Practice Essentials
The term tubulointerstitial is used to broadly refer to kidney diseases that involve structures in the kidney outside the glomerulus. [1] These diseases generally involve tubules and/or the interstitium of the kidney and spare the glomeruli, as shown in the image below.
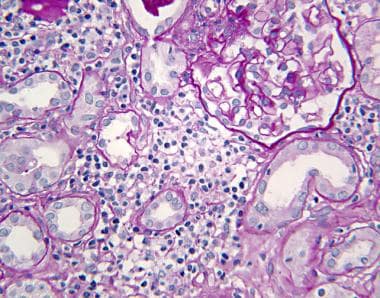 Tubulointerstitial nephritis: Kidney biopsy reveals acute interstitial nephritis. The renal cortex shows a diffuse interstitial, predominantly mononuclear, inflammatory infiltrate with no changes to the glomerulus. Tubules in the center of the field are separated by inflammation and edema, as compared with the more normal architecture in the right lower area (periodic acid–Schiff, 40 X).
Tubulointerstitial nephritis: Kidney biopsy reveals acute interstitial nephritis. The renal cortex shows a diffuse interstitial, predominantly mononuclear, inflammatory infiltrate with no changes to the glomerulus. Tubules in the center of the field are separated by inflammation and edema, as compared with the more normal architecture in the right lower area (periodic acid–Schiff, 40 X).
Although primary glomerular diseases are often associated with prominent tubulointerstitial changes (see the following image), the clinical presentation is dominated by the consequences of glomerular injury; hence, they are not considered in this article.
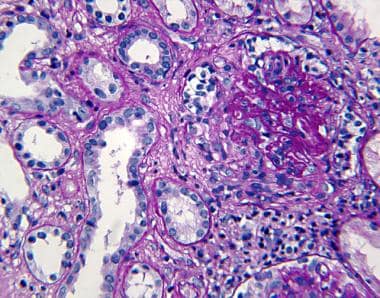 Tubulointerstitial nephritis. Kidney biopsy shows acute crescentic glomerulonephritis. The glomerular tuft is compressed by the proliferation of epithelial cells, forming a crescent. In addition, the interstitium shows mononuclear inflammatory infiltrate and edema (periodic acid–Schiff, 40 X).
Tubulointerstitial nephritis. Kidney biopsy shows acute crescentic glomerulonephritis. The glomerular tuft is compressed by the proliferation of epithelial cells, forming a crescent. In addition, the interstitium shows mononuclear inflammatory infiltrate and edema (periodic acid–Schiff, 40 X).
Many cases of tubulointerstitialnephritis result from exposure to drugs or other nephrotoxic agents such as heavy metals and, rarely, infection. By far the most common form of tubulointerstitial inflammation is a hypersensitivity reaction to medications, termed allergic interstitial nephritis. See Etiology
Presentation and workup
In acute tubulointerstitial nephritis, the presentation may vary depending on the cause. Rash, fever, eosinophilia, eosinophiluria, and elevated IgE levels are common. Patients with allergic interstitial nephritis caused by NSAIDs may present with nephrotic syndrome, with massive proteinuria, hypoalbuminemia, and edema in addition to the typical features of acute interstitial nephritis.
In chronic tubulointerstitial nephritis, patients are usually asymptomatic. The condition is often discovered incidentally on routine laboratory screening or evaluation of hypertension.
Although the clinical presentation is often sufficient to make the diagnosis, kidney biopsy is required for a definitive diagnosis of tubulointerstitial nephritis. Additional testing may be indicated for confirmation of etiology (eg, ultrasonography to identify hydronephrosis in obstructive disease, EDTA lead mobilization in suspected lead nephropathy).
Treatment
In cases of allergic interstitial nephritis, early recognition and prompt discontinuation of the offending drug usually, but not always, results in complete recovery. If no sign of improvement is observed within a few days, corticosteroid therapy may be considered.
Tubulointerstitial disease may progress to end-stage renal disease and thus require dialysis or transplantation.
See also Glomerulonephritis, Membranoproliferative Glomerulonephritis, Pediatric Nephritis, and Radiation Nephritis.
