Practice Essentials
Sjögren syndrome is a systemic chronic inflammatory disorder characterized by lymphocytic infiltrates in exocrine organs. The disorder most often affects women, and the median age of onset is around 50 to 60 years. Most individuals with Sjögren syndrome present with sicca symptoms, such as xerophthalmia (dry eyes), xerostomia (dry mouth), and parotid gland enlargement, which is seen in the image below. [1] (See Presentation.)
 Marked bilateral parotid gland enlargement in a patient with primary Sjögren syndrome. Sicca syndrome is a common clinical finding. (C) 1972-2004 American College of Rheumatology Clinical Slide Collection. Used with permission.
Marked bilateral parotid gland enlargement in a patient with primary Sjögren syndrome. Sicca syndrome is a common clinical finding. (C) 1972-2004 American College of Rheumatology Clinical Slide Collection. Used with permission.
In addition, numerous extraglandular features may develop, such as the following:
-
Arthralgia
-
Arthritis
-
Myalgia
-
Pulmonary disease
-
Gastrointestinal disease
-
Leukopenia
-
Anemia
-
Lymphadenopathy
-
Neuropathy
-
Vasculitis
-
Renal tubular acidosis
-
Lymphoma
About 50% of patients with Sjögren syndrome have cutaneous findings, such as dry skin (xeroderma), palpable and nonpalpable purpura, and/or urticaria. [1] (See Etiology, Presentation, and Workup.)
Primary Sjögren syndrome occurs in the absence of another underlying rheumatic disorder, whereas secondary Sjögren syndrome is associated with another underlying rheumatic disease, such as systemic lupus erythematosus (SLE), rheumatoid arthritis (RA), or scleroderma. Given the overlap of Sjögren syndrome with many other rheumatic disorders, it is sometimes difficult to determine whether a clinical manifestation is solely a consequence of Sjögren syndrome or is due to one of its overlapping disorders.
Importantly, classic clinical features of Sjögren syndrome may also be seen in infections with certain viruses. These include hepatitis C virus, human immunodeficiency virus (HIV), and human T-cell lymphotrophic virus (HTLV). (See DDx.)
Most patients with primary Sjogren syndrome have two specific antibodies: against Ro (SS-A) and La (SSB) antigens. (See Workup.)
Treatment for Sjögren syndrome is largely based on symptoms (eg, lotion for dry skin, artificial tears for dry eyes). Rituximab has shown promise in the treatment of severe extraglandular manifestations (eg, vasculitis, cryoglobulinemia, peripheral neuropathy). Patients must be monitored carefully for the potential development of lymphoma, as the risk for this disease is significantly higher than in the general population. (See Treatment and Medication.)
For more information on other aspects of Sjögren syndrome, see Pediatric Sjögren Syndrome and Ophthalmologic Manifestations of Sjögren Syndrome.
Classification criteria
A number of classification criteria for Sjögren syndrome were designed primarily for clinical research studies but are also often used to help guide clinical diagnoses. The American-European Consensus Group’s criteria for the classification of Sjögren syndrome were proposed in 2002 and are the most commonly used criteria for the diagnosis of Sjögren syndrome. A new set of classification criteria was developed by the Sjögren’s International Collaborative Clinical Alliance (SICCA) investigators and accepted as a provisional criteria set by the American College of Rheumatology (ACR) in 2012.
In 2012, investigators from the SICCA team and the EULAR Sjögren’s Task Force formed the International Sjögren’s Syndrome Criteria Working Group. The Task Force's work was published in 2016 as ACR/European League Against Rheumatism (EULAR) classification criteria for primary Sjögren syndrome. [2]
American-European Consensus Group classification
The American-European Consensus Group (AECG) criteria for the classification of Sjögren syndrome are outlined below. [3, 4] These criteria allow a diagnosis of Sjögren syndrome in patients without sicca symptoms or who have not undergone a biopsy.
According to the American-European classification system (as modified by Tzioufas and Voulgarelis [5] ), diagnosis of primary Sjögren syndrome requires at least four of the criteria listed below; in addition, either criterion number 5 or criterion number 6 must be included. Sjögren syndrome can be diagnosed in patients who have no sicca symptoms if three of the four objective criteria are fulfilled. The criteria are as follows:
- Ocular symptoms - Dry eyes for more than 3 months, foreign-body sensation, use of tear substitutes more than 3 times daily
Oral symptoms - Feeling of dry mouth, recurrently swollen salivary glands, frequent use of liquids to aid swallowing
Ocular signs - Schirmer test performed without anesthesia (< 5 mm in 5 min), positive vital dye staining results
Oral signs - Abnormal salivary scintigraphy findings, abnormal parotid sialography findings, abnormal sialometry findings (unstimulated salivary flow < 1.5 mL in 15 min)
Positive minor salivary gland biopsy findings
Positive anti–SSA or anti–SSB antibody results
Secondary Sjögren syndrome is diagnosed when, in the presence of a connective-tissue disease, symptoms of oral or ocular dryness exist in addition to criterion 3, 4, or 5, above.
