Practice Essentials
Hepatocellular carcinoma (HCC) is a primary malignancy of the liver (see the image below) that occurs predominantly in patients with underlying chronic liver disease and cirrhosis. However, up to 25% of patients have no history of cirrhosis or risk factors for it.
 Large hepatocellular carcinoma. Image courtesy of Arief Suriawinata, MD, Department of Pathology, Dartmouth Medical School.
Large hepatocellular carcinoma. Image courtesy of Arief Suriawinata, MD, Department of Pathology, Dartmouth Medical School.
The incidence of HCC has been rising worldwide over the last 20 years and is expected to increase until 2030 in some countries, including the United States. [1] The incidence of HCC is highest in Asia and Africa, where the endemic high prevalence of hepatitis B and hepatitis C strongly predisposes to the development of chronic liver disease and subsequent development of HCC.
Current international vaccination strategies for hepatitis B virus (HBV), and advances in the management of hepatitis C virus (HCV) infections, promise to have a major impact on the incidence of HCC, but their benefit will be realized slowly because of the very long latency period—20-30 years—from hepatic damage to HCC development.
Meanwhile, however, there is a growing problem with cirrhosis due to nonalcoholic fatty liver disease (NAFLD), specifically nonalcoholic steatohepatitis (NASH). NASH, which typically develops in the setting of obesity, type 2 diabetes, dyslipidemia, and hypertension, appears to lead the list of risk factors for HCC in the United States. [2, 3]
The presentation of HCC has evolved significantly over the past few decades. Whereas in the past, patients with HCC generally presented at an advanced stage, with right-upper-quadrant pain, weight loss, and signs of decompensated liver disease, HCC is now increasingly recognized at a much earlier stage as a consequence of the routine screening of patients with known cirrhosis, using ultrasonography with or without serum alpha-fetoprotein (AFP) measurements.
The diagnosis of HCC can often be established on the basis of noninvasive imaging, without biopsy confirmation. Even when biopsy is needed, imaging is usually required for guidance. [4] Laboratory evaluation of patients with newly diagnosed HCC should include testing to determine the severity of the underlying liver disease and to elucidate the etiology of the underlying disease, such as the following:
-
CBC
-
Electrolytes
-
Liver function tests
-
Coagulation studies
-
AFP determination
See Workup for more information.
Liver transplantation remains the best option for patients with HCC. Unfortunately, the supply of good-quality deceased-donor organs is limited. Thus, other treatments, including resection; radiofrequency ablation (RFA); and, potentially, systemic therapy should be used to bridge patients to transplant or to delay recurrence if possible. The following agents are approved for first-line treatment of unresectable HCC:
-
Sorafenib
-
Lenvatinib
-
Atezolizumab plus bevacizumab
-
Tremelimumab plus durvalumab
Agents approved for treatment of HCC unresponsive to sorafenib and other therapies are as follows:
-
Regorafenib
-
Pembrolizumab
-
Cabozantinib
-
Ramucirumab
-
Nivolumab plus ipilimumab
-
Dostarlimab
-
Selpercatinib
See Treatment and Medication.
For patient education resources, see Hepatitis, the Cirrhosis of the Liver Directory, and the Liver Cancer Directory.
Anatomy
A complete understanding of the surgical and interventional approach to the liver requires a comprehensive understanding of its anatomy and vascular supply. [5, 6] The liver is the largest internal organ, representing 2-3% of the total body weight in an adult. It occupies the right upper quadrant of the abdomen, surrounding the inferior vena cava, and attaches to the diaphragm and parietal peritoneum by various attachments that are commonly referred to as ligaments.
The vascular supply of the liver includes two sources of inflow that travel in the hepatoduodenal ligament, as follows:
-
Hepatic artery
-
Portal vein
The hepatic artery is generally derived from the celiac axis, which originates on the ventral aorta at the level of the diaphragm. Common variations include a replaced right hepatic artery, which originates from the superior mesenteric artery, a replaced left hepatic artery, which is derived from the left gastric artery, or a completely replaced common hepatic artery, which can originate from the superior mesenteric artery or the aorta. The hepatic artery supplies 30% of the blood flow to the normal liver parenchyma but greater than 90% to hepatic tumors, including both HCC and metastatic lesions.