Pathophysiology
Tubulointerstitial nephritis involves the immune-mediated infiltration of the kidney interstitium by inflammatory cells. [2] Lethal or sublethal injury to kidney cells leads to expression of new local antigens, inflammatory cell infiltration, and activation of proinflammatory and chemoattractant cytokines. These cytokines are produced by inflammatory cells (ie, macrophages, lymphocytes) and also by the kidney cells (ie, proximal tubule, vascular endothelial cells, interstitial cells, fibroblasts). The outcome can be acute or chronic nephritis.
In acute interstitial nephritis, the tubular damage leads to renal tubular dysfunction, with or without acute kidney injury. Regardless of the severity of the damage to the tubular epithelium, the kidney dysfunction is generally reversible, possibly reflecting the regenerative capacity of tubules with preserved basement membrane. Conversely, chronic tubulointerstitial nephritis is characterized by interstitial scarring, fibrosis, and tubule atrophy, resulting in progressive chronic kidney insufficiency. [3, 4]
The principal mechanism in acute tubulointerstitial nephritis is a hypersensitivity reaction to drugs such as penicillins, nonsteroidal anti-inflammatory drugs (NSAIDs), and sulfa drugs. Another mechanism is acute cellular injury caused by infection, viral or bacterial, often associated with obstruction or reflux. The kidney is remarkably resistant to structural damage in bacterial infections, and, in the absence of obstruction, damage from bacterial infection in the kidney parenchyma is extremely unlikely to occur.
Serum components — in particular, matrix metalloproteinases MMP1 and MMP7 — can directly injure the downstream tubular portions of the kidney. This can lead to secretion of inflammatory cytokines and extracellular remodeling, which may promote kidney fibrosis. [5]
Studies have revealed transforming growth factor–beta (TGF-β) as a major participant in fibrogenesis. TGF-β favors accumulation of collagen and noncollagen basement membrane components by direct stimulation of production and by inhibiting matrix degradation enzymes such as collagenases and metalloproteinases. Activation of nuclear transcription factors, such as nuclear factor kappa B (NFκB) in injured kidney cells, [6] with consequent transcription and release of proinflammatory cytokines into the interstitium, appears to be a major mechanism of chronic tubulointerstitial inflammation accompanying proteinuric kidney diseases.
Etiology
Tubulointerstitial diseases of the kidney encompass diverse etiologies and pathophysiologic processes, and the patient can present with acute or chronic conditions. Many forms of tubulointerstitial injury involve exposure to drugs or other nephrotoxic agents such as heavy metals and, rarely, infection. By far the most common form of tubulointerstitial inflammation is hypersensitivity reaction to medications, termed allergic interstitial nephritis.
The following are causes of acute tubulointerstitial nephritis [7] :
-
Hypersensitivity reactions: Any pharmacologic agent can cause an acute allergic reaction involving the kidneys (eg, penicillins, sulfa drugs, antineoplastic agents, [8, 9] nonsteroidal anti-inflammatory drugs [NSAIDs], vaccines [10, 11] ) (See Presentation.)
-
Immunologic diseases (eg, associated with lupus, Goodpasture syndrome)
-
Acute transplant rejection
-
Infections, including bacterial (must be accompanied by obstruction or reflux), viral (eg, cytomegalovirus [CMV], hantavirus, human immunodeficiency virus [HIV], hepatitis B [HBV]), COVID-19, [11] fungal (eg, histoplasmosis), and parasitic (eg, Leishmania, Toxoplasma)
The following are causes of chronic tubulointerstitial nephritis:
-
Drugs (eg, analgesics, lithium, cyclosporine, tacrolimus) [12]
-
Heavy metals (eg, lead, cadmium, mercury)
-
Obstructive uropathy, nephrolithiasis, reflux disease
-
Immunologic diseases (eg, lupus, Sjögren syndrome, primary glomerulopathies, sarcoidosis, vasculitis, antineutrophil cytoplasmic antibody [ANCA]–associated vasculitides, [13] granulomatosis with polyangiitis, chronic transplant nephropathy)
-
Neoplasia (eg, myeloma, leukemia)
-
Atherosclerotic kidney disease (ischemic) - Underlying atherosclerotic disease, dyslipidemia, and smoking are conditions commonly associated with cholesterol microembolism; catheter manipulations above the level of the renal arteries or anticoagulation in a patient with atherosclerosis can trigger cholesterol microembolic disease
-
Metabolic diseases (eg, hypercalcemia, cystinosis, potassium depletion, hyperoxaluria)
-
Genetics (eg, Alport syndrome, medullary cystic disease, medullary amyloidosis [14] )
Lead nephropathy
Environmental and occupational exposure to lead can cause chronic tubulointerstitial nephritis. Occupations in welding, smelting, the battery industry, and mining have all been responsible for lead nephropathy cases. The removal of lead from gasoline in the United States has reduced environmental exposure, but sporadic cases from exposure to lead-based paint is still observed, particularly among children living in deteriorating older housing in urban areas. Rarely, lead poisoning can be observed in individuals who consume moonshine whiskey and those who drink beverages from imported ceramics painted with leaded glaze.
