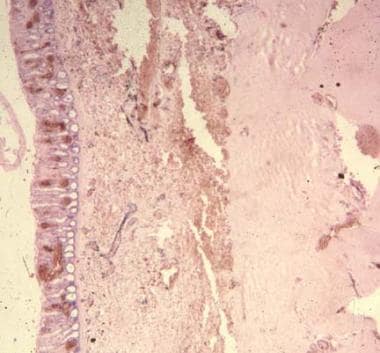
Damage to the affected bowel portion may range from reversible ischemia to transmural infarction with necrosis and perforation. The injury is complicated by reactive vasospasm in the SMA region after the initial occlusion. Arterial insufficiency causes tissue hypoxia, leading to initial bowel-wall spasm (see the image below). This leads to gut emptying by vomiting or diarrhea. Mucosal sloughing may cause bleeding into the gastrointestinal (GI) tract.
At this stage, little abdominal tenderness is present, producing the classic intense visceral pain that is disproportionate to physical examination findings.
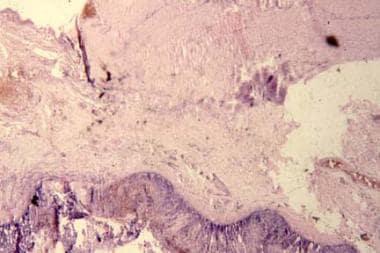
As the ischemia persists, the mucosal barrier becomes disrupted, and bacteria, toxins, and vasoactive substances are released into the systemic circulation (see the image below). This can cause death from septic shock, cardiac failure, or multisystem organ failure before bowel necrosis actually occurs.
As hypoxic damage worsens, the bowel wall becomes edematous and cyanotic. Fluid is released into the peritoneal cavity; this explains the serosanguineous fluid sometimes recovered by diagnostic peritoneal lavage. Bowel necrosis can occur in 8-12 hours from the onset of symptoms (see the image below). Transmural necrosis leads to peritoneal signs and heralds a much worse prognosis.
Acute mesenteric arterial embolism
AMAE (ie, embolic AMI) is usually caused by an embolus of cardiac origin. Typical causes include mural thrombi after myocardial infarction, atrial thrombi associated with mitral stenosis and atrial fibrillation, vegetative endocarditis, mycotic aneurysm, and thrombi formed at the site of atheromatous plaques within the aorta or at the sites of vascular aortic prosthetic grafts interposed anywhere between the heart and the origin of the SMA.
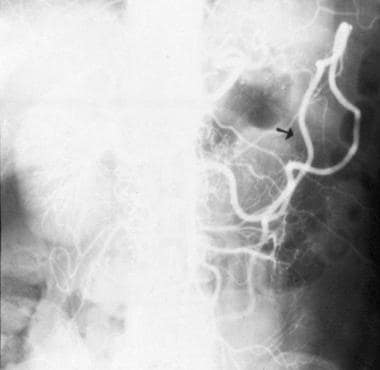
Because the vascular occlusion is sudden, patients have not been able to develop a compensatory increase in collateral flow. As a result, they experience worse ischemia than patients with AMAT. Because of its small takeoff angle from the aorta and higher flow, the SMA is the visceral vessel most susceptible to emboli (see the image below); the IMA is less commonly affected. [24] Most often, emboli lodge about 6-8 cm beyond the arterial origin, at a narrowing near the emergence of the middle colic artery.
 Complete aortic occlusion (Leriche syndrome) with acute embolism of superior mesenteric artery.
Complete aortic occlusion (Leriche syndrome) with acute embolism of superior mesenteric artery.
The US Centers for Disease Control and Prevention (CDC) Injury Center reports a special form of mesenteric ischemia due to systemic air embolism in victims of high-energy blast injuries. These patients sustain severe primary blast injury to the lung, a condition referred to as blast lung.
Acute mesenteric arterial thrombosis
AMAT (ie, thrombotic AMI) is a late complication of preexisting visceral atherosclerosis. Symptoms typically do not develop until two of the three arteries (usually the celiac artery and the SMA) are stenosed or completely blocked. [25] Progressive worsening of the atherosclerotic stenosis before the acute occlusion allows time for development of additional collateral circulation.
