Practice Essentials
Lymphedema (see the image below) is an abnormal collection of protein-rich fluid in the interstitium resulting from obstruction of lymphatic drainage. Lymphatic obstruction causes an increase in the protein content of the extravascular tissue, with subsequent retention of water and swelling of the soft tissue. The increase in the extravascular protein stimulates proliferation of fibroblasts, organization of the fluid, and the development of a nonpitting swelling of the affected extremity.
 Lymphedema in a patient with hypertension, diabetes, and impaired cardiac function.
Lymphedema in a patient with hypertension, diabetes, and impaired cardiac function.
Signs and symptoms
Signs and symptoms of lymphedema include the following:
-
Chronic swelling of an extremity preceded lymphedema
-
Primarily lower extremity involvement (80%) but can also involve the upper extremities, face, genitalia, and trunk
-
Fevers, chills, and generalized weakness
-
Fatigue related to the size and weight of the extremity
-
Embarrassment in public
-
Severe impairment of daily activities
-
Recurrent bacterial or fungal infections
-
Recurrent episodes of cellulitis, lymphangitis, fissuring, ulcerations, and/or verrucous changes
See Clinical Presentation for more detail.
Diagnosis
Examination in a patient with lymphedema may reveal the following findings:
-
Nontender, pitting edema of the affected area, most commonly in the distal extremities; over time, radial enlargement of the area, progressing to a nonpitting edema
-
Erythema of the affected area and thickening of the skin, which appears as peau d'orange skin and woody edema
-
Elephantiasis nostra verrucosa (with long-term involvement): An area of cobble-stoned, hyperkeratotic, papillomatous plaques most commonly seen on the shins; the plaques can be covered with a loosely adherent crust, can be weepy or oozing a clear or yellow fluid, and/or can have a foul-smelling odor. Lymphedema from Kaposi sarcoma so severe as to be evident as elephantiasis nostras verrucose may occur. [1]
-
Fissuring, ulcerations, skin breakdown, and lymphorrhea
-
Superinfection: Common and can manifest as impetigo with yellow crusts
-
Positive Stemmer sign (inability to pinch the dorsal aspect of skin between the first and second toes)
-
Detection of early mild arm lymphedema may be facilitated by using cutaneous palpation in combination with determining the tissue dielectric constant, which evaluates local tissue water in the skin and upper subcutis, measured from fixed measurement sites. [2]
Other associated physical findings specific for the cause of secondary lymphedema and genetic disorders involving lymphedema may be noted upon examination.
Testing
In general, analysis of blood, urine, or tissue is not needed to make the diagnosis of lymphedema. Such tests, however, help to define the underlying causes of lower extremity edema when the etiology is unclear.
If a renal or hepatic etiology is suspected, obtain the following laboratory tests:
-
Liver function tests
-
Blood urea nitrogen/creatinine levels
-
Urinalysis
If a neoplasm is suspected, obtain results for specific markers. Obtain a complete blood count with differential if an infectious etiology is being considered.
Imaging studies
Imaging is not necessary to make the diagnosis of lymphedema, but it can be used to confirm it, to assess the extent of involvement, and to determine therapeutic intervention. Such studies may include the following:
-
Plain radiographs: To exclude abnormalities of the bone
-
Computed tomography scanning: When malignancy is suspected
-
Magnetic resonance imaging: When malignancy is suspected or to show lymph trunk anatomy and causes of obstructive secondary lymphedema
-
Ultrasonography: To evaluate the lymphatic and venous systems
-
Fluorescence microlymphography: To demonstrate a lack of microlymphatics
-
Lymphoscintigraphy: Criterion standard for evaluation of the lymphatic system
Procedures
Perform a biopsy if the diagnosis is not clinically apparent, if areas of chronic lymphedema look suspicious, or if areas of chronic ulceration exist.
See Workup for more detail.
Management
The goal of lymphedema therapy is to restore function, reduce physical and psychologic suffering, and prevent the development of infection. In secondary lymphedema, the underlying etiology (ie, neoplasm, infection) should also be properly treated, in order to relieve the lymphatic obstruction. The natural history and morbidity of lymphedema may be related to patient's body mass index (BMI). An active lifestyle with a normal BMI tends to portend less severe disease as compared to those who are obese. [3]
Pharmacotherapy
The following medications are used in to manage lymphedema:
-
Benzopyrones (eg, coumarin, flavonoids)
-
Retinoidlike agents (eg, acitretin, topical tazarotene)
-
Anthelmintic agents (eg, albendazole)
-
Topical skin products (eg, ammonium lactate lotion, topical urea)
-
Antibiotics (eg, cefazolin, clindamycin, penicillin G)
Nonpharmacotherapy
Conservative measures for managing lymphedema include the following:
-
Maintenance of appropriate hygiene and skin care
-
Use of complex physical therapy (first-line treatment) [4] and compression stockings
-
Weight loss (if overweight)
-
Avoiding trauma
-
Avoiding constrictive clothing
-
Elevating affected limb
Surgical option
Surgical treatment is palliative, not curative, and it does not obviate the need for continued medical therapy. Procedures are divided into physiologic (to improve lymphatic drainage) and excisional (removal of the affected tissues to reduce the lymphedema-related load) surgeries.