Obstructive uropathy
A variety of causes contribute to obstructive uropathy, including the following:
-
Prostate disease in elderly men
-
Pelvic or colonic tumors involving both ureters, in both sexes
-
Nephrolithiasis, with or without urinary tract infection
-
Radiation to the pelvic area
-
Drugs, such as methysergide, that can cause retroperitoneal fibrosis
Sjögren syndrome
In a study by Maripuri et al, kidney biopsies in 24 patients with primary Sjögren syndrome who also had kidney dysfunction revealed that 17 individuals had tubulointerstitial nephritis as the primary lesion, [17] and 11 of those 17 patients had the chronic form of this nephritis. The investigators suggested these results support the notion that in patients with primary Sjögren syndrome, chronic tubulointerstitial nephritis is the most frequent cause of renal impairment found through kidney biopsy.
Similarly, a prospective study by Jain et al of renal involvement in 70 patients with primary Sjögren syndrome reported that tubulointerstitial nephritis was the most common disorder found on kidney biopsy. Tubulointerstitial nephritis was identified in nine of 17 biopsies in this study. [18]
Balkan endemic nephropathy
Balkan endemic nephropathy is a form of chronic tubulointerstitial nephritis characterized by insidious onset, gradual progression to end-stage renal disease, and frequent association with urothelial carcinoma of the upper urinary tract (UTUC). The disease was reported in the Balkan peninsula of southeastern Europe, in rural areas around tributaries of the Danube River. It was eventually traced to consumption of home-baked bread made with flour contaminated with aristolochic acid from Aristolochia clematitis, a common weed in wheat fields in the region. [16]
Chinese herb/aristolochic acid nephropathy
In the early 1990s, aristolochic acid was recognized as a potent nephrotoxin that was causing rapidly progressive interstitial fibrosis and end-stage renal disease (ESRD) in young women using a Chinese herb as part of a slimming regimen in Belgium. Since then, many other cases of so-called Chinese herb (CH) nephropathy have been reported from around the world.
Chinese herb nephropathy may not be an appropriate name for the disease, however, because aristolochic acid can be present in herbal medicines from any country, and is the environmental phytotoxin that causes Balkan endemic nephropathy (see above). The term aristolochic acid nephropathy (AAN) more accurately characterizes this form of toxic nephropathy. [15]
As with Balkan endemic nephropathy, AAN from other causes is also associated with UTUC. This appears to occur because aristolochic acid can trigger oncogene mutations, including alterations in the tumor-suppressor gene TP53. [19]
IgG-4–related nephropathy
Immunoglobulin G (IgG)-4–related disease can affect almost any anatomic site, and often affects multiple sites, but approximately 20% of cases involve the kidney only. [20, 21, 22, 23] IgG4-related disease is characterized by high serum levels of IgG and IgG4, and in the kidney, tubulointerstitial nephritis with an abundant IgG4-positive plasma cell interstitial infiltration. [24]
Epidemiology
Primary tubulointerstitial diseases (ie, diseases of the renal tubules and interstitium sparing the glomeruli) constitute 10-15% of all kidney diseases both in the United States and around the world. In certain regions, such as the Balkans (ie, Yugoslavia, Bosnia, Croatia, Romania, Bulgaria), where endemic nephropathy is common, interstitial diseases may be more prevalent. [16]
Neither acute nor chronic tubulointerstitial diseases of the kidney demonstrate racial predilections. However, lead nephropathy may be more common in black people because of socioeconomic factors.
