Practice Essentials
The term scleroderma is derived from the Greek words skleros (hard or indurated) and derma (skin) and it is used to describe a disease characterized by progressive skin hardening and induration. Scleroderma is an aspect of systemic sclerosis, a systemic connective tissue disease that also involves subcutaneous tissue, muscles, and internal organs.
Diagnosis is based on clinical manifestations, but tests and procedures may be used initiallly to exclude alternative diagnoses, and later for assessment of organ involvement and monitoring of disease progression (see Presentation and Workup). Treatment is directed principally toward managing complications and providing symptomatic relief, but disease-modifying agents are under investigation (see Treatment and Medication).
Background
Definition
The term systemic sclerosis is used to describe a systemic autoimmune disease of unknown origin characterized by excessive deposition of collagen and other connective tissue macromolecules in skin and multiple internal organs, prominent and often severe fibroproliferative alterations in the microvasculature, and numerous humoral and cellular immunologic abnormalities. Although systemic sclerosis is not inherited, a genetic predisposition plays an important role in its development.
Systemic sclerosis is a complex and heterogeneous disease with clinical forms ranging from limited skin involvement (limited cutaneous systemic sclerosis) to forms with diffuse skin sclerosis and severe and often progressive internal organ involvement (diffuse cutaneous systemic sclerosis), and occasionally a fulminant course (fulminant systemic sclerosis).
Limited cutaneous systemic sclerosis involves areas distal to the elbows and knees but may involve the face and neck. CREST syndrome (calcinosis, Raynaud phenomenon, esophageal dysmotility, sclerodactyly, and telangiectasias—although not all are needed for the disorder to be called CREST) is an older term used to describe this subset of limited cutaneous systemic sclerosis.
Diffuse cutaneous systemic sclerosis refers to skin thickening affecting the trunk and the skin of the extremities proximal to the elbows and knees besides involvement of the face. There are rare cases of typical systemic sclerosis internal organ involvement in the absence of clinically apparent cutaneous involvement, a clinical subset known as “scleroderma sine scleroderma”.
Systemic sclerosis involvement is most obvious in the skin; however, the gastrointestinal tract as well as the respiratory, renal, cardiovascular, musculoskeletal, endocrine, and genitourinary systems are frequently involved.
In 2013, a joint committee of the American College of Rheumatology (ACR) and the European League Against Rheumatism (EULAR) published a revised classification criteria for systemic sclerosis [1, 2] to improve the sensitivity of the widely used previous classification criteria. The revised criteria for the classification of systemic sclerosis are listed in Table I, below.
Table 1. ACR/EULAR Revised Systemic Sclerosis Classification Criteria (Open Table in a new window)
Item |
Sub-item(s) |
Score* |
Skin thickening of the fingers of both hands extending proximally to the metacarpophalangeal joints (presence of this criterion is sufficient criterion for SSc classification) |
None |
9 |
Skin thickening of the fingers (count the higher score only) |
Puffy fingers |
2 |
Sclerodactyly (distal to the metacarpophalangeal joints but proximal to the proximal interphalangeal joints) |
4 |
|
Fingertip lesions (count the higher score only) |
Digital tip ulcers |
2 |
Fingertip pitting scars |
3 |
|
Telangiectasia |
None |
2 |
Abnormal nailfold capillaries |
None |
2 |
Pulmonary arterial hypertension and/or interstitial lung disease (maximum score is 2) |
Pulmonary arterial hypertension |
2 |
Interstitial lung disease |
2 |
|
Raynaud phenomenon |
None |
3 |
Systemic sclerosis–related autoantibodies (maximum score is 3) |
Anticentromere |
3 |
Anti–topoisomerase I |
3 |
|
Anti–RNA polymerase III |
3 |
|
*The total score is determined by adding the maximum score in each category. Patients with a total score ≥ 9 are classified as having definite systemic sclerosis (modified from van den Hoogen F, Khanna D, Fransen J, et al. 2013 classification criteria for systemic sclerosis: an American College of Rheumatology/European League against Rheumatism collaborative initiative. Arthritis Rheum. Nov 2013;65(11):2737-47. [1] ) |
||
Historical background
Hippocrates first described this condition as thickened skin. [3, 4] In 1836, Giovambattista Fantonetti used for the first time the term “skleroderma generale” to describe a patient with dark leather-like skin who exhibited a loss of range of joint motion caused by skin tightening. [5] Robert H. Goetz introduced the concept of scleroderma as a systemic disease in 1945 and coined the term progressive systemic sclerosis to emphasize the systemic and often progressive nature of the disease. [6]
The purpose of classification criteria is to enroll a uniform population of patients in research studies and it is based on various parameters that are commonly used for systemic sclerosis diagnosis. It is important to emphasize that these criteria are not diagnostic criteria and are not applicable to patients with scleroderma-like disorders or to patients with skin thickening sparing the fingers.