A thrombus forms during a state of low flow, resulting in acute cessation of flow to the gut. Bloody stools develop as the more sensitive mucosa dies first. The bowel gradually becomes necrotic (see the image below); subsequently, bacterial overgrowth develops, and the resulting bowel perforation causes sepsis and finally death.

Most patients with AMAT have atherosclerotic disease at other sites (eg, coronary artery disease [CAD], cerebrovascular accident or stroke, or peripheral arterial disease [PAD]). A drop in cardiac output resulting from myocardial infarction (MI) or congestive heart failure (CHF) may cause AMI in a patient with visceral atherosclerosis.
AMAT may also be a complication of arterial aneurysm or other vascular pathologies, such as dissection, trauma, and thromboangiitis obliterans. In inflammatory vascular disease, smaller vessels are affected. Thrombosis tends to occur at the origin of the SMA, causing widespread infarction. These patients frequently present with a history of chronic mesenteric ischemia in the form of intestinal angina before the emergency event.
Nonocclusive mesenteric ischemia
NOMI is precipitated by a severe reduction in mesenteric perfusion, with secondary arterial spasm from such causes as cardiac failure, septic shock, hypovolemia, or the use of potent vasopressors in critically ill patients. [18] Because bowel perfusion, like cerebral perfusion, is preserved in the setting of hypotension, NOMI represents a failure of autoregulation. Many vasoactive drugs (eg, digitalis, cocaine, diuretics, and vasopressin) may also cause regional vasoconstriction. [26] Gross pathologic arterial or venous occlusions are not observed.
Mesenteric venous thrombosis
MVT often (ie, >80% of the time) is the result of some processes that make the patient more likely to form a clot in the mesenteric circulation (ie, secondary MVT). Primary MVT occurs in the absence of any identifiable predisposing factor. MVT may also occur after ligation of the splenic vein for a splenectomy or ligation of the portal vein or the SMV as part of damage control surgery for severe penetrating abdominal injuries. Other associated causes include pancreatitis, sickle cell disease, and hypercoagulability caused by malignancy.
The mechanism responsible for ischemia in this setting is a massive influx of fluid into the bowel wall and lumen, which results in systemic hypovolemia and hemoconcentration. The consequent bowel edema and decreased outflow of blood secondary to venous thrombosis impede the inflow of arterial blood, and this leads to bowel ischemia. Although bowel ischemia is itself detrimental to the patient, it is the resulting multiple organ system failure that actually accounts for the high mortality.
MVT often affects a much younger population. Symptoms may be present longer than in more typical cases of AMI, sometimes for more than 30 days. Infarction from MVT is rarely observed with isolated SMV thrombosis, unless collateral flow in the peripheral arcades or vasa recta is compromised as well. Fluid sequestration and bowel wall edema are more pronounced than in arterial occlusion. The colon is usually spared because of better collateral circulation.
In a study of mortality factors in 31 patients with MVT, Abu-Daff et al determined that 30-day mortality in these patients was strongly linked to colonic involvement in ischemia and to short-bowel syndrome. [27] Lack of anticoagulation also may have been a factor. The 5-year mortality, according to the investigators, was primarily related to short-bowel syndrome.
Etiology
Acute mesenteric arterial embolism
Causes of AMAE (embolic AMI) include the following [19] :
-
Cardiac emboli - Mural thrombus after MI, auricular thrombus associated with mitral stenosis and atrial fibrillation, or septic emboli from valvular endocarditis (less frequent)
-
Emboli from fragments of proximal aortic thrombus due to a ruptured atheromatous plaque
-
Atheromatous plaque dislodged by arterial catheterization or surgery (eg, aortic aneurysm resection)
Most emboli lodge in the SMA, just distal to the origin of the middle colic artery. Embolization is less often associated with ischemic disease than thrombosis and has a better survival rate when optimally treated.
Acute mesenteric arterial thrombosis
Causes of AMAT (thrombotic AMI) include the following:
-
Atherosclerotic vascular disease (most common)
-
Aortic aneurysm
-
Aortic dissection
-
Arteritis
-
Decreased cardiac output from MI or CHF (thrombotic AMI may cause acute decompensation)
-
Dehydration from any cause
Unlike embolic events, which generally occur in arterial branches and result in limited bowel ischemia, thrombosis typically occurs at the vessel’s origin, resulting in extensive bowel involvement.