The other major inflow vessel is the portal vein which carries 70-85% of the blood into the liver. The portal vein is confluence of the splenic vein and the superior mesenteric vein, which drain the intestines, pancreas, stomach, and spleen.
The primary venous drainage of the liver is through three large hepatic veins that enter the inferior vena cava adjacent to the diaphragm. The right hepatic vein is generally oval in shape, with its long axis in the line of the vena cava. The middle and left hepatic veins enter the inferior vena cava through a single orifice in about 60% of individuals. In addition, there are 10-50 small hepatic veins that drain directly into the vena cava.
The biliary anatomy of the liver generally follows hepatic arterial divisions. The common bile duct gives off the cystic duct and becomes the hepatic duct. The hepatic duct then divides into two or three additional ducts draining the liver. There is significant variation in the biliary anatomy, and thus, careful preoperative imaging is vital before any major hepatic resection. [5]
The vascular anatomy of the liver defines its functional segments. Bismuth synthesized existing knowledge and new insight into the anatomy of the liver. [7] Bismuth defined the right and left hemilivers, which are defined by a line connecting the gallbladder fossa and the inferior vena cava, roughly paralleling the middle hepatic vein that is slightly to the left. [7]
The right hemiliver (lobe) is divided into four segments (ie, 5, 6, 7, 8), each of which is supplied by a branch of the portal vein. The right hemiliver drains via the right hepatic vein. The left hemiliver (lobe) is composed of three segments (ie, 2, 3, 4). Segment 4 is the most medial and is adjacent to the middle hepatic vein. Segments 2 and 3 make up the left lateral section, are to the left of the falciform ligament, and drain via the left hepatic vein. Finally, segment 1 (caudate lobe) is located behind the porta hepatis and adjacent to the vena cava.
In general, resection of the liver is divided into the following two main categories [8] :
-
Nonanatomic (wedge) resections are generally limited resections of a small portion of liver, without respect to the vascular supply
-
Anatomic resections involve removing one or more of the eight segments of the liver
Commonly, a right hepatectomy refers to the removal of segments 5-8, an extended right hepatectomy (right trisectionectomy) includes segments 4-8, a left hepatectomy includes segments 2-4, and an extended left hepatectomy (left trisectionectomy) includes segments 2, 3, 4, 5, and 8. A left lateral sectionectomy includes only segments 2 and 3. The caudate lobe can be removed as an isolated resection or as a component of one of the more extensive resections noted above. The extent of resection that can be tolerated is based upon the health of the remnant liver.
Pathophysiology
The pathophysiology of HCC has not been definitively elucidated and is clearly a multifactorial event. In 1981, after Beasley linked hepatitis B virus (HBV) infection to HCC development, the cause of HCC was thought to have been identified. [9] However, subsequent studies failed to identify HBV infection as a major independent risk factor, and it became apparent that most cases of HCC developed in patients with underlying cirrhotic liver disease of various etiologies, including patients with negative markers for HBV infection.
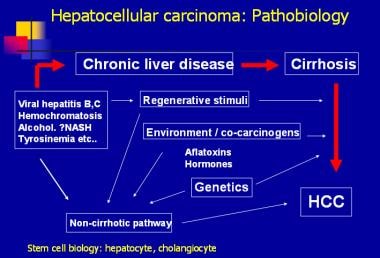
The disease processes, which result in malignant transformation, include a variety of pathways, many of which may be modified by external and environmental factors and eventually lead to genetic changes that delay apoptosis and increase cellular proliferation (see the image below).
