Practice Essentials
Rhinoviruses (RVs) are the most common cause of the common cold. They chiefly cause upper respiratory tract infections (URTIs) but may infect the lower respiratory tract. [1, 2] Potential complications of infection include otitis media, sinusitis, chronic bronchitis, and exacerbations of reactive airway disease (eg, asthma). Although rhinovirus infections occur year-round, the incidence is highest in the fall and the spring.
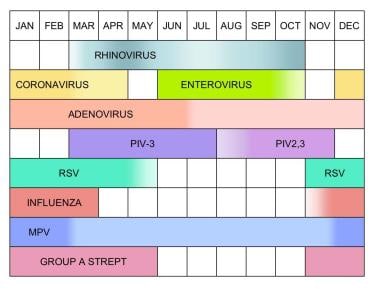 Seasonal variations in frequency of selected upper respiratory tract infection pathogens. PIV = parainfluenza virus; RSV = respiratory syncytial virus; MPV = metapneumovirus; Group A Strept = group A streptococcus.
Seasonal variations in frequency of selected upper respiratory tract infection pathogens. PIV = parainfluenza virus; RSV = respiratory syncytial virus; MPV = metapneumovirus; Group A Strept = group A streptococcus.
Signs and symptoms of rhinovirus infection
Manifestations of rhinovirus infection typically appear after an incubation period of 12-72 hours and last 7-11 days, but may persist for longer. Signs and symptoms include the following [3] :
-
Nasal dryness or irritation – May be first symptom
-
Sore throat or throat irritation – Common and bothersome initial symptom
-
Nasal discharge, nasal congestion, and sneezing – Intensify over 2-3 days
-
Headache
-
Facial and ear pressure
-
Loss of sense of smell and taste
-
Cough (30% of infected individuals)
-
Hoarseness (20%)
-
Posttussive vomiting
-
Irritability or restlessness
-
Fever (unusual; when present, typically low grade)
Age-related differences in presentation are as follows:
-
Infants and preschoolers – Fever more likely, often 38-39°C
-
Infants and toddlers – May display only nasal discharge
-
School-aged children – Usually complain of nasal congestion, cough, and runny nose
Physical examination findings include the following:
-
Typically less severe than the symptoms reported by the patients
-
Fever uncommon, though temperatures of 38-39°C are possible in younger children
-
A red nose with a profuse, dripping nasal discharge may be present
-
Nasal discharge can be clear and watery or mucopurulent (yellow or green)
-
The nasal mucous membranes have a glistening, glassy appearance, usually without obvious erythema or edema
-
The pharynx typically appears normal, without any erythema, exudate, or ulceration
-
Mildly enlarged, nontender cervical lymph nodes are present
-
Auscultation of the chest may reveal rhonchi
Complications include the following:
-
Otitis media
-
Sinusitis
-
Chronic bronchitis
-
Exacerbations of reactive airway disease
See Clinical Presentation for more detail.
Diagnosis of rhinovirus infection
If findings from a thorough history and physical examination are consistent with a viral etiology and no complications are noted, an aggressive workup rarely is necessary. Common laboratory tests (eg, WBC, CBC, ESR) have little value. Because of the prolonged time to obtain positive culture findings, rhinovirus culture rarely has been found useful in clinical settings. PCR testing of respiratory specimens may be useful in evaluating severely immunocompromised patients.
See Workup for more detail.
Management
Rhinovirus infections are predominantly mild and self-limited; thus, treatment generally is focused on symptomatic relief and prevention of person-to-person spread and complications. The mainstays of therapy are as follows:
-
Rest
-
Hydration
-
Antihistamines
-
Nasal decongestants
Other conventional supportive care for the common cold includes the following:
-
Disinfecting the environment using phenol-alcohol–based compounds
-
Washing hands
-
Positioning the mattress at a 45° angle
-
Providing comfortable surrounding temperature and adequate humidity (soothes irritated nasopharyngeal mucosae and helps eliminate nasal secretions by preventing dryness)
-
Using nasal saline drops with bulb-syringe nostril aspiration, in infants with congestion and obstruction
-
Discontinuing smoking or using alcohol
Pharmacologic treatment includes the following:
-
The combined effect of NSAIDs and antihistamines often relieves nasal obstruction.
-
Oral decongestants (pseudoephedrine) and topical decongestants (oxymetazoline and phenylephrine) commonly are used for symptomatic relief.
-
First-generation antihistamines, topical anticholinergics, and ipratropium bromide reduce rhinorrhea by 25-35%.
-
Second-generation or nonsedating antihistamines appear to have no effect on common cold symptoms.
-
Corticosteroids have no impact on cold symptoms and may increase viral replication.
