Practice Essentials
Aortic stenosis is the obstruction of blood flow across the aortic valve (see the image below). Among symptomatic patients with medically treated moderate-to-severe aortic stenosis, mortality from the onset of symptoms is approximately 25% at 1 year and 50% at 2 years. Symptoms of aortic stenosis usually develop gradually after an asymptomatic latent period of 10-20 years.
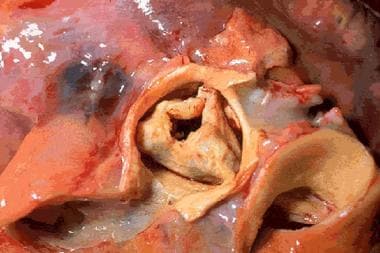 Stenotic aortic valve (macroscopic appearance).
Stenotic aortic valve (macroscopic appearance).
Signs and symptoms
The classic triad of symptoms in patients with aortic stenosis is as follows [1] :
-
Chest pain: Angina pectoris in patients with aortic stenosis is typically precipitated by exertion and relieved by rest.
-
Heart failure: Symptoms include paroxysmal nocturnal dyspnea, orthopnea, dyspnea on exertion, and shortness of breath.
-
Syncope: This often occurs upon exertion when systemic vasodilatation in the presence of a fixed forward stroke volume causes the arterial systolic blood pressure to decline.
Systolic hypertension can coexist with aortic stenosis. However, a systolic blood pressure higher than 200 mmHg is rare in patients with critical aortic stenosis.
In severe aortic stenosis, the carotid arterial pulse typically has a delayed and plateaued peak, decreased amplitude, and gradual downslope (pulsus parvus et tardus).
Other symptoms of aortic stenosis include the following:
-
Pulsus alternans: Can occur in the presence of left ventricular systolic dysfunction
-
Hyperdynamic left ventricle: Unusual; suggests concomitant aortic regurgitation or mitral regurgitation
-
Soft or normal S1
-
Diminished or absent A2: The presence of a normal or accentuated A2 speaks against the existence of severe aortic stenosis
-
Paradoxical splitting of the S2: Resulting from late closure of the aortic valve with delayed A2
-
Accentuated P2: In the presence of secondary pulmonary hypertension
-
Ejection click: Common in children and young adults with congenital aortic stenosis and mobile valve leaflets
-
Prominent S4: Resulting from forceful atrial contraction into a hypertrophied left ventricle
-
Systolic murmur: The classic crescendo-decrescendo systolic murmur of aortic stenosis begins shortly after the first heart sound; the intensity increases toward mid systole and then decreases, with the murmur ending just before the second heart sound
See Presentation for more detail.
Diagnosis
The following studies are used in the diagnosis and assessment of aortic stenosis:
-
Serum electrolyte levels
-
Cardiac biomarkers
-
Complete blood count
-
Electrocardiography (ECG): Serial ECG can demonstrate the progression of aortic stenosis
-
Chest radiography
-
Echocardiography: Two-dimensional and Doppler
-
Cardiac catheterization: Can be used if clinical findings are inconsistent with echocardiogram results
-
Coronary angiography
-
Radionuclide ventriculography: May provide information on left ventricular function
-
Exercise stress testing: Contraindicated in symptomatic patients with severe aortic stenosis
See Workup for more detail.
Management
The only definitive treatment for aortic stenosis in adults is aortic valve replacement (surgical or percutaneous). The development of symptoms due to this condition provides a clear indication for replacement. [4, 5] Infants, children, and adolescents with a bicuspid valve may undergo balloon or surgical valvotomy.
Emergency care
A patient presenting with uncontrolled heart failure should be treated supportively with oxygen, cardiac and oximetry monitoring, intravenous access, loop diuretics, nitrates (keep in mind the potential nitrate sensitivity of patients with aortic stenosis), morphine (as needed and tolerated), and noninvasive or invasive ventilatory support (as indicated). Patients with severe heart failure due to aortic stenosis that is resistant to medical management should be considered for urgent surgery.