Surgical intervention is reserved for patients who do not improve with conservative measures or for cases in which the extremity is so large that it impairs daily activities and prevents successful conservative management.
See Treatment and Medication for more detail.
Background
Lymphedema is an abnormal collection of protein-rich fluid in the interstitium resulting from obstruction of lymphatic drainage. Lymphatic obstruction causes an increase in the protein content of the extravascular tissue, with subsequent retention of water and swelling of the soft tissue. The increase in the extravascular protein stimulates proliferation of fibroblasts, organization of the fluid, and the development of a nonpitting swelling of the affected extremity (see the image below). (See Pathophysiology and Etiology.)
Lymphedema in a patient with hypertension, diabetes, and impaired cardiac function.
Fibrosis also obstructs the lymphatic channels and leads to increased protein concentration in the tissues, continuing this cycle. Lymphedema most commonly affects the extremities, but it can involve the face, genitalia, or trunk. (See Etiology, Pathophysiology, and Presentation.)
In addition to causing soft tissue swelling, lymphedema opens channels in the integument and allows bacteria to enter the subcuticular space, which overwhelms host defenses and leads to cellulitis of the extremity. (See Pathophysiology, Prognosis, Treatment, and Medication.)
Lymphedema is classified into primary and secondary forms. Primary lymphedema (which results from genetic factors) is caused by abnormalities in the lymphatic system that are present at birth, although not always clinically evident until later in life. Primary lymphedema can also be associated with various cutaneous syndromes. The three categories of primary lymphedema are as follows (see Etiology and Workup):
-
Congenital lymphedema (Milroy disease)
-
Lymphedema praecox (Meige disease)
-
Lymphedema tarda
Secondary lymphedema occurs as a result of obstruction of lymphatic flow by known mechanisms, including the following (see Etiology and Workup):
-
Filariasis
-
Silica
-
Podoconiosis, which occurs in barefoot subsistence farmers after walking on red volcanic soil, mostly commonly in Ethiopia [5]
-
Obstruction by a proximal mass
-
Postsurgical mechanisms - Eg, mastectomy
-
Fibrosis secondary to chronic infections
-
Unilateral lower extremity edema (as a complication of non-Hodgkin lymphoma) [6]
-
Massive obesity (termed massive localized lymphedema or obesity-related lymphedema) [7, 8] : The risk of lower extremity lymphedema has been correlated with body mass index (BMI), such that BMI less than 40 is 0%, BMI of 40-49 is 17%, BMI of 50-59 is 63%, BMI of 60-69 is 86%, BMI of 70-79 is 91%, and BMI of 80 or greater is 100%. [9]
-
Edema (giant penile elephantiasis) after circumcision of the penis [10]
Pathophysiology
Normal lymphatic physiology
The normal function of the lymphatics is to return proteins, lipids, and water from the interstitium to the intravascular space; 40-50% of serum proteins are transported by this route each day. High hydrostatic pressures in arterial capillaries force proteinaceous fluid into the interstitium, resulting in increased interstitial oncotic pressure that draws in additional water.
Interstitial fluid normally contributes to the nourishment of tissues. About 90% of the fluid returns to the circulation via entry into venous capillaries. The remaining 10% is composed of high-molecular-weight proteins and their oncotically associated water, which are too large to readily pass through venous capillary walls. This leads to flow into the lymphatic capillaries, where pressures are typically subatmospheric and can accommodate the large size of the proteins and their accompanying water. The proteins then travel as lymph through numerous filtering lymph nodes on their way to join the venous circulation.
Disease-related changes in lymphatic flow and their effects
In a diseased state, the lymphatic transport capacity is reduced. Consequently, the normal volume of interstitial fluid formation exceeds the rate of lymphatic return, resulting in the stagnation of high-molecular-weight proteins in the interstitium. This usually occurs after flow has been reduced by 80% or more. The result, as compared with forms of edema that have much lower concentrations of protein, is high-protein edema, or lymphedema, with protein concentrations of 1.0-5.5 g/mL. This high oncotic pressure in the interstitium favors the accumulation of additional water.