Inflammation, necrosis, fibrosis, and ongoing regeneration characterize the cirrhotic liver and contribute to HCC development. In patients with HBV, in whom HCC can develop in livers that are not frankly cirrhotic, underlying fibrosis is usually present, with the suggestion of regeneration. By contrast, in patients with hepatitis C virus (HCV) infection, HCC almost invariably presents in the setting of cirrhosis. This difference may relate to the fact that HBV is a DNA virus that integrates in the host genome and produces HBV X protein, which may play a key regulatory role in HCC development by promoting cell proliferation. [10] HCV is an RNA virus that replicates in the cytoplasm and does not integrate in the host DNA.
Some of the factors associated with the development of HCC in HBV-infected individuals are as follows [11] :
-
Elevated serum HBV DNA viral load
-
HBV genotype – Risk of HCC appears to be higher with HBV genotypes C and F
-
HBV mutations – Such as in preS, basic core promoter ( BCP), or HBx regions
-
Host factors – Such as polymorphisms in KIF1B, HLA-DQ, STAT4, and GRIK1
-
HBV integration into growth-control genes (eg, TERT), pro-oncogenic genes, or tumor suppressor genes and the oncogenic activity of truncated HBx
Genomic sequencing studies for HCC have been performed, and potential driver genes in HCC have been catalogued. Frequently mutated genes identified in large-scale studies, and their functions, include the following [12] :
-
T ERT - Maintaining telomere length
-
TP53 - Tumor suppressor
-
CTNNB1 - Transcriptional regulator
-
ARID1A, ARID2 [13] - Chromatin remodeling
Whereas various nodules are frequently found in cirrhotic livers, including dysplastic and regenerative nodules, no clear progression from these lesions to HCC occurs. Prospective studies suggest that the presence of small-cell dysplastic nodules conveyed an increased risk of HCC, but large-cell dysplastic nodules were not associated with an increased risk of HCC. Evidence linking small-cell dysplastic nodules to HCC includes the presence of conserved proliferation markers and the presence of nodule-in-nodule on pathologic evaluation. This term describes the presence of a focus of HCC in a larger nodule of small dysplastic cells. [14]
Some investigators have speculated that HCC develops from hepatic stem cells that proliferate in response to chronic regeneration caused by viral injury. [15] The cells in small dysplastic nodules appear to carry markers consistent with progenitor or stem cells.
Tumors are multifocal within the liver in 75% of cases. Late in the disease, metastases may develop in the lung, portal vein, periportal nodes, bone, or brain (see images below).
 Hepatocellular carcinoma (HCC). Dilated collateral superficial abdominal veins in a 67-year-old man with cirrhosis, HCC, and portal vein occlusion.
Hepatocellular carcinoma (HCC). Dilated collateral superficial abdominal veins in a 67-year-old man with cirrhosis, HCC, and portal vein occlusion.
Etiology
Cirrhosis
In general, cirrhosis of any etiology is the major risk factor for HCC. [16, 17] About 80% of patients with newly diagnosed HCC have preexisting cirrhosis. Major causes of cirrhosis in the United States are nonalcoholic fatty liver disease (NAFLD), alcohol abuse, hepatitis C infection, and hepatitis B infection. [2]
Metabolic factors
Obesity and diabetes have been implicated as risk factors for HCC, most likely through the development of nonalcoholic steatohepatitis (NASH). [18, 19, 20] In the analysis of a large managed care database, the incidence of HCC linked to nonalcoholic fatty liver disease rose by 10 times from 0.03-0.46 per 100,000 between the years 1997 and 2005. [21] Currently, nonalcoholic fatty liver disease constitutes the main risk factor for HCC in the United States. [2, 3, 22]
Alcohol
In the United States, about 30% of HCC cases are thought to be related to excessive alcohol use. Chronic alcohol use (> 80 g/d or > 6-7 drinks per day) for more than 10 years increases risk of HCC 5-fold.
Approximately 50% of US HCC patients have histories of alcohol abuse. As many as 50% of alcoholics may have subclinical HCC at autopsy.
Alcohol abusers are at increased risk of HCC if they stop drinking alcohol, because heavy drinkers typically do not survive long enough to develop cancer. The risk of HCC in patients with decompensated alcoholic cirrhosis is approximately 1% per year.
