Practice Essentials
An arteriovenous malformation (AVM) is a defect in the vascular system in which a tangle of abnormal blood vessels directly connects the feeding arteries to a venous drainage network without the interposition of a capillary bed. [1]
Vascular anomalies are among the most common congenital abnormalities in infants and children. Historically, their treatment has been impeded by confusing terminology and imprecise classification. Lesions were named with descriptive terms (eg, strawberry hemangioma or port-wine stain) or histopathologic terms (eg, capillary hemangioma, cavernous hemangioma, or lymphangioma). Although some vascular anomalies may appear similar, their biologic behavior differs markedly; therefore, treatment should be based on a proper classification system. [2, 3]
Classification
Classification of vascular anomalies is based on the landmark 1982 paper by Mulliken and Glowacki, which proposed a simplified categorization of these anomalies that was based on biologic activity. [4] As a result, the following two main types of vascular anomalies are generally recognized:
-
Vascular tumors
Differentiating between these two types of anomalies is essential because their treatment is quite different. The management of vascular anomalies is a dynamic and rapidly developing subspecialty, which requires interdisciplinary care and collaboration.
During its 1996 workshop, the International Society for the Study of Vascular Anomalies (ISSVA) adopted a classification system designed to provide a common language for guiding treatment. It was based on Mulliken and Glowacki’s biologic study but also further distinguished vascular malformations according to hemodynamics and predominant anomalous channels. [5, 6, 7, 8] At its 20th workshop in 2014, the ISSVA approved a revised classification, [9] which was further revised at the ISSVA General Assembly in May 2018 (see Table 1 below). [10]
Table 1. ISSVA Classification of Vascular Anomalies (May 2018 Revision) (Open Table in a new window)
| Vascular Tumors | Vascular Malformations |
|---|---|
Benign vascular tumors Infantile hemangioma/hemangioma of infancy Congenital hemangioma
Tufted angioma Spindle-cell angioma Epithelioid angioma Pyogenic granuloma (lobular capillary hemangioma) Others Related lesions |
Simple vascular malformations Capillary malformation (CM)
Lymphatic malformation (LM)
Venous malformation (VM)
Arteriovenous malformation (AVM)
Arteriovenous fistula (AVF) (congenital)
|
Locally aggressive or borderline vascular tumors Kaposiform hemangioendothelioma Retiform hemangioendothelioma Papillary intralymphatic angioendothelioma (PILA), Dabska tumor Composite hemangioendothelioma Pseudomyogenic hemangioendothelioma Polymorphous hemangioendothelioma Hemangioendothelioma not otherwise specified Kaposi sarcoma Others |
Combined vascular malformations CM + VM = CVM CM + LM = CLM CM + AVM = CAVM LM + VM = LVM CM + LM + VM = CLVM CM + LM + AVM = CLAVM CM + VM + AVM = CVAVM CM + LM + VM + AVM = CLVAVM |
Malignant vascular tumors Angiosarcoma Epithelioid hemangioendothelioma Others |
Anomalies of major named vessels (channel-type or truncal vascular malformations) Affecting
Anomalies of
|
Vascular malformations associated with other anomalies Klippel-Trenaunay syndrome Parkes Weber syndrome Servelle-Martorell syndrome Sturge-Weber syndrome Limb CM + congenital nonprogressive limb overgrowth Maffucci syndrome Macrocephaly-CM Microcephaly-CM CLOVES syndrome Proteus syndrome Bannayan-Riley-Ruvalcaba syndrome CLAPO syndrome |
|
| C = capillary, V = venous, L = lymphatic, A = arterial, M = malformation, F = fistula. |
A few vascular anomalies remained provisionally unclassified. [10] Additional information is available on the ISSVA Web site.
Pathophysiology
The pathogenesis of AVMs is not well understood [11, 1] but is thought to involve abnormal vasculogenesis. Multiple biologic studies since 1982 have demonstrated clear differences between vascular tumors (hemangiomas) and vascular malformations. Some have hypothesized that infantile hemangiomas result from excess angiogenesis, whereas vascular malformations are due to errors in vessel remodeling. [12] Although some vascular malformations thicken, expand, or multiply with time, it is unclear whether true angiogenesis occurs.