-
In adults, oral zinc reduced duration of illness when high doses (at least 75 mg of elemental zinc per day) were used and when taken within 24 hours of onset of common cold symptoms. This was not seen in children. Zinc has been associated with faster resolution of nasal congestion, nasal drainage, and sore throat, as well as improvement of cough (in terms of cough score).
-
Children younger than 6 years should receive treatment with analgesics, cough suppressants, decongestants, or antihistamines only when recommended and supervised by a physician. [4]
-
The FDA recommends against the use of over-the-counter cough and cold medicines in children younger than 2 years.
See Treatment and Medication for more detail.
Background
Rhinoviruses (RVs) are members of the Picornaviridae family, which includes the human pathogens Enterovirus and Hepatovirus (notably, hepatitis A virus). More than 100 different subtypes exist in 3 major groups, categorized according to receptor specificity: intercellular adhesion molecule-1 (ICAM-1), low-density lipoprotein (LDL) receptors, and sialoprotein cell receptors.
Rhinovirus infections are chiefly limited to the upper respiratory tract but may cause otitis media and sinusitis; they also may exacerbate asthma, cystic fibrosis, chronic bronchitis, and serious lower respiratory tract illness in infants, elderly persons, and immunocompromised persons. [5, 6] Although infections occur year-round, the incidence is highest in the fall and the spring. Of persons exposed to the virus, 70-80% have symptomatic disease. Most cases are mild and self-limited.
The common cold is an acute respiratory tract infection (RTI) characterized by mild coryzal symptoms, rhinorrhea, nasal obstruction, and sneezing. Although the list of agents that cause the common cold is large, 66-75% of cases are due to 200 antigenically distinct viruses from 8 different genera. Rhinoviruses are the most common of these (25-80% of cases), followed by coronaviruses (10-20%), influenza viruses (10-15%), and adenoviruses (5%).
Although the incidence of acute RTI cannot be clearly defined because of seasonal and locational variability, it is estimated to range from 3-6 cases per person per year in the United States. Children younger than 1 year have experienced an average of 6-8 episodes of acute RTI. This figure decreases to 3-4 episodes per year by adulthood.
Pathophysiology
Viral transmission
Rhinoviruses possess various transmission modes and can infect a huge population at any given time. Most commonly, they are transmitted to susceptible individuals through direct contact or via aerosol particles. The primary site of inoculation is the nasal mucosa, though the conjunctiva may be involved to a lesser extent. The virus attaches to respiratory epithelium and spreads locally. Rhinovirus species A and B bind to the major human rhinovirus receptor, ICAM-1 (found in high quantities in the posterior nasopharynx). [7, 8, 9] Rhinovirus C (RV-C) binds to cadherin-related family member 3 receptor (CHDR-3). Viral particles usually are transmitted via inoculation into the eye or the nose from contact with the fingers that harbor the virus, especially since rhinoviruses are capable of surviving on hands for hours. [10, 11, 12]
Highly contagious behavior includes nose blowing, sneezing, and physically transferring infected secretions onto environmental surfaces or paper tissue. Contrary to popular belief, behaviors such as kissing, talking, coughing, or even drooling do not contribute substantially to the spread of disease.
Infection rates approximate 50% within the household and range from 0% to 50% within schools, indicating that transmission requires long-term contact with infected individuals. Brief exposures to others in places such as movie theaters, shopping malls, friends’ houses, or doctors’ offices are associated with a low risk for transmission. Because children produce antibodies to fewer serotypes, those who attend school are the most common reservoirs of rhinovirus infection.
Indeed, a 2022 systematic review suggested the possibility that the major route of rhinovirus in many indoor settings is through airborne transmission although different studies were in disagreement. In the natural, "real life" setting, there appeared to be "low evidence" for transmission via hands and fomites, whereas the evidence for aerosol or airborne transmission was deemed better at "moderate." [13] It was reported that during the COVID-19 pandemic, exposure to respiratory viruses (including rhinovirus) was significantly reduced due to social distancing, restriction on social gathering and increased hygiene protocols, [14, 15, 16] though there also was a differing observation that rhinovirus seemed to continue to circulate in its usual "seasonal pattern." [13]
Pathogenesis of rhinovirus infection
The attachment of the virus to its receptors (ICAM-1, CHDR-3, low-density lipoprotein receptor [LDLR]) in susceptible individuals elicits an innate immune response leading to airway inflammation and remodeling.
Few cells are actually infected by rhinovirus, and the infection involves only a small portion of the epithelium. Symptoms develop 1-2 days after viral infection, peaking 2-4 days after inoculation, though reports have described symptoms as early as 2 hours after inoculation with primary symptoms 8-16 hours later. [17] Viremia is uncommon.
A local inflammatory response to rhinovirus in the respiratory tract can lead to nasal discharge, nasal congestion, sneezing, and throat irritation. The nasal epithelium is not damaged. [18, 19] Various polymorphisms in cytokine genes have been shown to impact the severity of infection, suggesting a genetic predisposition. [20] Detectable histopathology causing the associated nasal obstruction, rhinorrhea, and sneezing is lacking, which leads to the hypothesis that the host immune response plays a major role in the pathogenesis.