Hepatitis B virus infection
The global prevalence of chronic hepatitis B virus (HBV) infection was estimated to be 296 million persons in 2019 [23] ; chronic HBV infection is the most common cause of HCC worldwide. In the United States, about 20% of HCC cases are thought to be related to chronic HBV infection. Chronic HBV infection in the setting of cirrhosis increases the risk of HCC 1000-fold. The mechanism by which HBV causes HCC is thought to be from a combination of chronic inflammation and integration of the viral genome into the host DNA.
It is anticipated that with implementation of worldwide vaccination, the incidence of hepatitis B–related HCC will decrease. In a study from Taiwan, where universal hepatitis B vaccination in newborns and children was instituted in 1984, the average annual incidence of HCC per 100,000 children age 6-14 years declined from 0.70 in 1981-1986 to 0.36 in 1990-1994 (P < 0.01). [24] By the end of 2022, hepatitis B vaccine for infants had been introduced nationwide in 190 countries; in addition,113 countries had introduced one dose of hepatitis B vaccine to newborns within the first 24 hours of life. Estimated global coverage was 45%, ranging from 18% in the World Health Organization (WHO) African region to 80% in the WHO Western Pacific Region. [25]
Hepatitis C virus infection
Hepatitis C virus (HCV) infection is a global pandemic affecting 58 million persons. [23] Approximately 80% of individuals infected with HCV develop chronic infection; this rate is higher than occurs with HBV infection.
HCV infection has become the most common cause of HCC in Japan and Europe, and it is also responsible for the recent increased incidence in the United States. [6] More than 3 million Americans have chronic HCV infection. In the United States, about 30% of HCC cases are thought to be related to HCV infection. Some 5-30% of individuals with HCV infection develop chronic liver disease. In this group, about 30% progress to cirrhosis, and in these, about 1-2% per year develop HCC.
The lifetime risk of HCC in patients with HCV is approximately 5%, appearing 30 years after infection. However, studies suggest that antiviral treatment of chronic HCV infections may significantly reduce the risk of HCC. [26]
Co-infection with HBV further increases the risk; many patients are co-infected with both viruses. Alcohol use in the setting of chronic HCV doubles the risk of HCC compared with HCV infection alone.
Hemochromatosis
Patients with hemochromatosis, especially in the presence of cirrhosis, are at an increased risk of developing HCC. About 30% of all iron-related deaths in hemochromatosis are due to HCC.
Aflatoxin
This hepatic carcinogen is a byproduct of fungal contamination of foodstuffs in sub-Saharan Africa and East and Southeast Asia. Aflatoxin causes DNA damage and mutations of the p53 gene. Humans are exposed through the ingestion of moldy foods found in susceptible grains. Dietary levels in endemic areas correlate directly with incidence of hepatocellular carcinoma.