Accumulation of interstitial fluid leads to massive dilatation of the remaining outflow tracts and valvular incompetence that causes reversal of flow from subcutaneous tissues into the dermal plexus. The lymphatic walls undergo fibrosis, and fibrinoid thrombi accumulate within the lumen, obliterating much of the remaining lymph channels. Spontaneous lymphovenous shunts may form. Lymph nodes harden and shrink, losing their normal architecture.
In the interstitium, protein and fluid accumulation initiates a marked inflammatory reaction. Macrophage activity is increased, resulting in destruction of elastic fibers and production of fibrosclerotic tissue. Fibroblasts migrate into the interstitium and deposit collagen. The result of this inflammatory reaction is a change from the initial pitting edema to the brawny nonpitting edema characteristic of lymphedema. Consequently, local immunologic surveillance is suppressed, and chronic infections, as well as malignant degeneration to lymphangiosarcoma, may occur. [11]
Dermatologic pathology
The overlying skin becomes thickened and displays the typical peau d'orange (orange skin) appearance of congested dermal lymphatics.
Chronic lymphedema causes fissuring and impairment of the epidermis, allowing bacteria to enter and grow, and leading to lymphorrhea, the leakage of lymph onto the surface of the skin. With chronic lymphedema, the development of verrucous, cobblestone plaques, a condition known as elephantiasis nostra verrucosa (ENV), can occur.
Protein composition in lymphedema
A theory has also been proposed that chronic lymphedema changes the protein composition of lymph in affected areas. A decrease in alpha-2 globulin levels and an increase in the albumin-to-globulin ratio have been reported. This change in proteins and the resultant slowing of transport to the lymphoid tissue have been suggested to play a role in diminishing the effectiveness of immune surveillance and to prevent early detection of tumor-specific antigens.
Additionally, repeat episodes of chronic ulceration and healing may stimulate the proliferation of keratinocytes, which may contribute to neoplastic transformation.
Etiology
Lymphedema is caused by a compromised lymphatic system that impedes and diminishes lymphatic return. In primary lymphedema, the failure is caused by congenital hypoplasia or aplasia of the peripheral lymphatics or by valvular incompetence. In secondary lymphedema, the lymphatic drainage is altered by an acquired blockade of the lymph nodes or by disruption of the local lymphatic channels caused by one of the following etiologies:
-
Recurrent attacks of lymphangitis - A key type of this is cellulitis
-
Malignancy
-
Obesity
-
Surgery
Whether the cause is acquired blockade of the lymph nodes or disruption of the local lymphatic channels, the result is a failure to drain protein-rich lymphatic fluid from the tissue, causing interstitial edema with swelling of the affected site. (See the image below.
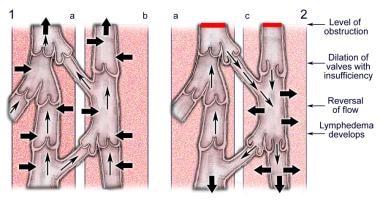 (1) Normal lymphatic flow in (a) deep systems and (b) superficial systems. Note the small collateral vessels interconnecting the 2 systems. (2) Lymphedema develops from obstruction, dilation of valves, valvular insufficiency, and subsequent reversal of lymphatic flow.
(1) Normal lymphatic flow in (a) deep systems and (b) superficial systems. Note the small collateral vessels interconnecting the 2 systems. (2) Lymphedema develops from obstruction, dilation of valves, valvular insufficiency, and subsequent reversal of lymphatic flow.
Although etiology determines the classification of lymphedema as either primary or secondary, it rarely impacts the choice of treatment. [12]
Primary lymphedema
Lymphedema arising from a developmental abnormality of the lymphatic system is classified as primary lymphedema. [12] This form of the disease is divided into the following 3 main types, which are distinguished by their age of onset. (Connell et al proposed a classification system of the primary lymphatic dysplasias that is based on phenotype rather than age of onset. [13] ) These types are as follows:
-
Congenital lymphedema (Milroy disease)
-
Lymphedema praecox (Meige disease)
-
Lymphedema tarda
These conditions involve the lower extremities almost exclusively. All are caused by a congenital abnormality in the lymphatic system, although these defects may not always be clinically evident until later in life, when a triggering event or worsening of the condition causes the lymphatic transport capacity to exceed the volume of interstitial fluid formation; in such cases, the patient is unable to maintain normal lymphatic flow.
Primary lymphedema also can be associated with other cutaneous and genetic disorders not among the 3 main, age-based categories.