Infected cells release interleukin (IL)–8, which is a potent chemoattractant for polymorphonuclear (PMN) leukocytes. Concentrations of IL-8 in secretions correlate proportionally with the severity of common cold symptoms. Inflammatory mediators, such as kinins and prostaglandins, may cause vasodilatation, increased vascular permeability, and exocrine gland secretion. These, together with local parasympathetic nerve-ending stimulation, lead to cold symptoms.
Deficient production of interferon beta by asthmatic bronchial epithelial cells has been proposed as a mechanism for increased susceptibility to rhinovirus infections in individuals with asthma.
Viral clearance is associated with the host response and is due in part to the local production of nitric oxide. Rhinovirus is shed in large amounts, with as many as 1 million infectious virions present per milliliter of nasal washings. Viral shedding can occur a few days before cold symptoms are recognized by the patient, peaks on days 2-7 of the illness, and may last as long as 3-4 weeks.
Serotype-specific neutralizing antibodies are found 7-21 days after infection in 80% of patients. Although these antibodies persist for years, providing long-lasting immunity, recovery from illness is more likely related to cell-mediated immunity. Persistent protection from repeat infection by that serotype appears to be partially attributable to immunoglobulin A (IgA) antibodies in nasal secretions, serum immunoglobulin G (IgG), and, possibly, serum immunoglobulin M (IgM).
Clinical studies indicate sinus involvement in common colds. Abnormal computed tomography (CT) findings (eg, opacification, air-fluid levels, and mucosal thickening) are present in adults with common colds that resolve over 1-2 weeks without antibiotic therapy.
Despite what is reported in folklore, no good clinical evidence suggests that colds are acquired by exposure to cold weather, getting wet, or becoming chilled.
Etiology
Rhinoviruses are small, nonenveloped, positive (sense) stranded RNA viruses of the Picornaviridae family. More than 100 different serotypes have been identified, categorized into 3 major groups on the basis of specificity for particular receptors: ICAM-1, LDL receptors, and sialoprotein cell receptors. Their structure is an icosahedral capsid of 12 pentamers containing the 4 viral proteins. A deep cleft is involved in viral attachment. Attachment to cellular receptors can be blocked by a specific antibody.
Rhinovirus grows efficiently only within a limited temperature range (33-35°C), and it cannot tolerate an acidic environment. Thus, it rarely is found outside the nasopharynx, because of the acidic environment of the stomach and the increased temperature in both the lower respiratory tract and the gastrointestinal (GI) tract.
Transmission occurs with close exposure to infected respiratory secretions, including hand-to-hand contact, self-inoculation of eyes or nose, and, possibly, large- and small-particle aerosolization. The virus has been cultured from the skin after up to 2 hours and after up to 4 days on inanimate objects in ideal conditions. Donors typically are symptomatic with a cold at the time of transmission, and virus is detected on the hands and nasal mucosa.
One study assessed the transfer of virus to surfaces by 15 adults with rhinovirus infection; each of the 15 stayed overnight in a hotel room, and afterward, 10 commonly touched sites in each room were tested for viral contamination. [21] The investigators determined that the virus could be recovered from 35% of these sites and found that the virus could be transferred back from inanimate objects to fingertips in many cases.
Higher rates of transmission occur in humid, crowded conditions such as are found in nurseries, daycare centers, and schools, especially during cooler months in temperate regions and the rainy season in tropical regions. The likelihood of transmission does not appear to be related to exposure to cold temperatures, fatigue, or sleep deprivation.
Risk factors
Factors that increase the risk and severity of rhinovirus infection include the following:
-
Smoking increases the risk for respiratory infection by approximately 50%
-
Very young or old individuals are at greater risk, possibly because of decreased immunity
-
Exposure to infected contacts increases the risk for infection
-
Touching the conjunctivae or the nose with contaminated fingers or objects increases the risk for infection
-
Crowding leads to increased transmission (eg, daycare settings) [22]
-
Men may have a slightly higher risk, but the increase probably is insignificant
-
Breastfeeding has little effect on the incidence of the common cold
-
Underlying chronic medical conditions, including anatomic, metabolic, genetic, and immunologic disorders (eg, tracheoesophageal fistula, congenital heart disease, cystic fibrosis, or immunodeficiency) increase the risk for and severity of infection
Epidemiology
United States statistics
Common colds are most frequent from September to April in temperate climates. Rhinovirus infections, which are present throughout the year, account for the initial increase in cold incidence during the fall (causing as many as 80% of colds in this period) and for a second incidence peak at the end of spring. Colds that occur from October through March are caused by the successive appearance of numerous viruses (see the image below). Adenovirus infections occur at a constant rate throughout the season.