Marler et al suggested that vascular malformations may be angiogenesis-dependent disorders. They found that urinary high-molecular-weight matrix metalloproteinases (hMW MMPs) and basic fibroblast growth factor (bFGF) levels are elevated in vascular tumors and some vascular malformations (eg, lymphatic malformations [LMs], lymphaticovenous malformations [LVMs], and AVMs) and that the urinary increase in these proteins parallels the tissue remodeling seen in diffuse and expanding vascular malformations. [13] They suggested that drugs targeting bFGF or MMPs may be an adequate therapeutic strategy for patients suffering from these vascular anomalies.
Inherited forms of vascular malformations are rare [6] but may offer insight into the molecular mechanisms and signaling pathways involved in the pathogenesis of these lesions. This may in turn identify potential novel therapeutic targets, though at present, it is unclear whether the more common sporadic vascular malformations share similar biologic mechanisms with the infrequent inherited vascular malformations.
An AVM is a hemodynamically active fast-flow vascular malformation. [14] Arterial feeders and enlarged draining veins directly connect through micro- and macroarteriovenous fistulas that create the nidus or epicenter of the AVM. AVMs may occur both superficially and viscerally. They are usually present at birth and rarely regress. [6] They have a normal endothelial cell cycle and grow commensurately with the child. [4, 2]
The natural history of AVMs may be organized according to the clinical staging system proposed by Schobinger at the 1990 ISSVA meeting in Amsterdam (see Table 2 below). [15]
Table 2. Schobinger Staging for AVMs (Open Table in a new window)
Stage |
Description |
I - Quiescence |
Pink-bluish stain, warmth, and arteriovenous shunting are revealed by Doppler scanning. The arteriovenous malformation mimics a capillary malformation or involuting hemangioma. |
II - Expansion |
The description is the same as stage I, plus enlargement, pulsations, thrill, and bruit and tortuous/tense veins. |
III - Destruction |
The description is the same as stage II, plus dystrophic skin changes, ulceration, bleeding, persistent pain, or tissue necrosis. Bony lytic lesions may occur. |
IV - Decompensation |
The description is the same as stage III, plus congestive cardiac failure with increased cardiac output and left ventricle hypertrophy. |
Some authors, citing case reports describing "de novo" brain AVMs, have suggested that some of these AVMS may develop some time after birth as a result some kind of "second hit" (eg, from a previous intracranial hemorrhage or vascular pathology). [16]
Epidemiology
Although vascular anomalies are among the most common pediatric abnormalities, occurring in approximately 1% of children, [17] AVMs are rare. [6]
Most AVMs are evident at birth (40% in a study of 200 AVMs by Enjolras et al), [18] though they may not be clinically relevant. Mulliken and Glowacki noted that 90% of vascular malformations were present at birth in a series of 23 patients; however, these lesions were predominantly venous in type and may not be representative of AVMs per se. [4]
The female-to-male ratio for vascular malformations is 1:1. [4, 18]
Prognosis
AVMs never regress and usually follow the stages outlined by Schobinger (see Pathophysiology). Morbidity and mortality are dependent on several factors, as follows:
-
Location and size of the AVM
-
Whether the AVM is surgically accessible or amenable to palliative embolization/sclerotherapy
-
Presence or absence of congestive heart failure
The prognosis is excellent when AVMs are managed by an interdisciplinary team, and the best success is achieved in surgically accessible lesions treated with combined embolization and complete surgical resection. (See the image below.)
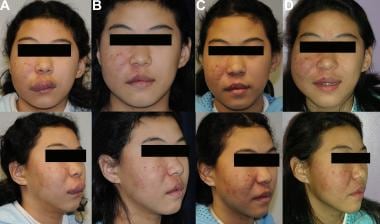 Panel A: 12-year-old female with right facial arteriovenous malformation (AVM) s/p sclerotherapy. Panel B: 12.5-year-old female 4 months after resection of right facial AVM with preoperative embolization, complex closure, and lip reconstruction with rotational advancement flaps. Panel C: 13-year-old female with good recovery and no residual palpable or pulsatile AVM. Panel D: 14-year-old female with regrowth of AVM after the onset of puberty.
Panel A: 12-year-old female with right facial arteriovenous malformation (AVM) s/p sclerotherapy. Panel B: 12.5-year-old female 4 months after resection of right facial AVM with preoperative embolization, complex closure, and lip reconstruction with rotational advancement flaps. Panel C: 13-year-old female with good recovery and no residual palpable or pulsatile AVM. Panel D: 14-year-old female with regrowth of AVM after the onset of puberty.