Rare associations
These include the following:
-
Androgenic steroids
-
Thorotrast radioactive contrast
-
Oral contraceptives
Epidemiology
In the United States, liver cancer is the most rapidly increasing cancer in both men and women, with incidence rates more than tripling since 1980; from 2006 to 2015, the rate increased by about 3% per year. For 2024, the American Cancer Society (ACS) estimates that 41,630 new cases of liver cancer (including intrahepatic bile duct cancers) will be diagnosed; approximately three-fourths of those will be HCC. [27]
Liver and intrahepatic bile duct cancers are the 13th most common type of cancer, [28] but are the fifth most common cause of cancer deaths in men in the US, and the seventh most common in women. [27] The ACS estimates that 29,840 deaths will occur from liver cancer in 2024. [27] According to Surveillance, Epidemiology, and End Results (SEER) program data, liver and intrahepatic bile duct cancers account for 2.1% of all new cancer cases but 4.8% of all cancer deaths. [28]
In the US, the median age at diagnosis is 66 years. Most cases occur in men: Incidence rates per 100,000 persons are 14.1 in men and 5.2 in women. Incidence rates increase with age; 31.6% of cases are in persons age 55-64 years and 33.7% in those 65-74 years. [28] Globally, the incidence of liver cancer among men and women who are younger than 30 years and those aged 30 to 59 years has declined, largely due to national hepatitis B virus (HBV) vaccination programs. [29]
By racial and ethnic group, rates are highest in American Indian/Alaska Natives, followed by Hispanics, Asians/Pacific Islanders, then Blacks, and whites. [28]
Worldwide, liver cancer was the sixth most common cancer and the third most common cause of cancer deaths in 2020, with an estimated 905,677 new cases and 830,180 deaths. The incidence was highest in East Asia, at 17.9 per 100,000 population (26.9 in males and 8.9 in females), followed by Micronesia, northern Africa, Southeast Asia, and Melanesia. The incidence was lowest in south-central Asia (3.0 per 100,000) and South America (4.4 per 100,000). By comparison, the incidence rate was 6.9 per 100,00 in northern America and 5.6 per 100,000 in western Europe. Overall, the incidence rate of liver cancer is approximately three times higher in males than in females. Mortality figures mirror the incidence figures. [1]
In the United Kingdom, both the incidence and mortality rates of hepatocellular carcinoma (HCC) have risen dramatically. From 1997 to 2017, incidence rates of HCC increased 5.9% per year, rising from 3.03 to 9.22 per 100,000 in men, and from 0.87 to 2.17 per 100,000 in women. Mortality rates per 100,000 population rose from 2.11 to 6.74 in men, and from 0.69 to 1.61 in women. [30]
Steady declines in HCC mortality are predicted for East Asia. In contrast, Northern and Central Europe, North America, and Latin America are showing unfavorable trends. [31] According to an analysis of data from the Global Burden of Disease (GBD) Study, the number of liver cancer cases increased nearly threefold in older men and more than twofold in older women (aged 60 years or more) from 1990 to 2017. The increase consisted mainly of cases secondary to nonalcoholic steatohepatitis (NASH; popularly known as fatty liver disease). [29]
Prognosis
Overall prognosis for survival is poor, with a 5-year relative survival rate of 21.6%. By stage, the relative 5-year survival is 37.3% in patients diagnosed with localized disease, 14.3% with regional disease, and 3.5% with distant disease. [28] Length of survival depends largely on the extent of cirrhosis in the liver; cirrhotic patients have shorter survival times and more limited therapeutic options. Portal vein occlusion, which occurs commonly, portends an even shorter survival. As many patients die of liver failure as from tumor progression.
The influence of diabetes, obesity, and glycemic control continues to be evaluated in studies of the etiology and outcomes of HCC. For example, in a study of patients who had undergone curative resection for solitary HCV-related HCC, the tumor-free survival rate at 3 years was more than twice as high in patients in patients who had a normal hemoglobin A1c than in those whose hemoglobin A1c was 6.5% or higher (66% versus 27%). [32]
Complications from HCC are those of hepatic failure; death occurs from cachexia, variceal bleeding, or (rarely) tumor rupture and bleeding into the peritoneum. Signs and symptoms of hepatic failure may signify tumor recurrence and/or progression.
Various studies have reported extrahepatic metastasis in up to 30–50% of cases of HCC, with lungs the commonest site, followed by lymph nodes and bones. Unusual extrahepatic metastatic sites include the following [33] :
-
Adrenal glands
-
Peritoneum
-
Diaphragm
-
Soft tissues
-
Brain
-
Skin
-
Oral cavity
-
Large hepatocellular carcinoma. Image courtesy of Arief Suriawinata, MD, Department of Pathology, Dartmouth Medical School.
-
Photomicrograph of a liver demonstrating hepatocellular carcinoma. Image courtesy of Arief Suriawinata, MD, Department of Pathology, Dartmouth Medical School.