Seasonal variations in frequency of selected upper respiratory tract infection pathogens. PIV = parainfluenza virus; RSV = respiratory syncytial virus; MPV = metapneumovirus; Group A Strept = group A streptococcus.
The incidence of the common cold is highest in preschool- and elementary school–aged children. An average of 3-8 colds per year is observed in this age group, and the incidence is even higher in children who attend daycare and preschool. Because of the numerous viral agents involved and the multiple serotypes that several of these agents (especially rhinovirus) have, it is not unusual for younger children to have new colds every month during the winter. Adults and adolescents typically have 2-4 colds per year.
International statistics
Internationally, rhinovirus is a significant cause of RTI, [23, 24, 25, 26, 27, 28, 29, 30, 31] as well as a minor cause of bronchiolitis. [32] Rhinoviruses have been found in all countries, even in remote areas such as the Kaluhi Islands and the Amazon. In Brazil, rhinoviruses reportedly cause 46% of acute RTIs. A seasonal increase in incidence during the winter months is observed worldwide.
Age-related demographics
Because antibodies to viral serotypes develop over time, the incidence of rhinovirus infection is highest in infants and young children and falls as children approach adulthood. Young children are more likely to have the frequent, close, personal contact necessary to transmit the virus; they commonly pass the infection to family members after acquiring the virus in nurseries, daycare facilities, and schools. Children also may be more contagious by virtue of having higher virus concentrations in secretions and longer duration of viral shedding.
Sex-related demographics
Some reports indicate a male predominance of infection in children younger than 3 years, which switches to a female predominance in children older than 3 years. In adults, no difference in infection rates between men and women is apparent.
Race-related demographics
No differences among different races with respect to susceptibility to rhinovirus infection or disease course have been described. In general, Native Americans and Inuit are more likely to develop the common cold and appear to have higher rates of complications such as otitis media. These findings may be explained as much by environmental conditions (eg, poverty and overcrowding) as by ethnicity.
Prognosis
The prognosis for rhinovirus infection is excellent. The most common manifestation of infection, the common cold, is mild and self-limited. Complete recovery usually is observed within 7 days for adolescents and adults and within 10-14 days for children. Occasionally, a child’s cough and congestion linger for 2-3 weeks.
Although rarely associated with fatal disease, rhinoviruses are associated with significant morbidity. Acute RTIs, predominantly rhinovirus infections, are estimated to cause 30-50% of time lost from work by adults and 60-80% of time lost from school by children. Severe respiratory disease, including bronchiolitis, asthma exacerbations, and pneumonia, [33, 34] can occur, particularly in infants and young children. [35] Preterm infants also are at high risk for severe infection. [36]
Rhinovirus is a predominant pathogen in lower respiratory tract infections (LRTI) in very low birth weight infants [30] and shares predominance in LRTI among young infants with respiratory syncytial virus (RSV). [37, 38] They also may be involved in LRTIs in elderly persons, those with cystic fibrosis, and immunosuppressed patients. The true impact of LRTI is not clear. Recovery of the virus in these patients may be a marker of an underlying disease process or a precursor to a bacterial infection.
A retrospective analysis of a prospective cohort of 728 hospitalized elderly patients with rhinovirus infection in Hong Kong revealed a significantly higher 90-day mortality rate than their counterparts (1218 patients) with influenza infection. The rhinovirus group developed pneumonia complications, required oxygen therapy, and had longer hospital stays. [39]
Patient Education
Because spread of secretions by contact with hands is a major route of transmission, encourage parents and patients to wash their hands frequently. In addition, emphasize other environmental measures to control infections, such as avoiding finger-to-eye and finger-to-nose contact and coughing and sneezing into the crook of the elbow.
Reassure families and patients that frequent colds are common at certain times of the year. Inform parents that 6-12 colds per year can be normal for young children, especially if they attend daycare or preschool. Explain that frequent self-limited colds do not indicate a problem with a child’s immune system and do not warrant antibiotic treatment and that patients with common colds need not be excluded from daycare or preschool settings.
Advise patients to return if fever exceeds 102°F, if significant respiratory distress develops, or if symptoms do not resolve in 10-14 days. Remind patients and families that purulent nasal discharge is commonly observed after the first few days of the infection and does not indicate a bacterial infection or the need for antibiotics.
Some clinicians have advocated supplementation with vitamin C. Although large doses of vitamin C have been used for prevention and treatment of colds, controlled trials reveal minimal therapeutic benefit and no preventive qualities. [40] In any case, high doses in children are not recommended.
-
Seasonal variations in frequency of selected upper respiratory tract infection pathogens. PIV = parainfluenza virus; RSV = respiratory syncytial virus; MPV = metapneumovirus; Group A Strept = group A streptococcus.