Application of these criteria has yielded a sensitivity of 97.2% and a specificity of 48.6% for the diagnosis of primary Sjögren syndrome. For secondary Sjögren syndrome, the specificity is 97.2% and the sensitivity, 64.7%. [6]
Exclusion criteria include any of the following:
-
Past head-and-neck irradiation
-
Hepatitis C virus infection
-
Acquired immunodeficiency syndrome (AIDS)
-
Prior lymphoma
-
Sarcoidosis
-
Graft versus host disease
-
Use of anticholinergic drugs
ACR/EULAR classification criteria for primary Sjogren syndrome
According to the ACR/EULAR classification criteria, individuals are classified as having primary Sjögren syndrome if they have a total score of 4 or higher, derived from the sum of the weights assigned to the following [2] :
-
Focal lymphocytic sialadenitis and focus score of ≥1 foci/4 mm² in labial salivary gland biopsy samples – weight/score 3
-
Anti-SSA/Ro positive – weight/score 3
-
Ocular Staining Score ≥5 (or van Bijsterveld score ≥4) in at least one eye – weight/score 1
-
Schirmer’s test ≤5 mm/5 min in at least one eye – weight/score 1
-
Unstimulated whole saliva flow rate ≤0.1 mL/min – weight/score 1
For inclusion, patients must have at least one symptom of ocular or oral dryness, defined as a positive response to at least one of the following questions:
-
Have you had daily, persistent, troublesome dry eyes for more than 3 months?
-
Do you have a recurrent sensation of sand or gravel in the eyes?
-
Do you use tear substitutes more than three times a day?
-
Have you had a daily feeling or dry mouth for more than 3 months?
-
Do you frequently drink liquids to aid in swallowing dry food?
Exclusion criteria include any of the following:
-
History of head-and-neck radiation treatment
-
Active hepatitis C infection (with confirmation by polymerase chain reaction [PCR]) testing
-
AIDS
-
Sarcoidosis
-
Amyloidosis
-
Graft versus host disease
-
IgG4-related disease
Complications
Complications related to Sjögren syndrome include the following (see Prognosis, Treatment, and Medication):
-
Emergence of disorders associated with Sjögren syndrome, such as SLE and RA
-
Infection of the parotid gland, typically staphylococcal, streptococcal, or pneumococcal - clues include unilateral worsening of symptoms, along with tenderness, warmth, and erythema
-
Emergence of parotid tumors - watch for unusually hard or unilateral parotid enlargement
-
Pregnant patients with antiRo/SS-A antidodies are at risk for fetal loss, complete heart block in the fetus ,and neonatal lupus syndrome in the newborn
-
Emergence of pseudolymphomas (pleomorphic cells that do not meet the criteria for malignancy) and non-Hodgkin B-cell lymphomas (see the image below) [5]
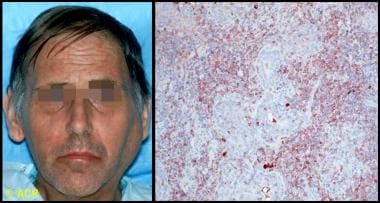 Clinical photograph and photomicrograph of a 48-year-old man with Sjögren syndrome with a large left parotid mass. On biopsy, B-cell lymphoma of mucosa-associated lymphoid tissue (MALT) type was identified. Microscopic section of parotid biopsy, stained with immunoperoxidase for kappa light chains (brown-stained cells), showed monoclonal population of B cells, confirming the diagnosis. (C) 1972-2004 American College of Rheumatology Clinical Slide Collection. Used with permission.
Clinical photograph and photomicrograph of a 48-year-old man with Sjögren syndrome with a large left parotid mass. On biopsy, B-cell lymphoma of mucosa-associated lymphoid tissue (MALT) type was identified. Microscopic section of parotid biopsy, stained with immunoperoxidase for kappa light chains (brown-stained cells), showed monoclonal population of B cells, confirming the diagnosis. (C) 1972-2004 American College of Rheumatology Clinical Slide Collection. Used with permission.

