Practice Essentials
Thrombosis of the inferior vena cava (IVC) is an underrecognized entity with a variety of clinical presentations. The general concepts of deep venous thrombosis (DVT) and thrombophlebitis are discussed in detail in Deep Venous Thrombosis. However, the implications and complexity of IVC thrombosis (IVCT) merit specific attention. [1, 2]
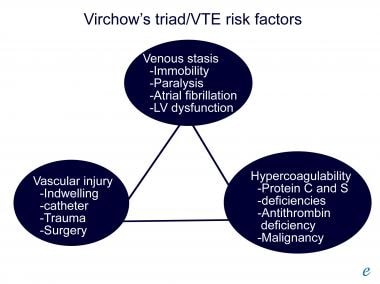
From a global standpoint, IVCT represents a subset of DVT. Virchow recognized and described the factors predisposing a patient to venous thrombosis. The triad of stasis, vessel injury, and hypercoagulability formulated by Virchow remain the foundation for our understanding of the pathophysiology of DVT in general and for IVCT in particular (see the image below).
As appreciation of the impact of these factors on the patient has improved, therapy has become more directed.
The clinical presentation of IVCT varies, depending on extent and location of the thrombus. Because of the variability in signs and symptoms, using a classification system to describe the clinical features may aid in the diagnosis of this condition.
Thrombophilic screening and evaluation of the clotting and fibrinolytic systems may aid in the diagnosis of IVCT. Contrast venography remains the criterion standard as the optimal diagnostic study for this condition.
Medical management of vena caval thrombosis focuses on anticoagulation and thrombolytic therapy. Surgical management of this condition consists of caval interruption, thrombectomy, or endovascular interventions.
Patient education
For patient education information, see the Circulatory Problems Center, as well as Deep Vein Thrombosis (Blood Clot in the Leg, DVT).
Anatomy
Understanding the anatomy of the IVC and its tributaries is essential to understanding the variability in the clinical presentations of patients with IVCT (see the image below).
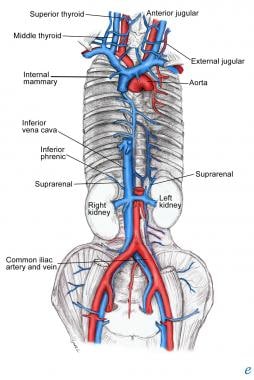 Veins of abdomen and thorax. Unless stated otherwise, lithograph plate is from Gray's Anatomy (online edition of the 20th US edition of Gray's Anatomy of the Human Body, originally published in 1918).
Veins of abdomen and thorax. Unless stated otherwise, lithograph plate is from Gray's Anatomy (online edition of the 20th US edition of Gray's Anatomy of the Human Body, originally published in 1918).
The IVC is formed by the confluence of the left and right common iliac veins. Numerous paired segmental lumbar veins drain into the IVC throughout its length. The right gonadal vein empties directly into the cava, whereas the left gonadal vein generally empties into the left renal vein. The azygous system has connections with the IVC or the renal veins at the level of the renal veins.
The next major veins encountered are the renal veins, followed by the hepatic veins. No valves are within the IVC. The cava enters the thoracic cavity through the tendinous portion of the diaphragm and terminates at its junction with the right atrium.
Several congenital anomalies of venous anatomy can involve the IVC, and their presence can increase the likelihood of IVCT. The symptomatology related to IVCT follows directly from the anatomic location of the thrombus and the degree of the lumen occupied by the thrombus.
Pathophysiology
Congenitally normal inferior vena cava
Thrombosis of the IVC in the absence of congenital abnormalities is rare; when it does occur, it is usually the result of a predisposing hypercoagulable state along with an acquired pathology in the IVC or one of its adjacent structures. [3, 4, 5, 6, 7] Iatrogenic thrombotic occlusion of IVC filters is increasing, particularly in the United States. As a consequence of the high number of IVC filter placements and the low retrieval rates (10-34%), [8, 9, 10] late filter thrombosis has been reported in as many as 33% of patients. [4, 5, 11, 12]
Congenital abnormalities of inferior vena cava
Congenital abnormalities of the IVC are rare (incidence, ~1%); however, IVCT thrombosis is more common among patients with such anomalies (range, 60-80%). [13, 14, 15] In patients with congenital cardiac defects, the incidence ranges from 2% to 3%. [16] Congenital IVC anomalies have three main anatomic configurations, as follows. [17, 6, 18] :
-
Infrarenal - Duplicate IVC, persistent left-side IVC, preaortic IVC, absence of the infrarenal IVC
-
Renal - Accessory left renal vein, retroaortic and circumaortic left renal vein
-
Suprarenal - Absence of the hepatic IVC with azygos continuation, congenital caval stenosis or atresia, IVC membranes
Because of well-developed collaterals, patients with congenital IVC anomalies rarely experience symptoms. The anatomic variants listed above are often noted as incidental findings on abdominal imaging. [14] Symptoms (eg, acute or chronic proximal DVT or evidence of chronic venous insufficiency) observed in patients are usually attributable to the involvement of the venous collaterals (frequently the deep pelvic veins or common iliac veins).