Pharmacologic therapy
Agents used in the treatment of patients with aortic stenosis include the following:
-
Digitalis, diuretics, and angiotensin-converting enzyme (ACE) inhibitors: Can be cautiously used in patients with pulmonary congestion
-
Vasodilators: May be used to treat for heart failure and for hypertension but should also be employed with extreme caution
-
Digoxin, diuretics, ACE inhibitors, or angiotensin receptor blockers [5] : Recommended by the European Society of Cardiology (ESC)/European Association for Cardio-Thoracic Surgery (EACTS) guidelines for patients with heart failure symptoms who are not suitable candidates for surgery or transcatheter aortic valve implantation
Aortic valve replacement
According to American College of Cardiology (ACC)/American Heart Association (AHA) guidelines, candidates for aortic valve replacement include the following patients [6] :
-
Symptomatic patients with severe aortic stenosis
-
Patients with asymptomatic, severe aortic stenosis undergoing coronary artery bypass surgery
-
Patients with asymptomatic, severe aortic stenosis undergoing surgery on the aorta or other heart valves
-
Patients with asymptomatic, severe aortic stenosis and left ventricular systolic dysfunction (ejection fraction < 0.50)
Percutaneous balloon valvuloplasty
Percutaneous balloon valvuloplasty is used as a palliative measure in critically ill adult patients who are not surgical candidates or as a bridge to aortic valve replacement in critically ill patients.
See Treatment and Medication for more detail.
Background
Aortic stenosis is the obstruction of blood flow across the aortic valve. Aortic stenosis has several etiologies, including congenital (unicuspid or bicuspid valve), calcific (due to degenerative changes), and rheumatic. Degenerative calcific aortic stenosis is now the leading indication for aortic valve replacement. The favorable long-term outcome following aortic valve surgery and the relatively low operative risk emphasize the importance of an accurate and timely diagnosis (see Prognosis).
A stenotic valve is shown in the image above. Symptoms of aortic stenosis usually develop gradually after an asymptomatic latent period of 10-20 years. Exertional dyspnea or fatigue is the most common initial complaint. Ultimately, most patients experience the classic triad of chest pain, heart failure, and syncope (see History).
Two-dimensional (2D) Doppler echocardiography is the imaging modality of choice to diagnose and estimate the severity of aortic stenosis and localize the level of obstruction (see Workup). The only definitive treatment for aortic stenosis is aortic valve replacement, either surgically or percutaneously. (see Treatment).
Go to Pediatric Valvar Aortic Stenosis, Pediatric Subvalvar Aortic Stenosis, and Pediatric Supravalvar Aortic Stenosis for more complete information on these topics.
Pathophysiology
When the aortic valve becomes stenotic, resistance to systolic ejection occurs and a systolic pressure gradient develops between the left ventricle and the aorta. This outflow obstruction leads to an increase in left ventricular (LV) systolic pressure. As a compensatory mechanism to normalize LV wall stress, LV wall thickness increases by parallel replication of sarcomeres, producing concentric hypertrophy. At this stage, the chamber is not dilated and ventricular function is preserved, although diastolic compliance is reduced.
Eventually, however, LV end-diastolic pressure (LVEDP) rises, which causes a corresponding increase in pulmonary capillary arterial pressures and a decrease in cardiac output due to diastolic dysfunction. The contractility of the myocardium may also diminish, which leads to a decrease in cardiac output due to systolic dysfunction. Ultimately, heart failure develops.
In most patients with aortic stenosis, LV systolic function is preserved and cardiac output is maintained for many years despite an elevated LV systolic pressure. Although cardiac output is normal at rest, it often fails to increase appropriately during exercise, which may result in exercise-induced symptoms.
Diastolic dysfunction may occur as a consequence of impaired LV relaxation and/or decreased LV compliance, as a result of increased afterload, LV hypertrophy, or myocardial ischemia. LV hypertrophy often regresses following relief of valvular obstruction. However, some individuals develop extensive myocardial fibrosis, which may not resolve despite regression of hypertrophy.
In patients with severe aortic stenosis, atrial contraction plays a particularly important role in diastolic filling of the LV. Thus, development of atrial fibrillation in aortic stenosis often leads to heart failure due to an inability to maintain cardiac output.