-
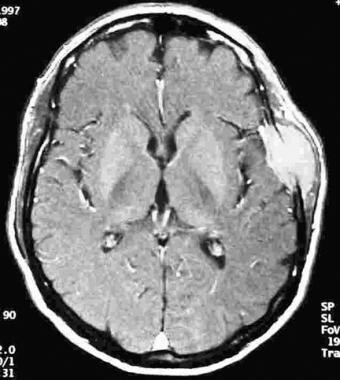
MRI of a liver with hepatocellular carcinoma.
-
Ultrasonographic image of hepatocellular carcinoma.
-
Arterial phase CT scan demonstrating enhancement of hepatocellular carcinoma.
-
Portal venous phase CT scan demonstrating washout of hepatocellular carcinoma.
-
The Barcelona-Clinic Liver Cancer (BCLC) approach to hepatocellular carcinoma management. Adapted from Llovet JM, Fuster J, Bruix J, Barcelona-Clinic Liver Cancer Group. The Barcelona approach: diagnosis, staging, and treatment of hepatocellular carcinoma. Liver Transpl. Feb 2004;10(2 Suppl 1):S115-20.
-
Hepatocellular carcinoma: pathobiology.
-
Right hepatectomy. Part 1: Dissection of portal vein. Courtesy of Memorial Sloan-Kettering Cancer Center, featuring Leslie H. Blumgart, MD. (From Blumgart LH. Video Atlas: Liver, Biliary & Pancreatic Surgery. Philadelphia, PA: Saunders; 2010.)
-
Right hepatectomy. Part 2: Devascularization of right liver. Courtesy of Memorial Sloan-Kettering Cancer Center, featuring Leslie H. Blumgart, MD. (From Blumgart LH. Video Atlas: Liver, Biliary & Pancreatic Surgery. Philadelphia, PA: Saunders; 2010.)
-
Right hepatectomy. Part 3: Suturing and dividing. Courtesy of Memorial Sloan-Kettering Cancer Center, featuring Leslie H. Blumgart, MD. (From Blumgart LH. Video Atlas: Liver, Biliary & Pancreatic Surgery. Philadelphia, PA: Saunders; 2010.)
-
Hepatocellular carcinoma (HCC). Dilated collateral superficial abdominal veins in a 67-year-old man with cirrhosis, HCC, and portal vein occlusion.
-
Hepatocellular carcinoma. Plain radiograph immediately following chemoembolization, demonstrating catheter placement and Ethiodol enhancement of tumors.
Tables
Alpha-Fetoprotein (ng/mL) |
Interpretation |
> 400-500 |
- HCC likely if accompanied by space-occupying solid lesion(s) in cirrhotic liver or levels are rapidly increasing. - Diffusely growing HCC, may be difficult to detect on imaging. - Occasionally in patients with active liver disease (particularly HBV or HCV infection) reflecting inflammation, regeneration, or seroconversion |
Normal value to < 400 |
- Frequent: Regeneration/inflammation (usually in patients with elevated transaminases and HCV) - Regeneration after partial hepatectomy - If a space-occupying lesion and transaminases are normal, suspicious for HCC |
Normal value |
Does not exclude HCC (cirrhotic and noncirrhotic liver) |
Author (Year) |
N |
Survival Rate |
|
1 year |
5 years |
||
Mazzefero (1996) |
48 |
84% |
74% |
Bismuth (1999) |
45 |
82% |
74% |
Llovet (1999) |
79 |
86% |
75% |
Jonas (2001) |
120 |
90% |
71% |
Stage |
Criteria |
0 – Very Early |
Child-Pugh class A Single < 2 cm nodule ECOG PS 0-1 |
A – Early |
Child-Pugh class A-B Single or 2-3 nodules < 3 cm ECOG PS 0-1 |
B – Intermediate |
Child-Pugh class A-B Multinodular ECOG PS 0-1 |
C - Advanced |
Child-Pugh class A-B Portal vein invasion, N1, M1 ECOG PS 0-2 |
D - Terminal |
Child-Pugh class C Any T, N, or M ECOG PS > 2 |
ECOG PS = Eastern Cooperative Oncology Group Performance Status |
|