Pathophysiology
Systemic sclerosis is a systemic disease that affects numerous organ systems in addition to the skin. The pathogenesis of systemic sclerosis is complex. [7, 8, 9, 10, 11, 12, 13, 14] Increasing evidence suggests interaction between environmental and genetic factors, with a regulatory epigenetic mechanism involving changes in the expression of DNA and microRNA. [15]
The clinical and pathologic manifestations result from three distinct processes: 1) severe fibroproliferative vascular lesions of small arteries and arterioles, 2) excessive and often progressive deposition of collagen and other extracellular matrix (ECM) macromolecules in skin and various internal organs, and 3) alterations of humoral and cellular immunity. It is not clear which of those processes is of primary importance or how they are temporally related during the development and progression of the disease.
Numerous studies have suggested a sequence of pathogenetic events initiated by unknown etiologic factors in a genetically receptive host, which trigger microvascular injury characterized by structural and functional endothelial cell abnormalities. The endothelial cell abnormalities result in either increased production and release of numerous potent mediators—including cytokines, chemokines, polypeptide growth factors, and various other substances such as prostaglandins, and reactive oxygen species (ROS)—or in the reduction of important compounds such as prostacyclin and nitric oxide.
The endothelial cell dysfunction allows the chemokine- and cytokine-mediated attraction of inflammatory cells and fibroblast precursors (fibrocytes) from the bloodstream and bone marrow and their transmigration into the surrounding tissues, resulting in the establishment of a chronic inflammatory process with participation of macrophages and T and B lymphocytes, with further production and secretion of cytokines and growth factors from these cells.
The immunologic alterations include innate immunity abnormalities, tissue infiltration with macrophages and T and B lymphocytes; production of numerous disease-specific autoantibodies; and dysregulation of cytokine, chemokine, and growth factor production. The released cytokines and growth factors induce the activation and phenotypic conversion of various cellular types, including resident fibroblasts, epithelial cells, endothelial cells, and pericytes into activated myofibroblasts, the cells ultimately responsible for initiation and establishment of the fibrotic process.
This sequence of events (see diagram below) results in the development of a severe and often progressive fibroproliferative vasculopathy, and exaggerated and widespread accumulation of fibrotic tissue, the hallmark of the fibrotic process characteristic of the disease.
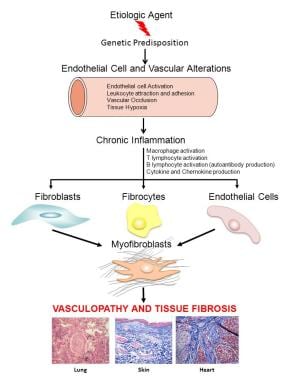 Overall scheme illustrating a proposed sequence of events involved in tissue fibrosis and fibroproliferative vasculopathy in systemic sclerosis. An unknown causative agent induces activation of immune and inflammatory cells in genetically predisposed hosts, resulting in chronic inflammation. Activated inflammatory and immune cells secrete cytokines, chemokines, and growth factors, which cause fibroblast activation, differentiation of endothelial and epithelial cells into myofibroblasts, and recruitment of fibrocytes from the bone marrow and the peripheral blood. The activated myofibroblasts produce exaggerated amounts of extracellular matrix, resulting in tissue fibrosis.
Overall scheme illustrating a proposed sequence of events involved in tissue fibrosis and fibroproliferative vasculopathy in systemic sclerosis. An unknown causative agent induces activation of immune and inflammatory cells in genetically predisposed hosts, resulting in chronic inflammation. Activated inflammatory and immune cells secrete cytokines, chemokines, and growth factors, which cause fibroblast activation, differentiation of endothelial and epithelial cells into myofibroblasts, and recruitment of fibrocytes from the bone marrow and the peripheral blood. The activated myofibroblasts produce exaggerated amounts of extracellular matrix, resulting in tissue fibrosis.
