Background
Onchocerciasis is an infection caused by the nematode Onchocerca volvulus. Humans acquire onchocerciasis through the bite of Simulium blackflies. [1, 2, 3, 4] Because the fly develops and breeds in flowing water, onchocerciasis is commonly found along rivers and is sometimes referred to as river blindness.
In the human host, the adult nematodes live in subcutaneous nodules and produce microfilariae, which are found throughout the body but preferentially reside in the skin and eye. Repeated exposures to infected flies increase the number of adult worms and microfilariae in the host. Chronic cutaneous onchocerciasis (onchodermatitis) causes pruritus, a papular rash, scarring, and lichenification. Over time, affected skin may begin to sag, leading to terms such as "hanging groin." Patchy depigmentation on the legs leads to a condition known as leopard skin. The term sowda is used to describe severe pruritus with darkening of the skin, often confined to one limb. Chronic ocular onchocerciasis may lead to sclerosing keratitis and iridocyclitis, and finally to blindness. [1]
Onchocerciasis is endemic in Africa, Yemen, and in small foci in Central America and South America. The burden of the disease has been reduced by prevention efforts, including control of the fly vector and periodic ivermectin therapy in at-risk individuals. More recently, attention has been focused on Wolbachia organisms, which are endosymbiotic bacteria carried by adult worms and microfilariae. Treatment of Wolbachia infection has been shown to disrupt microfilariae production by the adult female nematode. Despite these efforts, onchocerciasis remains the second leading infectious cause of blindness worldwide. [5]
Pathophysiology
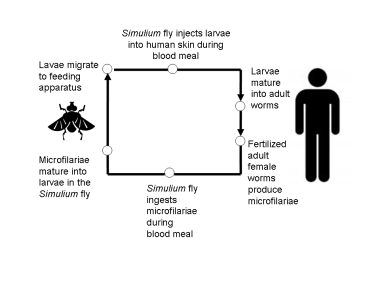
O volvulus microfilariae mature into larvae in the gut of blackflies of the genus Simulium. These larvae migrate to the proboscis of the fly and are introduced to the human bloodstream when flies take blood meals. In humans, larvae migrate to various parts of the body, but most often the skin and eye, and form nodules referred to as onchocercoma, typically seen in the skin, around joints and other bony prominences. [6]

O volvulus larvae mature into their sexually competent adult forms in these nodules. Male worms may move between nodules to fertilize female worms. Fertilized female worms then produce microfilariae, which are released into the bloodstream, and picked up when new Simulium blackflies feed from infected humans. Adults may inhabit nodules for as many as 10-15 years, and female adults may produce microfilariae for their entire lifespans. Microfilariae have lifespans of around 12-15 months. [7] The production of microfilariae by female adult worms depends on their associated Wolbachia endosymbiont. Drugs that target Wolbachia have been shown to adversely affect microfilariae production. [8, 9]
Epidemiology
Frequency
United States
Onchocerciasis is not acquired in the United States. Occasional cases are found in immigrants or travelers from endemic areas. [10, 11] However, symptomatic onchocerciasis usually requires heavy infestations and repeated exposure to the vector fly. Short-term travelers are at little or no risk for the disease. Pruritus, dermatitis, and eosinophilia may occur in travelers who stay longer than 3 months in endemic areas of Africa. Symptoms may occur months to years after leaving the endemic area.
International
Currently, onchocerciasis is endemic to 31 African countries, to Yemen, and in localized foci in Brazil and Venezuela. [12, 13] Globally, at least 18 million individuals have onchocerciasis, 99% of whom reside in Africa. [14, 15] Recent estimates suggest that over 220 million people live in areas with onchocerciasis transmission, and as many as 1.15 million people are blind or have reduced vision as a result of the disease. [16, 17]
Since 1975, the WHO, international foundations, nongovernmental organizations, and governments have worked cooperatively to reduce the burden of onchocerciasis. [18, 19, 20, 21, 22, 23, 24, 25, 26] Initial efforts focused on insecticide sprays and habitat control to reduce the numbers of black fly vectors. With the introduction of effective treatment, the program became focused on periodic treatment of at-risk persons.
Since 1987, ivermectin has been provided free of charge by Merck through the Mectizan Donation Program. By 2002, most affected countries had introduced population-based programs to supply ivermectin at least annually to at-risk individuals. The drug temporarily reduces the microfilarial burden, resulting in reduced morbidity and a reduced number of flies becoming infected when they bite humans. Reports suggest that this has been highly effective in the Americas, where transmission has been interrupted entirely in several areas, and ocular disease has been eliminated in most foci. In Africa, morbidity and transmission have been reduced but not eliminated. This may be due, at least in part, to migration of infected people into new areas, as well as the challenges inherent in educating and motivating large numbers of people. [27] Whether efforts to stem the transmission of Onchocerciasis might benefit from increased frequency of ivermectin administration is a matter of current debate, as increased medication administration has been associated with greater decreases in circulating O volvulus microfilariae, which might accelerate elimination efforts and limit the risk of drug resistance. [28, 29]
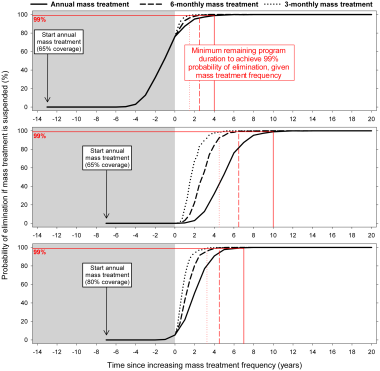 This graph shows predicted trends in onchocerciasis elimination under different MDA scenarios, showing projections for yearly, biannual, and quarterly MDA, 65% and 80% MDA coverage, and differing rounds of past MDA (8 vs 14). Courtesy of PLOS [Coffeng LE, Stolk WA, Hoerauf A, Habbema D, Bakker R, Hopkins AD, et al. Elimination of African Onchocerciasis: Modeling the Impact of Increasing the Frequency of Ivermectin Mass Treatment. PLoS One. 2014 Dec 29;9(12):e115886. Online at: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0115886.].