Patient education
Educate patients with Sjögren syndrome on avoidance strategies and self-care issues for the treatment of dry mouth, eyes, skin, and vagina. Patient education pamphlets regarding the disease are available through the Arthritis Foundation. The Sjögren’s Syndrome Foundation, founded in 1983, is a good resource for patients.
For patient education information, see the Arthritis Center, as well as Sjögren’s Syndrome.
Etiology
The etiology of Sjögren syndrome is not well understood. The presence of activated salivary gland epithelial cells expressing major histocompatibility complex (MHC) class II molecules and the identification of inherited susceptibility markers suggest that environmental or endogenous antigens trigger a self-perpetuating inflammatory response in susceptible individuals. In addition, the continuing presence of active interferon pathways in Sjögren syndrome suggests ongoing activation of the innate immune system. [7, 8] Together, these findings suggest an ongoing interaction between the innate and acquired immune systems in Sjögren syndrome.
Association with the human leukocyte antigen
The frequency of HLA-DR52 in patients with primary Sjögren syndrome is estimated to be 87%, but it is also significantly increased in secondary Sjögren syndrome that occurs with rheumatoid arthritis or systemic lupus erythematosus.
The genetic associations in Sjögren syndrome vary among ethnic groups. In White persons, for instance, the condition is linked to human leukocyte antigen (HLA)–DR3, HLA-DQ2, and HLA-B8, [9] whereas the linkage is to HLA-DRB1*15 in Spanish persons [10] and to HLA-DR5 in Greek and Israeli persons. [11]
Some evidence indicates that the true association of Sjögren syndrome may be with HLA-DQA1, which is in linkage disequilibrium with HLA-DR3 and HLA-DR5. [12] These HLA associations appear restricted to individuals with Sjögren syndrome who have antibodies to the antigens SSA and SSB rather than to the disease manifestations themselves. [13]
Environmental triggers
Viruses are viable candidates as environmental triggers, although proof of causation has remained elusive, and certainly no single virus has been implicated. Epstein-Barr virus (EBV), HTLV-1, human herpesvirus 6 (HHV-6), HIV, hepatitis C virus (HCV), and cytomegalovirus (CMV) may have a role. Sjögrenlike syndromes are seen in patients infected with HIV, HTLV-1, and hepatitis C. [14, 15, 16] An increase of more than 50% in newly diagnosed primary Sjögren syndrome was reported in Brazil during 2020, with more cases reported during the months following the first wave of COVID-19 cases. [17]
Damage and/or cell death due to viral infection or other causes may provide triggering antigens to Toll-like receptors in or on dendritic or epithelial cells, which, by recognizing pathogen-associated patterns, are activated and begin producing cytokines, chemokines, and adhesion molecules. As T and B lymphocytes migrate into the gland, they themselves become activated by dendritic and epithelial cells, thereafter acting as antigen-presenting cells. [18]
Expressed antigens include SSA/Ro, SSB/La, alpha-fodrin and beta-fodrin, and cholinergic muscarinic receptors. [13] Dendritic cell triggering by immune complexes formed from SSA ̶ anti-SSA (or other immune complexes) may propagate the ongoing innate and acquired immune activation.
A population-based cohort study of Taiwanese residents found that exposure to carbon monoxide (CO), nitric oxide (NO), and methane (CH4) was associated with a higher risk of developing primary Sjögren syndrome. [19]
Epidemiology
In the United States, Sjögren syndrome is estimated to be the second most common rheumatologic disorder, behind SLE. Sjögren syndrome affects 0.1-4% of the population. This wide range, in part, reflects the lack of uniform diagnostic criteria. [20] Internationally, comparative studies between different ethnic groups have suggested that Sjögren syndrome is a homogeneous disease that occurs worldwide with similar prevalence and affects 1-2 million people.
The female-to-male ratio of Sjögren syndrome is 9:1. Sjögren syndrome can affect individuals of any age but is most common in elderly people. Onset typically occurs in the fourth to fifth decade of life.
The systemic phenotype of primary Sjögren syndrome is strongly influenced by personal factors (eg, age, gender, ethnicity, place of residence, according to an analysis by the Sjögren Big Data Consortium, a five-continent multicenter registry, of a cohort that included 10,007 patients (9352 female, mean age 53 years) with recorded European League Against Rheumatism's Sjögren syndrome disease activity index (ESSDAI) scores available. [21] Findings (all P < 0.001) were as follows:
-
Males had a higher mean ESSDAI than females (8.1 vs 6.0, respectively).
-
Patients diagnosed at < 35 years had a higher mean ESSDAI than those diagnosed at > 65 years (6.7 vs 5.6).