The vascular alterations preferentially affect small arteries and arterioles. Vascular dysfunction is one of the earliest alterations of systemic sclerosis. Severe alterations in small blood vessels of skin and internal organs, including endothelial dysfunction, subendothelial fibrosis, and perivascular cellular infiltration with activated T cells and macrophages, are almost universally present in systemic sclerosis–affected tissues. [9]
Endothelial dysfunction and fibrosis appear to be closely related phenomena. The vascular alterations, including the phenotypic conversion of endothelial cells into activated mesenchymal myofibroblasts, may be the initiating event and the common pathogenetic alteration leading to the fibrotic and chronic inflammatory involvement of multiple organs. [9, 10]
The activation of endothelial cells induces the expression of chemokines and cell adhesion molecules, and causes the attraction, transendothelial migration, and perivascular accumulation of immunologic-inflammatory cells, including T- and B-lymphocytes and macrophages. The inflammatory cells produce and secrete a variety of cytokines and/or growth factors, including transforming growth factor beta (TGF-β) and other profibrotic mediators such as endothelin-1. Those induce increased proliferation of smooth muscle cells, marked accumulation of subendothelial fibrotic tissue, and initiation of platelet aggregation and intravascular thrombosis, eventually causing microvascular occlusion.
The fibrotic process is characterized by the excessive production and deposition of types I, III, and VI collagens and other ECM and connective tissue macromolecules, including cartilage oligomeric matrix protein (COMP), glycosaminoglycans, tenascin, and fibronectin. [11, 12] This crucial component results from the accumulation in skin and other affected tissues of myofibroblasts, which are cells possessing unique biological functions that include increased production of fibrillar type I and type III collagens, expression of α-smooth muscle actin, and reduction in the expression of genes encoding ECM–degradative enzymes. Thus, the accumulation of myofibroblasts in affected tissues and the uncontrolled persistence of their elevated biosynthetic functions are crucial determinants of the extent and rate of progression of the fibrotic process in systemic sclerosis.
The immunologic alterations include the production of numerous autoantibodies, some with very high specificity for the disease, as well as abnormalities in the innate and acquired cellular immune responses. [13, 14] The exaggerated connective tissue production by systemic sclerosis fibroblasts is induced by cytokines and growth factors released from the tissue-infiltrating inflammatory cells.
One of the growth factors that plays a crucial role in the fibrosis that accompanies systemic sclerosis is TGF-β. One of the most important effects of TGF-β is the stimulation of ECM synthesis by stimulating the production of various collagens and other ECM proteins. [11, 12] Besides its potent ECM stimulatory effects, TGF-β also induces the generation of myofibroblasts and decreases the production of collagen-degrading metalloproteinases. TGF-β also stimulates the production of protease inhibitors, which prevent ECM breakdown.
Etiology
The exact etiology of systemic sclerosis is not known. Systemic sclerosis is not inherited, although a genetic predisposition plays an important role in its development. In individuals with a genetic predisposition, environmental factors (eg, triggers or accelerators) may contribute to the development of systemic sclerosis. [16, 17, 18, 19, 20] These factors include the following:
-
Silica exposure
-
Solvent exposure (vinyl chloride, trichloroethylene, epoxy resins, benzene, carbon tetrachloride)
-
Radiation exposure or radiotherapy
Case reports describe the development of scleroderma in patients treated with the immune checkpoint inhibitor pembrolizumab for metastatic melanoma. [21]
Cytomegalovirus, human herpesvirus 5, and parvovirus B19 have been proposed as viral accelerating factors. However, evidence of their involvement is inconclusive. [22]
Epidemiology
United States statistics
The estimated incidence of systemic sclerosis in the United States is 20 cases per million population, and its prevalence has been estimated at 276 cases per million population, although the reported prevalence varies depending on the methodology used and the targeted population. [23, 24, 25] An increased systemic sclerosis incidence and prevalence has been evident in the last 50 years. Although improved diagnosis and increased survival rate can partially account for this observation, it appears that there has been a real increase in its incidence.
International statistics
Systemic sclerosis occurs worldwide, although its reported prevalence varies significantly in different countries; for example, higher prevalence rates are reported in Europe and North and South America than in East Asia. [24, 25, 26, 27] Obtaining an exact estimate of prevalence is difficult because systemic sclerosis is frequently misdiagnosed. Furthermore, ethnic and geographical clustering may contribute to the variability in terms of frequency. However, it appears that there is higher frequency among Black individuals. [28, 29, 30, 31]
Race
Systemic sclerosis affects individuals of all races. [28, 29, 30, 31] However, incidence rates, severity and mortality may vary among ethnic groups.