Nonocclusive mesenteric ischemia
Causes of NOMI include the following:
-
Hypotension from CHF, MI, sepsis, aortic insufficiency, severe liver or renal disease, or recent major cardiac or abdominal surgery
-
Vasopressors
-
Ergotamines
-
Digitalis (it is unclear whether digitalis use causes NOMI or whether patients who develop NOMI are older and thus more likely to have been prescribed digitalis)
Case reports have documented celiac artery compression syndrome (CACS) as a cause of mesenteric ischemia through external compression of the celiac artery, usually by the median arcuate ligament or the celiac ganglion. [30, 31] Case reports have also described marathon runners who develop ischemic colitis after a marathon; in most instances, this resolves with supportive treatment. [32]
Mesenteric venous thrombosis
Causes of MVT include the following (>80% of patients with MVT are found to have predisposing conditions):
-
Tumor causing venous compression or hypercoagulability (paraneoplastic syndrome)
-
Infection, usually intra-abdominal (eg, appendicitis, diverticulitis, or abscess)
-
Venous congestion from cirrhosis (portal hypertension)
-
Increased intra-abdominal pressure from pneumoperitoneum during laparoscopic surgery [39]
-
Pancreatitis
-
Decompression sickness
Epidemiology
United States and international statistics
AMI is believed to account for 0.1% of all hospital admissions; this figure may be expected to rise as the population ages. Annual incidence in the general population has been reported to be in the range of 0.63-12.9 per 100,000. [44] The exact prevalence of MVT is not known, because many cases are presumed to be limited in symptomatology and to resolve spontaneously. It is believed to account for approximately 10-15% of all cases of mesenteric ischemia and for 0.006% of hospital admissions. Venous thrombosis is found in approximately 0.001% of patients who undergo exploratory laparotomy.
Risk factors for AMI include atherosclerosis, arrhythmias, hypovolemia, CHF, recent MI, valvular disease, advanced age, and intra-abdominal malignancy. [45, 46, 47, 48] Mesenteric artery stenosis is found in 17.5% of independent elderly adults. [49] Approximately two thirds of patients are women.
Research indicates that inflammatory bowel disease (IBD) is another risk factor for mesenteric artery thrombosis. [50] In a review comparing 17,487 patients who had either Crohn disease or ulcerative colitis with 69,948 control subjects, the investigators detected a significantly higher risk of AMI in the patients with IBD. [46]
Outside the United States, reported rates of AMI are probably lower in countries with limited diagnostic capability or whose populations have a shorter life expectancy because AMI is primarily a disease of older individuals.
Age-, sex-, and race-related demographics
In large part because of the association with atherosclerosis, [51] AMI is commonly considered a disease of the older population, with the typical age of onset being older than 60 years. Nevertheless, younger people who have atrial fibrillation or risk factors for MVT, such as oral contraceptive use or hypercoagulable states (eg, those caused by protein C or S deficiency), may present with AMI.
No overall sex preference exists for AMI. Men might be at higher risk for occlusive arterial disease because they have a higher incidence of atherosclerosis. Conversely, women who are taking oral contraceptives or are pregnant are at higher risk for MVT.
No racial predilections are known for AMI. However, people of races with a higher rate of conditions leading to atherosclerosis, such as African American people, might be at higher risk.
Prognosis
Although survival rates for AMI have improved over the past four decades, the prognosis for patients with AMI of any type remains grave. [19] Over the past 15 years, the all-cause mortality from AMI has averaged 71% (range, 59-93%). Once bowel-wall infarction has occurred, mortality may be as high as 90%. Even with good treatment, as many as 50-80% of patients die. For those patients who do survive, the risk of rethrombosis is high, and lifestyle may be hindered by a lifetime of total parenteral nutrition as a remedy for short-gut syndrome.
Predictors of mortality have included older age, bandemia, hepatic and renal impairment, hyperamylasemia, metabolic acidosis, hypoxia, intramural pneumatosis, and sepsis. [52] Mortality is highest for AMAT, [53] followed by NOMI, AMAE, and MVT. [54]
Early and aggressive diagnosis and treatment have been shown to reduce mortality substantially if the diagnosis is made before the development of peritonitis. [55] It is essential to act early on clinical suspicion, rather than wait for the arrival of hard evidence. Survivors of extensive bowel resection face significant long-term morbidity because of the reduced intestinal mucosal surface available for absorption. However, with rapid treatment, mortality can be reduced considerably, and patients may be spared bowel resection.