Increased LV mass, increased LV systolic pressure, and prolongation of the systolic ejection phase all elevate the myocardial oxygen requirement, especially in the subendocardial region. Although coronary blood flow may be normal when corrected for LV mass, coronary flow reserve is often reduced.
Myocardial perfusion is thus compromised by the relative decline in myocardial capillary density and by a reduced diastolic transmyocardial (coronary) perfusion gradient due to elevated LV diastolic pressure. Therefore, the subendocardium is susceptible to underperfusion, which results in myocardial ischemia.
Angina results from a concomitant increased oxygen requirement by the hypertrophic myocardium and diminished oxygen delivery secondary to diminished coronary flow reserve, decreased diastolic perfusion pressure, and relative subendocardial myocardial ischemia.
There may exist a causal association between LDL-C-related genetic variants and aortic valve disease. In a community-based study consisting of 6942 subjects with data on aortic valve calcium and more than 28,000 subjects with aortic stenosis (follow-up, >16 y), Smith et al found that genetic predisposition toward elevations in low-density lipoprotein cholesterol (LDL-C) (as indicated by genetic risk scores [GRSs])—but not elevated high-density lipoprotein cholesterol (HDL-C) or triglycerides GRSs—were associated with the presence of aortic valve calcium and the incidence of aortic stenosis. [7] Whether early intervention aimed at reducing LDL-C levels may help to prevent aortic valve disease is unknown.
Etiology
Most cases of aortic stenosis are due to the obstruction at the valvular level. Common causes are summarized in Table 1.
Table 1. Common Causes of Aortic Stenosis Among Patients Requiring Surgery (Open Table in a new window)
Age < 70 years (n=324) |
Age >70 years (n=322) |
Bicuspid AV (50%) Postinflammatory (25%) Degenerative (18%) Unicommissural (3%) Hypoplastic (2%) Indeterminate (2%) |
Degenerative (48%) Bicuspid (27%) Postinflammatory (23%) Hypoplastic (2%) |
Valvular aortic stenosis can be either congenital or acquired.
Congenital valvular aortic stenosis
Congenitally unicuspid, bicuspid, tricuspid, or even quadricuspid valves may cause aortic stenosis. In neonates and infants younger than 1 year, a unicuspid valve can produce severe obstruction and is the most common anomaly in infants with fatal valvular aortic stenosis. In patients younger than 15 years, unicuspid valves are most frequent in cases of symptomatic aortic stenosis.
In adults who develop symptoms from congenital aortic stenosis, the problem is usually a bicuspid valve. Bicuspid valves do not cause significant narrowing of the aortic orifice during childhood. The altered architecture of the bicuspid aortic valve induces turbulent flow with continuous trauma to the leaflets, ultimately resulting in fibrosis, increased rigidity and calcification of the leaflets, and narrowing of the aortic orifice in adulthood.
A cohort study by Tzemos et al of 642 ambulatory adults with bicuspid aortic valves found that during the mean follow-up duration of 9 years, survival rates were not lower than for the general population. However, young adults with bicuspid aortic valve had a high likelihood of eventually requiring aortic valve intervention. [8]
Congenitally malformed tricuspid aortic valves with unequally sized cusps and commissural fusion (“functionally bicuspid” valves) can also cause turbulent flow leading to fibrosis and, ultimately, to calcification and stenosis. Clinical manifestations of congenital aortic stenosis in adults usually appear after the fourth decade of life.
Acquired valvular aortic stenosis
The main causes of acquired aortic stenosis include degenerative calcification and, less commonly, rheumatic heart disease.
Degenerative calcific aortic stenosis (also called senile calcific aortic stenosis) involves progressive calcification of the leaflet bodies, resulting in limitation of the normal cusp opening during systole. This represents a consequence of long-standing hemodynamic stress on the valve and is currently the most frequent cause of aortic stenosis requiring aortic valve replacement. The calcification may also involve the mitral annulus or extend into the conduction system, resulting in atrioventricular or intraventricular conduction defects.