This graph shows predicted trends in onchocerciasis elimination under different MDA scenarios, showing projections for yearly, biannual, and quarterly MDA, 65% and 80% MDA coverage, and differing rounds of past MDA (8 vs 14). Courtesy of PLOS [Coffeng LE, Stolk WA, Hoerauf A, Habbema D, Bakker R, Hopkins AD, et al. Elimination of African Onchocerciasis: Modeling the Impact of Increasing the Frequency of Ivermectin Mass Treatment. PLoS One. 2014 Dec 29;9(12):e115886. Online at: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0115886.].
Despite the challenges they face, control programs have had a significant impact. In Africa alone, an estimated 600,000 cases of blindness had been prevented by 2002 and 18 million children were living in risk-free areas. In 2007, 69 million doses of ivermectin were supplied through the Mectizan Donation Program to reduce the burden of onchocerciasis. In South America, transmission has been interrupted or eliminated in 11 of 13 original foci of infection, limiting the range of the disease from 6 to 2 countries on that continent. [12, 13, 30]
Mortality/Morbidity
Onchocerciasis is the second-leading infectious cause of blindness in the world. [5]
Skin disease and subcutaneous nodules can be intensely pruritic. [31]
Long-term onchodermatitis may cause scarring, depigmentation, loss of skin elasticity, and disfigurement.
Although not directly fatal, blindness and skin disease caused by onchocerciasis affect the hosts’ ability to assimilate into their societies, perform daily tasks, and care for themselves. [32]
Affected persons often have a low body mass.
Blindness alone has been estimated to reduce life expectancy by 4-10 years.
In some parts of the West African savanna, up to 10% of villagers may be blind from the disease.
Onchocerciasis may also be associated with neurologic disease, with reports of epilepsy (nodding syndrome, onchocerciasis-associated epilepsy) and developmental disability (Nakalanga syndrome) among children in specific foci of onchocerciasis transmission in Africa and in the Americas. Some have argued that all of these presentations may be different manifestations of onchocerciasis-associated epilepsy. [33]
Race
Onchocerciasis does not have a racial predilection. For an unclear reason, the symptoms caused by O volvulus infection appear to differ from region to region. For example, onchodermatitis is more common in forested areas, while blindness is more common in savanna areas. Some evidence has suggested that genetic variation in the host may explain part of this geographic specificity. [34]
Sex
Onchocerciasis does not have a sexual predilection.
Age
Onchocerciasis does not have an age predilection. Children born to mothers with onchocerciasis may be immunotolerant to O volvulus infection, potentially leading to a higher microfilarial burden. Transplacental transmission of microfilariae may occur.
-
Simulium fly (black fly).
-
Histopathology of an Onchocerca volvulus nodule. Courtesy of the CDC and Dr. Mae Melvin.
-
Simplified life cycle of Onchocerciasis volvulus.
-
Subcutaneous nodule on hip caused by encysted Onchocerca volvulus.
-
Man blinded by microfilariae of Onchocerca volvulus.
-
Bleeding on skin due to scratching of itchy skin (onchodermatitis).
-
One anatomic quarter of body (leg) markedly affected by edema and papule formation of onchodermatitis.
-
Skin of a West African person with leopard spot depigmentation.
-
Patient from Cameroon with sowdalike lesions.
-
Microfilaria of Onchocera volvulus stained from skin biopsy. Courtesy of Cali Colombia, D Scott Smith, MD, and Gloria Palma, MD, PhD.
-
Taking a skin snip from the hip with a 5-microgram iris scissors for quantitatively diagnosing Onchocerca volvulus infection (Rio de Micay, Colombia). Courtesy of D Scott Smith, MD.
-
Taking a skin snip from the hip with a 5-microgram iris scissors for quantitatively diagnosing Onchocerca volvulus infection (Rio de Micay, Colombia). Courtesy of D Scott Smith, MD.
-
Adults blinded by onchocerciasis. This is the WHO/New York Times photo that inspired World Bank funding for River Blindness control programs and then the bronze statue in front of the WHO in Geneva Switzerland. Courtesy of Otis Historical Archives, National Museum of Health and Medicine.
-
This graph shows predicted trends in onchocerciasis elimination under different MDA scenarios, showing projections for yearly, biannual, and quarterly MDA, 65% and 80% MDA coverage, and differing rounds of past MDA (8 vs 14). Courtesy of PLOS [Coffeng LE, Stolk WA, Hoerauf A, Habbema D, Bakker R, Hopkins AD, et al. Elimination of African Onchocerciasis: Modeling the Impact of Increasing the Frequency of Ivermectin Mass Treatment. PLoS One. 2014 Dec 29;9(12):e115886. Online at: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0115886.].