Analgesic nephropathy is 5-6 times more common in women. This is generally attributed to women taking more analgesics than men. However, a greater sensitivity to the toxic effects of analgesics or differences in analgesic metabolism in women cannot be ruled out.
All toxic nephropathies are related to the cumulative effects of toxic substances, particularly lead, and consequently are likely to be observed more frequently with advancing age. However, this is highly variable. For example, people with severe lead poisoning during childhood may present with chronic tubulointerstitial nephritis in early adult life. Atherosclerotic and/or ischemic kidney disease is increasingly common in elderly individuals. Metabolic disorders, such as cystinosis, oxalosis, and hypercalcemia, can occur in younger individuals.
Prognosis
Tubulointerstitial disease may progress to end-stage renal disease (ESRD) and thus require dialysis or transplantation. Electrolyte and acid-base disorders may also be observed, and an increased incidence of uroepithelial cancers is found among patients with analgesic nephropathy, aristolochic acid nephropathy, and Balkan endemic nephropathy. [15, 16]
Hypertension may also complicate any renal disease, but not all cases of interstitial renal disease are associated with hypertension (ie, Balkan endemic nephropathy, acute allergic interstitial nephritides).
Most patients with allergic interstitial nephritis recover renal function upon cessation of the offending agent.
Patients with cholesterol microembolic kidney disease often have some spontaneous improvement in renal function after the embolic event. Complete resolution of renal insufficiency is rare, however.
Although the natural history of chronic tubulointerstitial nephritides varies depending on the etiology, most chronic tubulointerstitial renal disease eventually progresses to ESRD. However, the rate of progression is generally believed to be much slower in tubulointerstitial nephritis than in glomerular diseases.
-
Tubulointerstitial nephritis: Kidney biopsy reveals acute interstitial nephritis. The renal cortex shows a diffuse interstitial, predominantly mononuclear, inflammatory infiltrate with no changes to the glomerulus. Tubules in the center of the field are separated by inflammation and edema, as compared with the more normal architecture in the right lower area (periodic acid–Schiff, 40 X).
-
Tubulointerstitial nephritis. On a kidney biopsy, the diagnosis of acute interstitial nephritis is based on the active inflammatory infiltrate on the right with unaffected glomeruli. Interstitial edema and fibrosis are present on the left side of the field, where some tubules show thickened basement membrane (hematoxylin and eosin, 20 X).
-
Tubulointerstitial nephritis. Kidney biopsy shows acute interstitial nephritis. The interstitium is expanded by mononuclear inflammatory infiltrate and edema. Acute tubular damage is present; some tubules are distended and contain granular casts (hematoxylin and eosin, 40 X).
-
Tubulointerstitial nephritis. Kidney biopsy shows acute crescentic glomerulonephritis. The glomerular tuft is compressed by the proliferation of epithelial cells, forming a crescent. In addition, the interstitium shows mononuclear inflammatory infiltrate and edema (periodic acid–Schiff, 40 X).
-
Tubulointerstitial nephritis. Kidney biopsy shows acute interstitial nephritis. The mononuclear inflammatory infiltrate contains abundant eosinophils, suggesting an allergic etiology. Severe tubular damage is observed (hematoxylin and eosin, 40 X).
-
Tubulointerstitial nephritis. Kidney biopsy shows acute interstitial nephritis. The inflammatory infiltrate forms an ill-defined granuloma, suggesting allergic or infectious etiologies. A partially destroyed tubule is present (periodic acid–Schiff, 40 X).
-
Tubulointerstitial nephritis. Kidney biopsy shows chronic tubulointerstitial nephritis. The interstitium is expanded by fibrosis, with distortion of tubules and periglomerular fibrosis. Glomeruli do not show pathologic changes (hematoxylin and eosin, 20 X).
-
Tubulointerstitial nephritis. Kidney biopsy in interstitial nephritis shows a cholesterol microembolism. The 2 arterioles in the center are occluded by elongated crystals (hematoxylin and eosin, 20 X).
-
Tubulointerstitial nephritis. Kidney biopsy in interstitial nephritis shows a cholesterol microembolism. The arteriole in the center of the field has a thickened wall. The lumen is occluded by elongated spaces, corresponding to dissolved crystals surrounded by cellular reaction. The 2 glomeruli flanking the arteriole are sclerotic and hardly recognizable (hematoxylin and eosin, 40 X).