A long-term follow-up study of 31 AMI patients who had surgery and survived the acute episode revealed 2- and 5-year survival rates of 70% and 50%. [56] Deaths were mainly related to cardiovascular comorbidity and malignant disease. With appropriate anticoagulation, only one patient died after a recurrent attack of AMAT.
Early recognition and treatment of NOMI has been shown to reduce mortality to 50-55%.
In a report from Madrid describing 21 patients with SMA embolus, intestinal viability was achieved in 100% of patients if the duration of symptoms was shorter than 12 hours, 56% if the duration was 12-24 hours, and only 18% if the duration was longer than 24 hours. [57] Another study found that even at hospital centers with angiography available 24 hours a day, mortality still was approximately 70%. [58]
MVT is associated with a 30-day mortality of 13-15%. Without anticoagulant therapy, mortality approaches 30%, with a 25% recurrence rate. The combination of anticoagulant therapy with surgery is associated with the lowest recurrence rate (~3-5%). Patients presenting with peritonitis and infarcted bowel have a prolonged and complicated course.
Patient Education
Patients who survive to discharge should be educated regarding short-bowel syndrome. They should also be instructed about the importance of taking warfarin or other discharge medications to prevent recurrence.
-
Pneumatosis intestinalis (black stripes of air) in advanced acute mesenteric ischemia (AMI) with gangrenous bowel.
-
CT scan (with contrast) of nonocclusive mesenteric ischemia with resulting bowel wall edema (arrows).
-
Aortogram showing narrowing of superior mesenteric artery.
-
Radiograph showing bowel spasm (early sign of ischemia).
-
Gas in colon wall (typical of advanced ischemia).
-
Ischemia stricture.
-
Thumbprinting of bowel, characteristic of mesenteric artery ischemia.
-
Pathologic findings 2 hours after bowel ischemia starts.
-
Microscopic findings 24 hours after ischemia starts.
-
Gross specimen showing hemorrhagic dead bowel after resection from patient with acute mesenteric ischemia.
-
Pneumatosis intestinalis, one of few radiographic findings in patients with mesenteric ischemia.
-
Diagnosis and treatment of intestinal ischemia (mesenteric venous thrombosis and major nonembolic arterial occlusion). Solid lines indicate accepted management plan; dashed lines indicate alternate management plan. DVT=deep vein thrombosis; SMA=superior mesenteric artery. Adapted from Gastroenterology. 2000 May;118(5):954-68.
-
Diagnosis and treatment of intestinal ischemia (minor arterial occlusion or embolus, major embolus, and splanchnic vasoconstriction without occlusion). Solid lines indicate accepted management plan; dashed lines indicate alternate management plan. DVT=deep vein thrombosis; SMA=superior mesenteric artery. Adapted from Gastroenterology. 2000 May;118(5):954-68.
-
Management of colon ischemia. Solid lines indicate accepted management plan; dashed lines indicate alternative management plan. BE=barium enema; NPO—nil per os (nothing by mouth); PLC=protein-losing colopathy; IBD=inflammatory bowel disease. Adapted from Gastroenterology. 2000 May;118(5):954-68.
-
Complete aortic occlusion (Leriche syndrome) with acute embolism of superior mesenteric artery.
-
Gross specimen of dead bowel.
-
Meandering artery (radiographic sign of preexisting bowel ischemia).
-
CT scan demonstrating thrombosis of superior mesenteric vein.
-
CT scan demonstrating thrombosis of portal vein.
-
CT scan demonstrating cavernous change of superior mesenteric vein as consequence of venous thrombosis.
-
Mesenteric venous air (red arrows) and free intraperitoneal air (white arrow.) Mesenteric venous air is common finding in advanced acute mesenteric ischemia. Courtesy of Brandon Dessecker, MD, Melanie Nukula, MD, and Robert Marx, DO.
-
Pronounced portal venous air seen within liver (red arrow), as well as free intraperitoneal air (white arrow) and pneumatosis intestinalis throughout bowel wall, which are classic findings for advanced acute mesenteric ischemia. Courtesy of Brandon Dessecker, MD, Melanie Nukula, MD, and Robert Marx, DO.







