Background
Balantidiasis (also known as balantidiosis) is defined as large-intestinal infection with Balantidium coli, which is a ciliated protozoan (and the largest protozoan that infects humans). B coli is known to parasitize the colon, and pigs may be its primary reservoir.
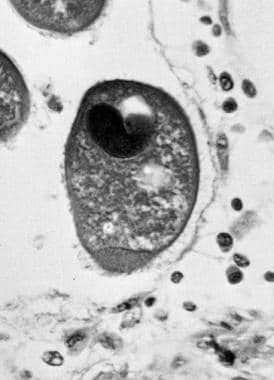 Trophozoite of Balantidium coli in colon. This photograph shows the large macronucleus and the thin cell membrane covered with cilia (X820). Courtesy of Armed Forces Institute of Pathology (AFIP 75-9300).
Trophozoite of Balantidium coli in colon. This photograph shows the large macronucleus and the thin cell membrane covered with cilia (X820). Courtesy of Armed Forces Institute of Pathology (AFIP 75-9300).
See Common Intestinal Parasites, a Critical Images slideshow, to help make an accurate diagnosis.
Balantidiasis is a zoonotic disease transmitted from pigs to humans and nonhuman primates via the fecal-oral route. Humans acquire this infection through water and food contaminated with pig or human feces. [1] Human-to-human transmission also is possible. Infected pigs remain asymptomatic, whereas humans can either remain asymptomatic or develop dysentery.
B coli was first described by Malmsten in 1857 in two patients presenting with symptoms of dysentery. It initially was named under the genus Paramoecium. It then was simultaneously reported by Leuckart and Stein in 1861 and 1862, respectively, and they renamed the genus Balantidium. It is more common in warmer regions than in cooler ones. [2]
Pathophysiology
B coli exists as a trophozoite and a cyst and usually affects the large intestine, from the caecum to the rectum. The trophozoites replicate by binary fission and conjugation, and they subsist on bacteria. Humans ingest infective cysts, which then migrate to the large intestine, cecum, and terminal ileum. The organisms primarily dwell in the lumen but can also penetrate the mucosa and cause ulcers. [3]
The invasion of the intestinal mucosa is facilitated by the following:
-
Mechanical action of ciliary movements of trophozoites
-
Production of hyaluronidase, which digests the hyaluronic acid necessary for keeping the mucosal epithelial cells together
-
Production of proteolytic enzymes by the parasite
The proteolytic activity of this parasite may also cause the tissue invasion and intestinal perforation. [4, 5]
Balantidium ulcers
Intestinal ulcers similar to those caused by intestinal amoebiasis are found in cecum, ascending colon, sigmoid colon, and rectum. However, in contrast to amebic ulcers, Balantidium ulcers do not invade muscular layers of intestine. The trophozoites can be demonstrated in the edges of the ulcer and in the pus. [2]
Epidemiology
Frequency
United States
Balantidiasis is found worldwide and has an overall estimated prevalence of 1%. Balantidiasis epidemics have occurred in psychiatric hospitals in the United States.
India
Cases of B coli infection from cattle, pigs, [6] and rats, among others, have been previously reported from India. Very few cases of human Bcoli infection have been reported in India. Kumar et al reported a case of B coli infection in a 37-year-old man with tuberculosis; he presented with fever, anorexia, mild abdominal pain, and episodes of loose stools for 1 week. [7]
In 2014 in India, urinary balantidiasis was reported in an elderly farmer with diabetes and chronic kidney disease. [8]
Umesh demonstrated a case of urinary balantidiasis in a 29-year-old woman in Mumbai, India, but this report failed to demonstrate B coli on stool examination, required to confirm the hypothesis of extraintestinal Bcoli infection in humans. [9]
In a 2002 study by Kaur et al, diarrhea in children in New Delhi were determined to be parasitic based on direct wet mount examination. [10] In 2016, Kapur et al described a case of liver abscess with B coli trophozoites on wet mount of pus aspirate. [11]
International
Balantidiasis tends to be more common among persons who handle pigs. The disease most commonly is reported in Latin America; Southeast Asia; and Papua, New Guinea. In 1971, a balantidiasis outbreak involving 100 people occurred in Truk following a typhoon. [12] In France, a pork butcher with immunosuppression due to alcohol use developed occupational balantidiasis. [13]
Urinary balantidiasis has been reported from Thailand. [14]
Mortality/Morbidity
Most cases of balantidiasis in immunocompetent individuals are asymptomatic. Mortality rates associated with acute and fulminating types of balantidiasis were as high as 30% in untreated patients prior to the introduction of antibiotics. Pneumonia has been described in patients with cancer-related immunosuppression [15] and has not always been associated with direct contact with pigs.
Prognosis
In the antibiotic era, severe balantidiasis carries an improved prognosis, and most affected patients now recover.
Patient Education
Patients should be counseled on the importance of good handwashing, particularly after being exposed to environments where likelihood of infection is high.
-
Trophozoite of Balantidium coli in colon. This photograph shows the large macronucleus and the thin cell membrane covered with cilia (X820). Courtesy of Armed Forces Institute of Pathology (AFIP 75-9300).
-
Cyst of Balantidium coli in feces. This photograph demonstrates a thick cyst wall and a large macronucleus (X820). Courtesy Armed Forces Institute of Pathology (AFIP 75-9301).






