Background
Schatzki ring is a benign, thin, circular mucosal and submucosal membrane seen at the squamocolumnar junction of the distal esophagus that does not contain muscularis propria. [1]
Since the 1950s, several investigators have published reports of patients with dysphagia who had associated lower esophageal ringlike constrictions, but each investigator had a different opinion as to the cause and nature of these rings. In 1953, Ingelfinger and Kramer believed that these rings occurred as a result of a contraction by an overactive band of esophageal muscle [2] ; however, Schatzki and Gary believed that these rings were fixed and not contractile. [3] Some of this controversy may be related to the confusion of categorizing muscular and mucosal rings under the same entity, as concluded by Goyal et al. [4, 5, 6, 7]
See the image below.
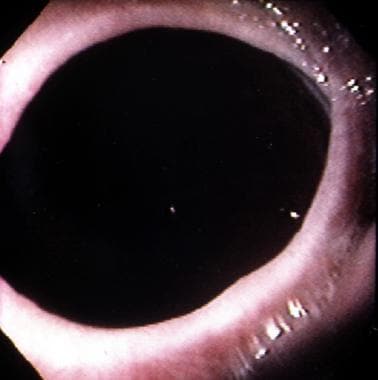 Schatzki Ring. Endoscopic appearance of the distal esophagus illustrating a Schatzki ring.
Schatzki Ring. Endoscopic appearance of the distal esophagus illustrating a Schatzki ring.
Two rings have been identified in the distal esophagus. The muscular ring, or A ring, is a thickened symmetric band of muscle that forms the upper border of the esophageal vestibule and is located approximately 2 cm above the gastroesophageal junction. The A ring is rare; furthermore, it is even more rarely associated with dysphagia. On the other hand, the mucosal ring, or B ring, is quite common and is the subject of discussion in this article. The B ring is a diaphragmlike thin mucosal ring usually located at the squamocolumnar junction; it may be symptomatic or asymptomatic, depending on the luminal diameter.
The pathogenesis is not clear, and patients typically present with intermittent nonprogressive dysphagia for solids. Fortunately, most patients respond well to initial and repeat dilatation therapy. A small number of patients may have stubborn rings that require more aggressive endoscopic or surgical intervention.
Pathophysiology
The pathogenesis of Schatzki rings is not clear, and at least 4 hypotheses have been proposed. These hypotheses may not be mutually exclusive. Proposed hypotheses are as follows:
The ring is a pleat of redundant mucosa that forms when the esophagus shortens transiently or permanently for unknown reasons.
The ring is congenital in origin.
The ring is actually a short peptic stricture occurring as a consequence of gastroesophageal reflux disease.
The ring is a consequence of pill-induced esophagitis.
Data supporting or refuting the first 2 hypotheses are few.
Data about the association of gastroesophageal reflux disease and rings are inconclusive or contradictory. It has been hypothesized that the ring acts as a protective barrier against further reflux. However, in one recent study involving 20 patients, no significant differences were noted in any of the reflux parameters measured before and after dilation. In fact, it was interesting to note that thick rings may actually decrease esophageal acid clearance, especially in the supine position, thereby increasing esophageal acid exposure.
The last hypothesis was based on a chance observation in one study showing that 62% of patients with rings had ingested medications known to cause pill-induced esophagitis.
In some studies, the severity of symptoms has clearly been demonstrated to correlate with the luminal diameter. Dysphagia predictably occurs in patients with a luminal diameter less than 13 mm and may vary between 13-20 mm, depending on the size and type of bolus.
Epidemiology
United States data
Schatzki ring is quite common and may be found in between 6% and 14% of all patients undergoing routine barium swallow studies; however, few of these patients exhibit any symptoms of dysphagia. [1] No known population studies exist for its prevalence in the general population. [1]
In restrospective review (2003-2018) of esophageal foreign body impaction (EFBI) at a single US institution, investigators analyzing data from 204 patients found structural causes were the most common etiology, with benign strictures and stenosis in 21.5% of patients, followed by Schatzki ring (7.8%) and hiatal hernia (6.9%).
International data
In a 2014 cross-sectional study (2012-2013) of data from 139 Pakistani patients presenting with dysphagia who underwent endoscopy, Schatzki ring was the fourth most common finding (n = 14 [10.1%]) after malignant esophageal stricture (n = 38 [27.3%]), normal upper gastrointestinal endoscopy (n =29 [20.9%]), and reflux esophagitis (n = 25 [18.0%]). [8]
In a 2015 retrospective report (1994-2004) of 91 geriatric (aged 62-92 years) Israeli patients presenting with dyspepsia who underwent standard radiographic studies and provocation tests for gastroesophageal reflux disease (GERD), Schatzki ring was present in 20 of the patients (22%), with all of the rings (100%) at the level of the proximal sphincter. [9]
Race-, sex-, and age-related demographics
No known race or sex predilection exists.
Although no known predilection for a specific age group exists, most patients are older than 40 years at presentation. It is relatively rare in children. [10]
In a retrospective study (2000-2009) that included 18,668 gastrointestinal or esophageal imaging studies in 15,410 children and young adults, Towbin and Diniz found 25 patients (0.2%) with a confirmed diagnosis of Schatzki ring. [10] Hiatal hernia (n = 24/25; 96%), eosinophilic esophagitis (n = 10/25; 40%), and gastroesophageal reflux (n = 10/25; 40%) were commonly associated with Schatzki rings. The investigators suggested clinicians consider endoscopy and biopsy in all children with Schatzki ring owing to the relatively high incidence of eosinophilic esophagitis in their analysis. [10]
Prognosis
Although results of dilatation are excellent for Schatzki ring, some series report that patients frequently have recurrence of dysphagia. In one study of 33 patients, 32% had recurrence at 1 year, and 89% had recurrence at 5 years. Recurrence rates up to 64% in the first 2 years have also been reported. [1]
No known prognostic indicators for recurrence of dysphagia exist, except for associated gastroesophageal reflux disease as reported in some studies. Other studies have refuted this contention.
Reassure patients that the ring is a benign entity; however, prepare them for repeat dilatation in the event of recurrence of dysphagia.
Morbidity/mortality
No mortality has been ascribed to this entity.
Morbidity is variable. Most episodes of dysphagia are short lived, and intervening periods between episodes may vary from weeks to months or even to years.
Complications
Esophageal dilatation for esophageal rings is well established as a safe procedure based on published series; however, potential complications include perforation and bleeding.
-
Schatzki Ring. Endoscopic appearance of the distal esophagus illustrating a Schatzki ring.
-
Schatzki Ring. Barium swallow illustrating an indentation at the gastroesophageal junction consistent with a Schatzki ring above a sliding hiatal hernia.
-
Schatzki Ring. A Schatzki ring dilated by the passage of a single large bougie.





