Background
Rickettsialpox is a mild, self-limited, zoonotic febrile illness characterized by eschar formation at the location of a mite bite, followed by the onset of systemic symptoms and a more generalized papulovesicular rash. The causative agent is Rickettsia akari. Previously classified as a member of the spotted-fever group of rickettsiae, it is now placed in the transitional group, since it has features of both the spotted-fever group and the typhus group. [1, 2]
Pathophysiology
R akari is an obligate intracellular gram-negative coccobacillus. Unlike other rickettsiae, which target vascular endothelial cells, R akari targets host CD68 macrophages.
Its vector is the colorless mite Liponyssoides sanguineus (formerly Allodermanyssus sanguineus), which is found on mice (most commonly the house mouse [Mus musculus]) and other rodents. These hosts serve as the reservoir for the disease. L sanguineus bite humans when murine hosts are scarce. Other vectors and reservoirs for R akari may exist considering the high seroprevalence of the pathogen among dogs in New York City and domesticated cats in California. [3]
About 7-10 days after the painless bite, a papular skin lesion appears at the bite location and becomes vesicular with a surrounding area of erythema. An eschar forms and slowly heals. About 3-7 days after the initial skin lesion develops, patients may suddenly develop high-grade fever, chills, headaches, and myalgias with subsequent development of a sparse generalized papulovesicular rash, resembling chickenpox.
 Multiple papulovesicles involving the upper trunk on a patient with rickettsialpox in North Carolina. Courtesy of the CDC.
Multiple papulovesicles involving the upper trunk on a patient with rickettsialpox in North Carolina. Courtesy of the CDC.
Rickettsialpox is mild and self-limited and usually persists for about a week.
Epidemiology
Frequency
United States
Rickettsialpox occurs primarily in urban areas, where the density of mites, mice, and humans is high. Huebner et al first isolated and named rickettsialpox in 1946 in New York City. [4]
Rickettsialpox has been reported primarily in the northeastern and midwest United States (Boston, Mass; West Hartford, Conn; Philadelphia, Pa; Pittsburgh, Pa; and Cleveland, Ohio). Cases have also been reported in North Carolina, Arkansas, and Utah. [5, 6, 7] R akari–like organisms have also been identified in wild rodents in Orange County, California. [8]
Although the prevalence of confirmed cases is very low, several reports suggest the disease is more common than previously thought. Serologic evidence of rickettsialpox exposure was found in 16% of 631 intravenous drug users in inner-city Baltimore, MD, and in 9% of 204 intravenous drug users in Harlem, NY. [9, 10] In addition, between 2001 and 2003, the number of clinical samples submitted to the Centers for Disease Control and Prevention (CDC) increased following the anthrax bioterror attack, reflecting an increased awareness of eschar-associated febrile illness. [11] Prior to this, these clinical syndromes may have been misdiagnosed, or perhaps the infected persons did not seek medical attention. Consequently, rickettsialpox is widely believed to be an underrecognized and underreported clinical entity, partially because physicians tend to be unfamiliar with this diagnosis.
In 2007, about 14 cases of rickettsialpox were reported New York City (a rate of approximately 1.7 cases per 1,000,000 persons). Case reports increased in of 2001 and continued in 2002, following the anthrax attacks in New York City, New Jersey, Washington, D.C., and Florida. [12]
International
Internationally, rickettsialpox has been described in South Africa, Costa Rica, France, Italy, Turkey, Croatia, Ukraine, Russia, and Korea. [5, 13, 14]
A case report from 2012 described the first case of rickettsialpox in the Netherlands wherein the patient did not have any contact with mice or other animals and the cause of transmission unclear. [15] There have been case reports of rickettsialpox in Mexico and suspected cases identified by serologic assays in Albania, Bosnia Herzegovina, Central African Republic, France, Germany, and Turkey. [16]
Mortality/Morbidity
Rickettsialpox is a benign, self-limited disease. No fatalities have been reported. The incubation period varies from 10-21 days. Rickettsialpox usually resolves within 14-21 days; however, headache and lassitude may persist for another 1-2 weeks.
Sex
Rickettsialpox has no sexual predilection.
Age
Rickettsialpox has no age predilection. It has been reported in patients aged 6 months to 72 years.
-
Multiple papulovesicles involving the upper trunk on a patient with rickettsialpox in North Carolina. Courtesy of the CDC.
-
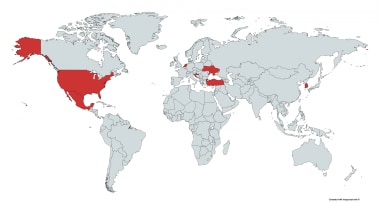
Global distribution of confirmed cases of rickettsialpox.
-
Rickettsialpox eschar on posterior right calf of patient from North Carolina. Courtesy of the CDC.
Tables
Disease |
Rash/Eschar |
Generalized Rash |
Clinical Features |
Geography |
Rickettsialpox secondary to R akari infection |
A red papule with a vesicle in the center dries and forms a black eschar with surrounding induration. Multiple eschars are possible. |
The papulovesicular rash is usually on the trunk and extremities; the palms, soles, and oral mucosa may also be involved. |
The papule precedes the febrile illness and mild systemic symptoms. Regional lymphadenopathy may develop. |
See Frequency |
Chickenpox secondary to varicella zoster infection |
The papule turns into a vesicle on an erythematous base and resembles a "dew drop on a rose petal." |
The rash begins on the head and progresses to the trunk, arms, and then legs; vesicles are present in all stages. |
It is common in children. No black eschar is present. |
Worldwide |
Mediterranean spotted fever secondary to Rickettsia conorii infection |
At the site of a tick bite, a single eschar with a red halo forms. |
The rash is generalized, involves the palms and soles, and is often maculopapular, occasionally petechial. |
Fever, headache, myalgias may develop. The onset is abrupt. The disease may be severe in context of comorbidity. |
North Africa, Middle East, Southern Europe |
African tick bite fever secondary to R africae infection |
Single or multiple eschars with regional lymphadenopathy |
A scant generalized rash, vesicular or maculopapular, may be present. Conversely, the rash may be absent. |
Fever, headache, myalgias, regional lymphadenopathy; associated with reports of subacute neuropathy |
Sub-Saharan Africa, Caribbean |
Human spotted fever secondary to R parkeri infection |
Single or multiple eschars develop from erythematous papules. |
Scant nonpruritic papules |
Fever, headache, myalgias, arthralgias |
United States |
Scrub typhus secondary to Orientia tsutsugamushi infection |
A vesicle or black scab appears on an erythematous base at the bite site. |
Vesicles are usually on the trunk or extremities. |
The rash fades within a few days; pneumonitis is common. |
Asia-Pacific rim |