Studies have documented a higher general and age-specific incidence rate in Blacks than in Whites. It has also been shown that affected African Americans develop more severe disease and have poorer outcomes when compared with other ethnic groups. [28, 29, 30, 31]
The highest prevalence of systemic sclerosis in the US is among the Oklahoma Choctaw Indians. The prevalence in the Choctaws is 469 cases per 100,000 population, which is higher than in non–full-blood Choctaw (31 per 100,000) and 20 times higher than the national average. [32] Similarly, a prevalence rate of 47 per 100,000 has been found in the indigenous peoples in Canada. [25]
Sex- and age-related disparities
The risk of systemic sclerosis is 4-9 times higher in women than in men. [23, 24, 25] However, the mechanisms responsible for the disproportionately higher frequency in females have not been elucidated.
A multicenter cohort of 2281 patients from the Italian Systemic sclerosis PRogression INvestiGation (SPRING) registry documented an overall female/male ratio of 8.2:1. Males were found to have a shorter time from onset of Raynaud phenomenon to systemic sclerosis diagnosis and an increased prevalence of the diffuse cutaneous subset, renal crisis, and digital ulcers. Women demonstrated a significantly higher percentage of sicca syndrome, serum antinuclear antibodies, antiextractable nuclear antigens, anti-La/SSB, and anticentromere protein. [33]
The peak onset occurs in individuals aged 30-50 years. Numerous cases occur in children, however, as well as in very old individuals.
Prognosis
Survival in patients with diffuse cutaneous disease has improved significantly; currently, the 5-year survival is estimated to be about 80%. Five-year survival in patients with limited cutaneous disease is approximately 90%.
Factors associated with a more severe prognosis are as follows:
-
Younger age
-
African descent
-
Rapid progression of skin symptoms
-
Greater extent of skin involvement
-
Anemia
-
Elevated erythrocyte sedimentation rate (ESR)
-
Pulmonary, renal, and cardiac involvement
Complications
Complications of systemic sclerosis include the following:
-
Digital infarctions
-
Pulmonary hypertension
-
Myositis
-
Kidney failure
Frerix and colleagues have proposed that osteonecrosis of the lunate bone (Kienböck disease), while very rare in the general population, may be a frequent manifestation of systemic sclerosis, and may be linked to vasculopathy from the disorder. [34] Lunate osteonecrosis manifests as pain and stiffness in the affected wrist and decreased grip strength in the hand.
A cross-sectional study that included 90 women with systemic sclerosis and 90 healthy controls aged 18–70 years documented a high prevalence of impaired pelvic floor function and sexual function in women with systemic sclerosis. The prevalence of female sexual dysfunction was 73% in systemic sclerosis patients versus 31% in the controls. Impaired sexual function correlated with higher disease activity, the presence of dyspnea and interstitial lung disease, increased systemic inflammation, reduced physical activity, functional disability, more severe depression, more pronounced fatigue, and impaired quality of life. [35]
Mortality/morbidity
Systemic sclerosis has the highest case-specific mortality among the systemic autoimmune diseases. Pulmonary hypertension, pulmonary fibrosis (interstitial lung disease), and scleroderma renal crisis are the most frequent causes of death. [36, 37, 38, 39, 40, 41, 42, 43]
Survival has improved in recent decades and correlates best with the clinical disease subtype (diffuse cutaneous vs limited cutaneous) and with the extent of organ involvement. Five-year survival among patients with diffuse cutaneous systemic sclerosis has improved significantly, from 69% in the 1990–1993 cohort to 84% in the 2000–2003 cohort. Five-year survival among the patients with limited cutaneous systemic sclerosis remained very high and unchanged for the same periods (93% and 91%, respectively).
For patients with scleroderma renal crisis, 1-year mortality is 20-30% and 5-year mortality is 30-50%; for normotensive scleroderma renal crisis, which accounts for about 10% of all cases, 1-year mortality is 60%. [44] Half of patients with scleroderma require hemodialysis, and kidney function recovers spontaneously in only one quarter of those. Predictors of worse outcome in patients with scleroderma renal crisis include the following [45] :
-
Older age
-
Male gender
-
Serum creatinine > 3 mg/dL at presentation
-
Incomplete blood pressure control within the first 3 days of the crisis
-
Normal blood pressure
-
Use of an angiotensin-converting enzyme (ACE) inhibitor prior to scleroderma renal crisis is also an independent predictor of poor outcome, possibly because by keeping the blood pressure under control, the medication blunts recognition of the unfolding renal crisis.