Etiology
To a large degree, the etiology of IVCT mirrors that of DVT in general. However, specific situations relate to the IVC only, but the wide variety of these situations all relate in one or more ways to Virchow's classic description.
Tumors
Numerous malignancies have been associated with IVCT. [19] Perhaps the most familiar is renal cell carcinoma (RCC). The intravascular tumor extends from the renal vein and can propagate as far as the heart. It can partially or completely occlude the IVC. Not all intravascular irregularities of the kidney represent tumor thrombus. In one case report, a patient who underwent radical nephrectomy for presumed RCC was subsequently found to have only renal vein thrombosis. [20] Other genitourinary tumors that reportedly cause IVCT are seminomas and teratomas.
Numerous other less common tumors reportedly involve the IVC. Intuitively, it is reasonable that any structure anatomically related to the IVC can generate either direct compression or vascular invasion. Retroperitoneal leiomyosarcoma, [21] adrenal cortical carcinoma, [22] and renal angiomyolipoma [23] have all presented in association with IVCT. Even hepatic hemangioma has caused IVCT from extrinsic compression. [24] Additionally, malignancy itself is a risk factor for DVT and thus represents a risk factor for the extension of DVT into the IVC.
Compression
Extrinsic compression may also result from nontumoral sources and increase the likelihood of IVCT. The distortion of the normal caval anatomy generates both venous stasis and turbulent flow. This situation facilitates the formation of a thrombus. An activity as innocuous as bicycle riding has reportedly caused IVCT. [25] The spectrum of medical diagnoses that can cause compression of the IVC is determined by those structures anatomically adjacent to the IVC.
Abdominal aortic aneurysms (AAAs) can compress the IVC and cause thrombosis. Although this clinical situation is uncommon, the implications for surgical repair of the aneurysm are significant. The surgeon must be prepared for enlarged venous collaterals and the possibility of unusual tissue-plane configurations. One reported case described incorporation of the IVC into the aneurysm [26] ; the wall of the IVC was actually part of the wall of the aneurysm. Knowing that AAA is a risk factor for IVCT should heighten clinical suspicion in appropriate cases.
Hepatic abscesses, either from amebae or echinococci, can also generate thrombosis of the IVC from compression. Because of the propensity of these processes to evolve over time, patients may present without symptoms suggestive of IVC occlusion. They may only demonstrate evidence of the primary process or of collateral venous hypertrophy. The initial presenting symptom may even be pulmonary embolization.
Other retroperitoneal organ systems that have been shown to cause IVCT include the pancreas and the kidneys. Polycystic disease of the right kidney has reportedly been clinically associated with thrombosis of the IVC. [27] Pancreatic pseudocysts have been observed to cause thrombosis of the IVC. [28] Acute pancreatitis has also been found to generate thrombosis of the IVC. [29, 30]
The pathophysiology of the evolution of the thrombosis may reflect either the local impact of inflammation of the pancreatic head or the impact of a hypercoagulable state on the IVC. Although IVCT in the setting of pancreatitis is uncommon, this clinical entity may account for an unexplained deterioration in the status of a patient with acute pancreatitis.
Hematoma/trauma
Other aspects of compression can be attributed to the presence of a hematoma adjacent to the cava or the iliac systems. Psoas hematomas and other hematomas of the retroperitoneum have been identified as causing IVCT. In one case, the hematoma was the result of a common iliac artery injury. Because the venous system was not involved, the presumed mechanism of compression of the cava by clot seems credible.
Unique among causes, trauma combines the limbs of the Virchow triad. Stasis, vessel injury, and hypercoagulability may all exist in the same clinical situation. Direct trauma to the IVC may be the result of either penetrating or blunt trauma. [31, 32, 33] In the absence of venous laceration, blunt endothelial damage has been postulated to cause IVCT. Other mechanisms observed secondary to trauma include extension of hepatic venous thrombosis and thrombus formation after perihepatic packing.
Dysfunctional coagulation system
By necessity and function, the balance between the coagulation system and the fibrinolytic system is delicate and dynamic. Disorders that disrupt this balance can cause a situation in which IVC thrombus formation may occur.
The nephrotic syndrome is a classic example. Patients with this syndrome have urinary protein losses. Both renal vein thrombosis and IVCT have been described. The exact mechanism of the hypercoagulability of patients with the nephrotic syndrome has not been fully delineated. However, these patients have massive urinary protein loss, and diminished levels of antithrombin III have been observed.