-
Panel A: 12-year-old female with right facial arteriovenous malformation (AVM) s/p sclerotherapy. Panel B: 12.5-year-old female 4 months after resection of right facial AVM with preoperative embolization, complex closure, and lip reconstruction with rotational advancement flaps. Panel C: 13-year-old female with good recovery and no residual palpable or pulsatile AVM. Panel D: 14-year-old female with regrowth of AVM after the onset of puberty.
-
MRI of a rectal arteriovenous malformation (AVM). Panel A: Axial, intraperitoneal rectum. Panel B: Axial, extraperitoneal rectum. Panel C: Coronal, posterior to lumbosacral prominence.
-
Angiogram of a rectal arteriovenous malformation (AVM). Panel A: arterial phase. Panel B: venous phase.
-
Ischemic contractures secondary to a right hand arteriovenous malformation (AVM). Panel A: ventral. Panel B: dorsal. Panel C: excellent outcome after surgical resection/amputation.
-
Left thigh arteriovenous malformation (AVM). Panel A: intraoperative. Panel B: bisected.
-
CT Angiogram of a pulmonary arteriovenous malformation (AVM).
Tables
| Vascular Tumors | Vascular Malformations |
|---|---|
Benign vascular tumors Infantile hemangioma/hemangioma of infancy Congenital hemangioma
Tufted angioma Spindle-cell angioma Epithelioid angioma Pyogenic granuloma (lobular capillary hemangioma) Others Related lesions |
Simple vascular malformations Capillary malformation (CM)
Lymphatic malformation (LM)
Venous malformation (VM)
Arteriovenous malformation (AVM)
Arteriovenous fistula (AVF) (congenital)
|
Locally aggressive or borderline vascular tumors Kaposiform hemangioendothelioma Retiform hemangioendothelioma Papillary intralymphatic angioendothelioma (PILA), Dabska tumor Composite hemangioendothelioma Pseudomyogenic hemangioendothelioma Polymorphous hemangioendothelioma Hemangioendothelioma not otherwise specified Kaposi sarcoma Others |
Combined vascular malformations CM + VM = CVM CM + LM = CLM CM + AVM = CAVM LM + VM = LVM CM + LM + VM = CLVM CM + LM + AVM = CLAVM CM + VM + AVM = CVAVM CM + LM + VM + AVM = CLVAVM |
Malignant vascular tumors Angiosarcoma Epithelioid hemangioendothelioma Others |
Anomalies of major named vessels (channel-type or truncal vascular malformations) Affecting
Anomalies of
|
Vascular malformations associated with other anomalies Klippel-Trenaunay syndrome Parkes Weber syndrome Servelle-Martorell syndrome Sturge-Weber syndrome Limb CM + congenital nonprogressive limb overgrowth Maffucci syndrome Macrocephaly-CM Microcephaly-CM CLOVES syndrome Proteus syndrome Bannayan-Riley-Ruvalcaba syndrome CLAPO syndrome |
|
| C = capillary, V = venous, L = lymphatic, A = arterial, M = malformation, F = fistula. |
Stage |
Description |
I - Quiescence |
Pink-bluish stain, warmth, and arteriovenous shunting are revealed by Doppler scanning. The arteriovenous malformation mimics a capillary malformation or involuting hemangioma. |
II - Expansion |
The description is the same as stage I, plus enlargement, pulsations, thrill, and bruit and tortuous/tense veins. |
III - Destruction |
The description is the same as stage II, plus dystrophic skin changes, ulceration, bleeding, persistent pain, or tissue necrosis. Bony lytic lesions may occur. |
IV - Decompensation |
The description is the same as stage III, plus congestive cardiac failure with increased cardiac output and left ventricle hypertrophy. |
Absolute Indications |
Relative Indications |
Hemorrhage Ischemia (arterial insufficiency or ulceration, gangrene) Chronic venous insufficiency with venous hypertension Lesions that compromise breathing, vision, hearing, or eating High-output cardiac failure |
Poor quality of life (disabling or intractable pain, functional impairment, severe cosmetic deformity) Lesions with potentially high risk of complications (eg, hemarthrosis, fracture, or limb-threatening location) Vascular-bone syndrome with limb length discrepancy |
Table modified from Lee et al. [29] |
|








