Practice Essentials
Chyle fistula is defined as a leakage of lymphatic fluid from the lymphatic vessels, typically accumulating in the thoracic or abdominal cavities but occasionally manifesting as an external fistula. It is a rare but potentially devastating and morbid condition.
First described in the 17th century as complications of trauma, chyle fistulas most commonly occur secondary to lymphatic disease or malignancy or following abdominal, neck, or thoracic operations. [1, 2] Chyle fistulas also can form as a result of venous hypertension, and they have been described in patients with superior vena cava syndrome or thrombosis of the vena cava.
Patients with chyle fistulas usually give histories of some comorbid conditions such as malignancy or prior operations of the chest, neck, or abdomen. In postoperative patients, symptoms become evident after the start of oral feeding and depend on the site of obstruction.
Chyle fistulas can cause extreme morbidity because of loss of fluids, electrolytes, and other nutrients. In addition, chyle fistulas can result in loss of lymphocytes and immune dysfunction. Finally, chyle fistulas are space-filling and exert pressure on surrounding tissues, creating symptoms that can range from minimal discomfort to life-threatening situations.
Treatment of chyle fistulas is determined by the following (see Treatment):
-
Etiology of the fistula
-
Amount of output
-
Site of the fistula
Anatomy
The cisterna chyli and the thoracic duct drain lymph from the entire body except the head, neck, arms, and right thorax (which instead use the right bronchomediastinal, jugular, and subclavian lymph trunks to form the right lymph duct). The anatomy is highly variable; 50% of people do not have an identifiable cisterna chyli. In addition, half of the 4 L of lymph draining through the cisterna chyli and thoracic duct originates from the intestinal and hepatic lymphatics.
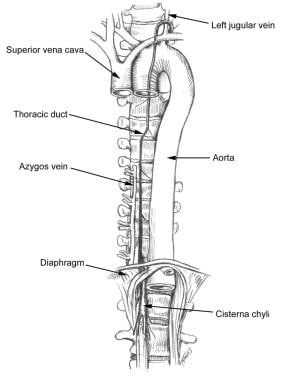
The cisterna chyli is found on the posterolateral edge to the right of the aorta at the level of vertebral bodies T12, L1, L2, and L3 as lymphatics from the mesentery, intercostal, and lumbar regions coalesce in the retroperitoneal space.
At approximately L1, the cisterna chyli ascends, becoming the thoracic duct (see the image below). The duct then enters the posterior mediastinum, crosses at T4 into the left retropleural space, and continues in a cephalad direction. The thoracic duct then enters the venous system at the junction of the left subclavian and internal jugular veins).
Pathophysiology
Leakage of lymph from damaged lymph vessels is common after surgery or trauma. [1] However, damaged lymphatics most often heal spontaneously or direct lymph centrally via rich interconnected lymphatic collaterals, without any significant morbidity. For chyle fistulas to form, either a scarcity of lymphatic collaterals must be present or the injury to the lymphatic channels must overwhelm the remaining lymphatic vessels. In addition, abnormal lymphatic vessels may be incapable of adequate lymph flow, leading to the accumulation of chyle.
Chyle flow varies dramatically depending on the quantity and quality of oral intake. During times of starvation, chyle flow is minimal. After meals, especially those with high contents of long-chain fatty acids, chyle flow increases dramatically. This basic knowledge provides the rationale for controlling dietary intake as part of the treatment of this disease.
Etiology
Chyle fistulas are rare events. Typical causes include the following [1] :
-
Lymphatic disease
-
Malignant invasion of the lymphatics
-
Trauma
-
Inflammatory reactions (eg, tuberculosis, pancreatitis, cirrhosis, adhesions, pulmonary fibrosis)
-
Postoperative trauma following abdominal, [3] neck, [4] or thoracic [5] operations - Approximately 75% of postoperative chyloperitoneum cases occur after abdominal aortic aneurysm repair, 19% after aortofemoral bypass, and 7% after resection of infected aortic grafts [1] ; chylous fistula after spinal surgery, though quite rare, has been reported [6] ; the extent of surgery is the main predictor of chylous ascites after major abdominal procedures [7]
-
Chyle fistula. Anatomy of the thoracic duct in relation to the aorta.
-
Chyle fistula. Management of chyloperitoneum.
-
Chyle fistula. Management of chylothorax.