Risk factors for degenerative calcific aortic stenosis include advanced age, hypertension, hypercholesterolemia, diabetes mellitus, and smoking. The available data suggest that the development and progression of the disease are due to an active disease process at the cellular and molecular level that shows many similarities with atherosclerosis, ranging from endothelial dysfunction to, ultimately, calcification. [9]
In rheumatic aortic stenosis, the underlying process includes progressive fibrosis of the valve leaflets with varying degrees of commissural fusion, often with retraction of the leaflet edges and, in certain cases, calcification. As a consequence, the rheumatic valve often is regurgitant and stenotic. Coexistent mitral valve disease is common.
Other, infrequent causes of aortic stenosis include obstructive vegetations, homozygous type II hypercholesterolemia, Paget disease, Fabry disease, ochronosis, and irradiation.
It is worthwhile to note that although differentiation between tricuspid and bicuspid aortic stenosis is frequently made, it is often difficult to determine the number of aortic valve leaflets. A study comparing operatively excised aortic valve structure evaluation by cardiac surgeons versus pathologists found that valve structure determination was frequently incongruous. [10]
Epidemiology
Severe aortic stenosis is rare in infancy, occurring in 0.33% of live births, and is due to a unicuspid or bicuspid valve. Most patients with a congenitally bicuspid aortic valve who develop symptoms do not do so until middle age or later. Patients with rheumatic aortic stenosis typically present with symptoms after the sixth decade of life.
Aortic sclerosis (aortic valve calcification without obstruction to blood flow, considered a precursor of calcific degenerative calcific aortic stenosis) increases in incidence with age and is present in 29% of individuals older than 65 years and in 37% of individuals older than 75 years. In elderly persons, the prevalence of aortic stenosis is between 2% and 9%.
Degenerative calcific aortic stenosis usually manifests in individuals older than 75 years and occurs most frequently in males. [4]
Prognosis
Patients with severe aortic stenosis may be asymptomatic for many years despite the presence of severe LV outflow tract obstruction (LVOTO). LVOTOs have been associated with “high heritability.” One study suggests that 20% of patients with isolated LVOTO had an affected first-degree relative with undetected bicuspid aortic valves. [11]
Asymptomatic patients, even with critical aortic stenosis, have an excellent prognosis for survival, with an expected death rate of less than 1% per year; only 4% of sudden cardiac deaths in severe aortic stenosis occur in asymptomatic patients. A new proposed aortic stenosis grading classification that integrates valve area and flow-gradient patterns has been found to allow for better characterization of the clinical outcome among patients with asymptomatic severe aortic stenosis. [12]
In general, the presence of low-gradient "severe stenosis" (defined as aortic valve area < 1.0 cm2 and mean gradient 40 mmHg), representing up to 40% of all patients with aortic stenosis, is considered to be associated with a poor prognosis. [13] However, the prospective Simvastatin and Ezetimibe in Aortic Stenosis (SEAS) study found that such patients have an outcome similar to that of patients with moderate stenosis. [14] A more recent study found that symptomatic paradoxical low-gradient severe aortic stenosis is associated with a poorer prognosis even after adjustment for flow status and aortic stenosis severity. [15] Moreover, the investigators indicated there may be a possible link to heart failure with preserved ejection fraction in some symptomatic patients. [15]
Among symptomatic patients with medically treated, moderate-to-severe aortic stenosis, mortality rates from the onset of symptoms are approximately 25% at 1 year and 50% at 2 years. More than 50% of deaths are sudden. In patients in whom the aortic valve obstruction remains unrelieved, the onset of symptoms predicts a poor outcome with medical therapy; the approximate time interval from the onset of symptoms to death is 1.5-2 years for heart failure, 3 years for syncope, and 5 years for angina.
Although the obstruction tends to progress more rapidly in degenerative calcific aortic valve disease than in congenital or rheumatic disease, predicting the rate of progression in individual patients is not possible. Catheterization and echocardiographic studies suggest that, on average, the valve area declines 0.1 to 0.3 cm2 per year; the systolic pressure gradient across the valve can increase by as much as 10-15 mmHg per year. Obstruction progresses more rapidly in elderly patients with coronary artery disease and chronic renal insufficiency.