Iatrogenic
Patients with a recent history of medical care may present with iatrogenic IVCT. The expansion of endovascular technology has led to increased recognition of iatrogenic IVCT. [34] Interventions that reportedly have identifiable rates of IVCT include the following:
-
Hepatic transplant
-
Dialysis access
-
Femoral venous catheters
-
Pacemaker wires
-
Vena caval filters
Awareness of the association of these procedures with IVCT allows clinicians to make educated decisions. Recognizing the association allows an accurate risk-benefit assessment for a given procedure. Additionally, recognizing these factors may aid in determining a prompt diagnosis in patients who have postprocedural clinical changes.
Congenital absence of inferior vena cava
Anomalies of the IVC have been described more frequently (0.6-2%) in those with other cardiovascular defects [35] and less so in otherwise healthy individuals. Various abnormalities of the IVC have been described, including complete absence, partial absence, or presence of bilateral IVC. [36]
Absent IVC is an extremely rare anomaly that is associated with idiopathic DVT, particularly in the young. Controversy exists as to whether an absent IVC has a true embryonic etiology or whether it is the result of perinatal IVC thrombosis causing regression and disappearance of the once present IVC. [37]
A case report has described an absent IVC and left renal hypoplasia and a right hypertrophic kidney. [38] A more commonly recognized association is right renal aplasia, as suggested in a review by Gayer et al, in which all nine patients with complete absence of the IVC had an absent or very small right kidney. [39]
The association of an absent or hypoplastic kidney is related (or may contribute to an absent IVC) to perinatal renal vein thrombosis. [40] Veen et al proposed naming this condition KILT (kidney and IVC abnormalities with leg thromboses) syndrome (when associated with DVT). [38]
It is estimated that DVT occurs at a rate of 1 case per 1000 patient-years [41] ; in as many as 80% of patients who are affected, a risk factor can be identified. Ruggeri et al presented four cases of absent IVC over a 5-year period that presented with idiopathic DVT in patients younger than 30 years, [42] representing an estimated 5% of cases of idiopathic DVT in young people.
Chee et al similarly noted that as many as 5% of 20- to 40-year-old patients presenting with DVT had an IVC anomaly (four in total, of which three had a complete absence of IVC). [13] This was much higher than the expected 0.5%.
Other associated conditions
Numerous other clinical situations have been associated with IVCT. They may meet some classification criteria to be listed in one or more of the categories mentioned above; however, they are noted here for clarity and can include (1) developmental anomalies of the IVC, (2) retroperitoneal fibrosis, (3) pregnancy, and (4) oral contraceptives.
Although not all-inclusive, the foregoing information provides a review of many of the known clinical situations in which IVCT may be evident. Knowledge of the potential for thrombosis of the IVC increases physicians' level of clinical awareness in patients who present with the identified primary processes.
Epidemiology
The exact number of patients who have IVCT remains elusive because of the clinical variability in presentation. By compiling information from several epidemiologic studies that investigated DVT prevalence, the following US estimates can be generated:
-
The DVT rate in the United States is 60-180 cases per 100,000 population per year
-
The frequency of IVCT in patients with DVT is 4-15%
-
Annually, 165,000-493,000 cases of DVT occur
-
Between 6600 and 74,000 cases of IVCT occur each year
These numbers are estimates generated from various population-based studies. Various groups within the general population have a greater propensity for IVCT (see Etiology).
Prognosis
The outcome of patients with IVCT is often determined by the underlying condition that initially caused the thrombosis. However, some general statements can be made. The impact and outcome of IVCT are as variable as the clinical presentation. In one study, only one third of patients had a correct diagnosis before venography. Adult patients with ligation of their vena cava reportedly have either no symptoms or mild edema after ligation. [43]
A report on children who had IVCT unrelated to catheterization revealed that 50% had persistent IVCT. Symptoms of chronic limb pain and chronic abdominal pain were observed. Another series of pediatric patients with IVCT secondary to central venous access identified no sequelae unless concurrent superior vena cava thrombosis was present.
Finally, the outcome of patients who have IVCT relates to the embolic risk associated with DVT overall. If the cava is occluded, pulmonary embolization does not present a significant risk. However, if a caval lumen remains, embolization may occur.
-
Virchow triad/venous thromboembolism (VTE) risk factors.
-
Photo showing dilated superficial abdominal veins (upper quadrant), with bruising and thrombosed large abdominal veins (lower quadrant).
-
Abdominal CT scan shows absent inferior vena cava with thrombosis of very prominent collateral veins in the abdominal wall, corresponding to right side of abdomen as seen in earlier photo.
-
Veins of abdomen and thorax. Unless stated otherwise, lithograph plate is from Gray's Anatomy (online edition of the 20th US edition of Gray's Anatomy of the Human Body, originally published in 1918).