Mortality associated with scleroderma renal crisis has declined significantly in recent decades. In contrast, pulmonary involvement (interstitial lung disease and/or pulmonary arterial hypertension) has become the most common cause of death in patients with systemic sclerosis.
Patient Education
To minimize the risk of Raynaud phenomenon flare, instruct patients to maintain their core body temperature; strongly encourage smoking cessation in patients who smoke, and advise all patients to avoid exposure to cigarette smoke. Instruct the patient to avoid digital or skin trauma and prolonged cold exposure.
For patient education information, see Scleroderma.
-
Scleroderma: Tightening of the skin in the face, with a characteristic beaklike facies and paucity of wrinkles.
-
Scleroderma: Sclerodactyly with digital ulceration, loss of skin creases, joint contractures, and sparse hair.
-
Scleroderma: Anterior chest demonstrating salt-and-pepper hypopigmentation and diffuse hyperpigmentation in a white woman.
-
A radiograph of the distal digits demonstrating calcinosis and distal phalanx reabsorption (acral osteolysis).
-
Scleroderma: Fingernail capillary bed demonstrating capillary dropout with large dilated vessels.
-
Lung biopsy demonstrating severe interstitial fibrosis and medial fibrosis and smooth muscle hyperplasia of a pulmonary arteriole compatible with pulmonary hypertension.
-
Lung biopsy demonstrating expansion of the interstitium of the lung by fibrous tissue along with chronic inflammatory cells.
-
Scleroderma: Barium swallow demonstrating reflux into the distal esophagus, as well as an accordion appearance in the duodenum.
-
Skin biopsy showing extensive fibrosis. The biopsy has a square morphology, which reflects the rigidity of the tissue biopsy specimen due to striking pan-dermal sclerosis. In addition, the fibrosing reaction extends into the panniculus. The number of adnexal structures is reduced, another characteristic feature of scleroderma. A significant inflammatory cell infiltrate is not observed. This is in contradistinction to morphea, in which a prominent inflammatory cell infiltrate is present.
-
Skin biopsy showing severe fibrosis. The fibrosis reflects a widening of collagen bundles in concert with an increase in the number of collagen fibers. Note the superimposed deposition of the newly synthesized delicate collagen bundles interposed between the preexisting collagen bundles, the latter appearing wide and manifesting a hyalinized morphology.
-
Overall scheme illustrating a proposed sequence of events involved in tissue fibrosis and fibroproliferative vasculopathy in systemic sclerosis. An unknown causative agent induces activation of immune and inflammatory cells in genetically predisposed hosts, resulting in chronic inflammation. Activated inflammatory and immune cells secrete cytokines, chemokines, and growth factors, which cause fibroblast activation, differentiation of endothelial and epithelial cells into myofibroblasts, and recruitment of fibrocytes from the bone marrow and the peripheral blood. The activated myofibroblasts produce exaggerated amounts of extracellular matrix, resulting in tissue fibrosis.
Tables
Item |
Sub-item(s) |
Score* |
Skin thickening of the fingers of both hands extending proximally to the metacarpophalangeal joints (presence of this criterion is sufficient criterion for SSc classification) |
None |
9 |
Skin thickening of the fingers (count the higher score only) |
Puffy fingers |
2 |
Sclerodactyly (distal to the metacarpophalangeal joints but proximal to the proximal interphalangeal joints) |
4 |
|
Fingertip lesions (count the higher score only) |
Digital tip ulcers |
2 |
Fingertip pitting scars |
3 |
|
Telangiectasia |
None |
2 |
Abnormal nailfold capillaries |
None |
2 |
Pulmonary arterial hypertension and/or interstitial lung disease (maximum score is 2) |
Pulmonary arterial hypertension |
2 |
Interstitial lung disease |
2 |
|
Raynaud phenomenon |
None |
3 |
Systemic sclerosis–related autoantibodies (maximum score is 3) |
Anticentromere |
3 |
Anti–topoisomerase I |
3 |
|
Anti–RNA polymerase III |
3 |
|
*The total score is determined by adding the maximum score in each category. Patients with a total score ≥ 9 are classified as having definite systemic sclerosis (modified from van den Hoogen F, Khanna D, Fransen J, et al. 2013 classification criteria for systemic sclerosis: an American College of Rheumatology/European League against Rheumatism collaborative initiative. Arthritis Rheum. Nov 2013;65(11):2737-47. [1] ) |
||