-
By ethnicity, the highest global ESSDAI scores were reported in blacks/African Americans (6.7), followed by whites (6.5), Asians (5.4), and Hispanics (4.8).
-
Black/African-American patients showed the highest frequencies in the lymphadenopathy, articular, peripheral and central nervous system, and biological domains.
-
White patients showed the highest frequencies in the glandular, cutaneous, and muscular domains.
-
Asian patients showed the highest frequencies in the pulmonary, renal, and hematological domains.
-
Hispanic patients showed the highest frequenies in the constitutional domain.
-
Systemic activity and disease activity was higher in patients from southern countries.
Prognosis
Sjögren syndrome carries a generally good prognosis. In patients who develop a disorder associated with Sjögren syndrome, the prognosis is more closely related to the associated disorder (eg, SLE, lymphoma). Interestingly, primary Sjögren syndrome is associated with lower cardiovascular risk factors and lower risk of serious cardiovascular events such as myocardial infarction and stroke, in comparison with SLE. [22]
Although salivary and lacrimal function generally stabilize, the presence of SSA and/or hypocomplementemia may predict a decline in function. [23]
Morbidity and mortality
Morbidity associated with Sjögren syndrome is mainly associated with the gradually decreased function of exocrine organs, which become infiltrated with lymphocytes. The increased mortality rate associated with the condition is primarily related to disorders commonly associated with Sjögren syndrome, such as SLE, RA, and primary biliary cirrhosis. Patients with primary Sjögren syndrome who do not develop a lymphoproliferative disorder have a normal life expectancy. [24]
Lymphoma
Among patients with Sjögren syndrome, the incidence of non-Hodgkin lymphoma is 4.3% (18.9 times higher than in the general population), with a median age at diagnosis of 58 years. The mean time to the development of non-Hodgkin lymphoma after the onset of Sjögren syndrome is 7.5 years.
The most common histologic subtype of non-Hodgkin lymphoma in Sjögren syndrome is mucosa-associated lymphoid tissue (MALT) lymphoma, which can develop in any nonlymphoid tissue infiltrated by periepithelial lymphoid tissue—most commonly the salivary glands, but also the stomach, nasopharynx, skin, liver, kidneys, and lungs. The progression of these infiltrates to lymphoma occurs slowly and in a stepwise fashion. Lymphoma is present at more than 1 site in 20% of patients at initial diagnosis.
The results of one study suggest that diagnostic labial salivary gland tissue biopsy can be used to detect germinal center ̶ like lesions, which can be a highly predictive and easily obtained marker for non-Hodgkin lymphoma in primary Sjögren syndrome patients. [25]
Risk factors for lymphoma include the following:
-
Salivary gland enlargement
-
Regional or generalized lymphadenopathy
-
Hepatosplenomegaly
-
Palpable purpura
-
Leukopenia
-
Renal insufficiency
-
Loss of a previously positive polyclonal gammopathy
-
Development of a monoclonal gammopathy or a monoclonal cryoglobulinemia
-
RF positivity
-
Anti-SSA/SSB positivity
-
Hypocomplementemia
Demographic risk factors for the development of lymphoma include male gender and older age. [26]
Pregnancy complications
Women with Sjögren syndrome are at higher risk for experiencing complications during pregnancy. Worsening of pulmonary hypertension and increased rates of spontaneous abortion and preterm deliveries have been reported. [27]
Children born to mothers with antibodies against SSA/Ro and SSB/La are at an increased risk of neonatal lupus and congenital heart block. [26] If one such child develops congenital heart block, the risk for congenital heart block during a subsequent pregnancy is 15%.
Antiphospholipid syndrome
Patients with Sjögren syndrome who have antiphospholipid antibodies can develop the clinical features of antiphospholipid syndrome, which include increased fetal wastage and vascular thromboses.
Pathophysiology
Sjögren syndrome can occur as a primary disease of exocrine gland dysfunction or in association with several other autoimmune diseases (eg, systemic lupus erythematosus [SLE], rheumatoid arthritis, scleroderma, systemic sclerosis, cryoglobulinemia, polyarteritis nodosa). These primary and secondary types occur with similar frequency, but the sicca complex seems to cause more severe symptoms in the primary form.
Virtually all organs may be involved. The disease commonly affects the eyes, mouth, parotid gland, lungs, kidneys, skin, and nervous system.