Epicardial adipose tissue (EAT) volume appears to be associated with adverse outcomes in patients with severe aortic stenosis undergoing transcatheter aortic valve replacement (TAVR). A retrospective study of 503 such patients found EAT volume was independently associated with all-cause 1-, 2-, and 3-year mortality and the early safety endpoint at 30 days. [16]
Complications
Possible complications of aortic stenosis include the following:
-
Conduction defects
-
Calcific embolization
-
Stenotic aortic valve (macroscopic appearance).
Tables
Age < 70 years (n=324) |
Age >70 years (n=322) |
Bicuspid AV (50%) Postinflammatory (25%) Degenerative (18%) Unicommissural (3%) Hypoplastic (2%) Indeterminate (2%) |
Degenerative (48%) Bicuspid (27%) Postinflammatory (23%) Hypoplastic (2%) |
Severity |
Mean gradient (mmHg) |
Aortic valve area (cm2) |
Mild |
< 25 |
>1.5 |
Moderate |
25-40 |
1-1.5 |
Severe |
>40 |
< 1 (or < 0.5 cm2/m2 body surface area) |
Critical |
>80 |
< 0.5 |
Indication |
Class |
Symptomatic severe high-gradient AS (Stage D1) |
I |
Asymptomatic severe AS (Stage C2) with and LVEF < 50% |
I |
Severe AS (Stage C or D) undergoing other cardiac surgery |
I |
Asymptomatic, very severe AS (Stage C1, aortic velocity ≥5.0 m/s) and low surgical risk |
IIa |
| Asymptomatic, severe AS (Stage C1) and decreased expercise tolerance or an exercise fall in blood pressure | IIa |
| Symptomatic severe low flow/low gradient AS with reduced LVEF (Stage D2) with a low-dose dobutamine stress study with aortic velocity ≥4.0 m/s with a value are ≤1.0 cm2 at any dobutamine dose | IIa |
| Symptomatic severe low flow/low gradient AS (Stage D3) who are normotensive and have an LVEF ≥50% if clinical, hemodynamic and anatomic data support valve obstruction as the most likely cause of symptoms | IIa |
| Moderate AS (Stage B) who are undergoing other cardiac surgery | IIa |
| Asymptomatic severe AS (Stage C1) with rapid disease progression and low surgical risk | IIb |
Intervention Selection |
AHA/ACC (2014) [6] |
ESC/EACTS (2012) [5] |
STS(2013) [56] |
Surgical AVR in patients with low or intermediate surgical risk |
Class I |
Class I |
|
Transcatheter aortic valve replacement (TAVR) for patients who have a prohibitive surgical risk and a predicted post-TAVR survival >12 mo |
Class I |
Class I |
Class I |
TAVR for patients who have high surgical risk |
Class IIa-Reasonable |
Class IIa-Reasonable |
|
TAVR is not recommended in patients in whom existing comorbidities would preclude the expected benefit from correction of AS |
Class III |
Class III |
|
Balloon aortic valvuloplasty (BAV) as a bridge to surgical AVR or TAVR in severely symptomatic patients |
Class IIb-Consider |
Class IIb-Consider |
Class IIa-Reasonable |
BAV as bridge to AVR in hemodynamically unstable patients with severe AS where immediate AVR is not feasible |
Class IIb-Consider |
Class IIa-Reasonable |
|
BAV in severely symptomatic patients where AVR is not an option for symptom relief |
Class IIb-Consider |
||
BAV as a palliative measure when surgery is contraindicated because of severe comorbidities |
Class IIb-Consider |
Class IIb-Consider |

What would you like to print?
- Overview
- Presentation
- DDx
- Workup
- Treatment
- Guidelines
- 2021 ACC/AHA Valvular Heart Disease Clinical Practice Guidelines
- 2021 ESC/EACTS Management of Valvular Heart Disease (VHD) Clinical Practice Guidelines
- 2017 Multisociety Appropriate Use Criteria
- 2017 AHA/ACC Guidelines for the Management of Patients with Valvular Heart Disease
- 2014 Multisociety Guidelines for the Management of Valvular Heart Disease
- Show All
- Medication
- Questions & Answers
- Tables
- References




