Practice Essentials
Trigonitis is a pathological process of the bladder trigone characterized by nonkeratinizing squamous metaplasia (see the image below). Anatomically, the trigone occupies the region between the ureteric ridge and the bladder neck. Histologically, the bladder trigone is normally lined by urothelium, a type of transitional epithelial tissue found throughout the urinary tract. [1]
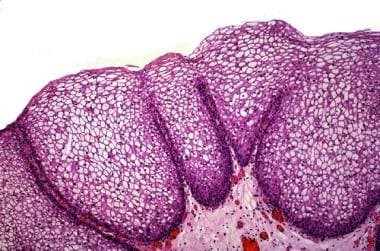 Nonkeratinizing squamous metaplasia. Stratified squamous metaplasia is usually seen in the bladder neck and trigone. Note the lack of densely eosinophilic layer, representing keratin, at the luminal side.
Nonkeratinizing squamous metaplasia. Stratified squamous metaplasia is usually seen in the bladder neck and trigone. Note the lack of densely eosinophilic layer, representing keratin, at the luminal side.
Trigonitis was first described in 1905 by Heymann, who called the disorder cystitis trigoni. [2] Subsequently, Cifuentes described trigonitis as a true trigonal membrane. [3] It is also referred to in the scientific literature as pseudomembranous trigonitis or vaginal metaplasia.
Squamous metaplasia of the trigone has been observed almost exclusively in women of childbearing age. It is almost nonexistent in children. Although the exact etiology of trigonitis is unknown, the condition usually occurs in response to an irritative insult to the bladder trigone (eg, from a long-term indwelling catheter) or an infectious process.
Patients with squamous metaplastic changes in the bladder may be asymptomatic or may present with irritative voiding symptoms. Diagnosis of trigonitis requires cystoscopy (see Workup). Asymptomatic patients do not require treatment. Several treatment approaches have been tried in patients with symptomatic trigonitis, including medications and surgery. See Treatment.
Trigonitis is a benign lesion that does not carry malignant potential. Expertise and scientific data indicate that follow-up cystoscopy after diagnosis is not required. However, urologists should make it a point of emphasis to distinguish trigonitis from keratinizing squamous metaplasia, also known as leukoplakia, which does carry malignant potential.
For patient education information, see Bladder Cancer.
Pathophysiology
Trigonitis, although its name suggests inflammation, is a metaplastic process. The precise underlying cause is not known, but squamous metaplasia in the bladder usually occurs in response to irritation (eg, from a long-term indwelling catheter) or infection. Given that nonkeratinizing squamous metaplasia is commonly found in adult women of childbearing age, a hormonal component is often considered likely.
In a study of bladder biopsies performed in women with pseudomembranous trigonitis and women who underwent cystoscopy for staging gynecological cancer, estrogen and progesterone receptors were found in the trigone in association with squamous metaplastic changes. [4] In a more extensive mapping study of the female lower urinary tract, both estrogen and progesterone receptors were found in squamous epithelial tissue, including the transitional cell epithelium in the trigone and proximal urethra that had undergone squamous metaplastic changes. [5]
In the first case report of pseudomembranous trigonitis in a patient with Klinefelter syndrome (a 16-year-old boy), the findings of raised estrogen levels in conjunction with increased expression of estrogen receptors in the trigone area, but not the remainder of the bladder, suggest that estrogen could be an etiological driver, much like the association of Klinefelter syndrome with estrogen-driven cancers such as breast cancer. [6] Trigonitis has been reported in men receiving estrogen therapy for the treatment of prostate cancer. [7]
However, whether hormonal influences lead to squamous metaplasia is unclear. Other authors have suggested that squamous cell metaplasia is not associated with increased estrogen activity. [8] Kvist et al did not find estrogen receptors in 36 historically collected samples of squamous metaplasia of the bladder urothelium, although these authors posited that if only relatively few receptors had been present initially, they might have been destroyed in the tissue preparation process. [8]
Instead, other explanations focus on the potential role of chronic inflammation and/or a deficient urothelium. In one autopsy study of adult women, histological evidence of chronic inflammation was found significantly more often in bladders with squamous metaplasia. The authors suggest that squamous metaplasia is not a consequence of chronic inflammation but rather that its surface characteristics may predispose to chronic infection. [9]
Squamous metaplasia is observed over edematous or inflamed lamina propria. [10] Electron microscopy of the keratinizing variant has demonstrated that squamous metaplastic cells lack the tight junctions seen in normal transitional epithelial cells, which might allow urine to permeate the subepithelial layers, resulting in ongoing inflammation. [11]
Bacterial cystitis has been associated with the development of trigonitis in cases of recurrent urinary tract infections. The literature regarding interstitial cystitis suggests that the mucosal coating of the bladder surface, also known as the glycosaminoglycan (GAG) layer, plays a profound role in preventing urinary solutes from permeating into the urothelium of the bladder wall. [12] Restriction of the characteristic lesion to the trigone of the bladder is possibly due to the estrogenic effect. This restriction could be explained by the fact that the trigone is anatomically and embryologically distinct from the remainder of the bladder. [13]
Defects in this protective mechanism, or injuries resulting from chronic irritation or recurrent infections, may result in chronic inflammatory changes leading to metaplasia. However, not all individuals with squamous metaplasia are symptomatic, and not all symptomatic patients have squamous metaplasia, which complicates understanding of this elusive disease process.
Epidemiology
The frequency of trigonitis differs in various reports, but the literature consistently shows that trigonitis occurs almost exclusively in women of childbearing age. Nonkeratinizing squamous metaplasia of the bladder neck and trigone can be seen in 50-70% of premenopausal women and is considered a normal variant. [11]
In a study by Wiener et al that examined 100 grossly normal bladders at autopsy, 46% of premenopausal and postmenopausal women were to found to have squamous metaplasia; in comparison, only 7% of men were found to have squamous metaplasia of the bladder. [14] In an autopsy study of bladders from 106 women who had died of diseases unrelated to the urinary tract, 72% exhibited squamous metaplasia in the trigone. [9] Other reports suggest that trigonitis occurs in approximately 40% of adult women and approximately 5% of men. [15] Trigonitis may also be seen in men receiving hormonal therapy for prostate cancer. [7]
-
Keratinizing squamous metaplasia of the bladder.
-
Cystoscopic appearance of trigonitis as a well-defined white area overlying the trigone.
-
Nonkeratinizing squamous metaplasia. Stratified squamous metaplasia is usually seen in the bladder neck and trigone. Note the lack of densely eosinophilic layer, representing keratin, at the luminal side.