Glandular pathology
The pathology of a typical involved salivary or lacrimal gland in Sjögren syndrome reveals aggregations of lymphocytes—periductal at first, then panlobular. These cells are primarily CD4 T cells (75%) and memory cells, with 10% B cells and immunoglobulin-secreting plasma cells. Although individual lobules can be destroyed, salivary gland biopsy samples from patients with Sjögren syndrome typically retain 40%-50% of their viable glandular structure. Therefore, inflammatory destruction of salivary and lacrimal glands may not fully account for the symptoms of Sjögren syndrome. [28]
Studies suggest that the disease process of Sjögren syndrome has a neuroendocrine component. Proinflammatory cytokines released by epithelial cells and lymphocytes may impair neural release of acetylcholine. In addition, antibodies to acetylcholine (muscarinic) receptors may interfere with the neural stimulation of local glandular secretion, [29] perhaps by interfering with aquaporin. [30] Moreover, a study reports that M3 muscarinic receptor antibodies may cause autonomic dysfunction in patients with Sjögren syndrome. [31, 32]
Current studies have also focused on the role of apoptotic mechanisms in the pathogenesis of primary Sjögren syndrome. A defect in Fas-mediated apoptosis, which is necessary for down-regulation of the immune response, can result in a chronic inflammatory destruction of the salivary gland, resembling Sjögren syndrome. [33]
Owing to these structural and functional changes in the lacrimal and salivary glands, their aqueous output is diminished. In the eye, tear hyperosmolarity results and is itself a proinflammatory stimulus, resulting in an inflammatory cascade on the ocular surface, [34] with evidence of immune activation of the conjunctival epithelium and local cytokine and metalloproteinase production. Damage to the corneal epithelium, already vulnerable due to inadequate tear film protection, ensues, with resultant epithelial erosions and surface irregularity.
Extraglandular involvement
Extraglandular involvement in Sjögren syndrome manifests in part as hypergammaglobulinemia and the production of multiple autoantibodies, especially ANA and RF. This may be due to polyclonal B-cell activation, but the cause of this expanded activation is not known.
Involvement of other organs and tissues may result from effects of these antibodies, immune complexes, or lymphocytic infiltration and occurs in one third of patients with Sjögren syndrome. Prolonged hyperstimulation of B cells may lead to disturbances in their differentiation and maturation and may account for the greatly increased incidence of lymphoma in these patients. [35]
Sex hormones
The fact that primary Sjögren syndrome occurs predominantly in women suggests that sex hormones may influence the immunologic manifestations of the disease. The prevalence of serologic markers tends to be lower in male patients than in female patients. Although the role of sex hormones (eg, estrogens, androgens) in the pathogenesis of primary Sjögren syndrome remains unknown, adrenal and gonadal steroid hormone deficiency probably affects immune function.
-
Marked bilateral parotid gland enlargement in a patient with primary Sjögren syndrome. Sicca syndrome is a common clinical finding. (C) 1972-2004 American College of Rheumatology Clinical Slide Collection. Used with permission.
-
Clinical photograph and photomicrograph of a 48-year-old man with Sjögren syndrome with a large left parotid mass. On biopsy, B-cell lymphoma of mucosa-associated lymphoid tissue (MALT) type was identified. Microscopic section of parotid biopsy, stained with immunoperoxidase for kappa light chains (brown-stained cells), showed monoclonal population of B cells, confirming the diagnosis. (C) 1972-2004 American College of Rheumatology Clinical Slide Collection. Used with permission.
-
Photograph that demonstrates the Schirmer test, which is used to detect deficient tear production in patients with Sjögren syndrome. The filter paper strip is placed at the junction of the eyelid margins. After 5 minutes, 15 mm of paper should be moistened if tear production is normal, as shown here. Persons older than 40 years may moisten between 10 mm and 15 mm. Patients with Sjögren syndrome have less moistening. Sjögren syndrome is most common in patients with rheumatoid arthritis but may also occur without associated disease and in systemic lupus erythematosus, polyarteritis, systemic sclerosis, lymphoma, and sarcoidosis. (C) 1972-2004 American College of Rheumatology Clinical Slide Collection. Used with permission.
-
Dryness of the mouth and tongue due to lack of salivary secretion is characteristic of xerostomia associated with Sjögren syndrome. Mouth dryness may produce a deep red tongue, as shown here, and dental caries are common. (C) 1972-2004 American College of Rheumatology Clinical Slide Collection. Used with permission.
-
Photomicrograph of a lip biopsy specimen showing two lymphocytic foci adjacent to normal-appearing mucinous acini typical of minor salivary gland abnormalities in Sjögren syndrome. (C) 1972-2004 American College of Rheumatology Clinical Slide Collection. Used with permission.