Congenital lymphedema
Congenital lymphedema, or Milroy disease, accounts for 10-25% of all primary lymphedema cases. A familial, autosomal-dominant disorder, it is often caused by anaplastic lymphatic channels. The disorder manifests at birth or later, up to age 1 year. Females are affected twice as often as males, and the lower extremities are involved 3 times more frequently than the upper extremities. The edema is most commonly pitting and nonpainful. Patients may have bilateral lymphedema, and this form may improve spontaneously with increasing age. Unilateral lymphedema is not noted in Milroy disease, but if it were, it might spontaneously improve with age.
Congenital lymphedema has also been associated with cellulitis, prominent veins, intestinal lymphangiectasias, upturned toenails, and hydrocele.
Although congenital lymphedema is classically thought to be caused by the failure of lymphatic vessels to develop in utero, examination of patients with this disease by fluorescence microlymphangiography demonstrated a high rate of functional failure of the lymphatic system. [14, 15] Such failure may play a role in the development of edema.
Several mutations can cause lymphedema; new variants are being delineated. [3] Congenital lymphedema may be linked to a mutation that inactivates VEGFR3. This gene, which is expressed in adult lymphatic endothelial cells, has been mapped to the telomeric part of chromosome arm 5q in the region 5q34-q35. This region codes for a tyrosine kinase receptor specific for the function of the lymphatic vessels, and indeed, the receptor has been reported to be abnormally phosphorylated in patients with Milroy disease. [16, 17, 18, 19, 20, 21, 22]
Lymphedema praecox
Lymphedema praecox, also known as Meige disease, is the most common form of primary lymphedema. By definition, this disease becomes clinically evident after birth and before age 35 years. The condition accounts for 65-80% of all primary lymphedema cases and most often arises during puberty. About 70% of cases are unilateral, with the left lower extremity being involved more often than the right. Histologically, these patients are likely to demonstrate a hypoplastic pattern, with the lymphatics reduced in caliber and number.
Females are affected 4 times as often as males. The fact that lymphedema praecox usually manifests clinically around menarche suggests that estrogen may play a role in its pathogenesis.
Lymphedema tarda
Lymphedema tarda manifests later in life, usually in persons older than 35 years. It is thought to be caused by a defect in the lymphatic valves, resulting in incompetent valve function. Whether this defect is congenital or acquired is difficult to determine.
As the rarest form of primary lymphedema, this disease accounts for only 10% of cases. Histologically, patients are likely to demonstrate a hyperplastic pattern, with tortuous lymphatics increased in caliber and number.
Associated conditions
As mentioned, primary lymphedema is seen in association with various cutaneous and genetic disorders.
Distichiasis lymphedema syndrome is a form of hereditary early and late-onset lymphedema associated with distichiasis (double row of eyelashes). Affected persons usually manifest bilateral lower extremity lymphedema by age 8-30 years. Lymphatic vessels are usually larger in affected areas. It is a hereditary condition with an autosomal dominant pattern with variable penetrance. It reportedly is associated with a mutation in the FOXC2 transcription factor. [23] Other associated anomalies may include vertebral abnormalities, spinal arachnoid cysts, hemangiomas, cleft palate, ptosis, short stature, webbed neck, strabismus, thoracic duct abnormalities, and microphthalmia.
Primary lymphedema has also been associated with yellow nail syndrome. This entity may be associated with recurrent pleural effusions and bronchiectasis.
Other genetic syndromes and cutaneous conditions associated with primary lymphedema include the following:
-
Turner syndrome
-
Noonan syndrome
-
Klinefelter syndrome
-
Neurofibromatosis type 1
-
Hemangiomas
-
Xanthomatosis
-
Congenital absence of nails
One case reportedly occurred in association with CHARGE (coloboma, heart anomalies, choanal atresia, somatic and intellectual disability, genitourinary anomalies, ear abnormalities) syndrome. [24]
Secondary lymphedema
Secondary Lymphedema is caused by an acquired defect in the lymphatic system and is commonly associated with obesity, infection, neoplasm, trauma, and therapeutic modalities. It may also be associated with intravenous drug abuse. [25] Puffy hand syndrome is associated with lymphedema-cellulitis-venous thrombosis of the hand in intravenous drug abusers.
Filariasis
The most common cause of secondary lymphedema worldwide is filariasis, a disease caused by a mosquito-borne nematode infection with the parasite Wucheria bancrofti. Commonly occurring in developing countries around the world, this infection results in permanent lymphedema of the limb. [26, 27, 28] The major immunological feature of lymphatic filariasis appears to be an antigen-specific Th2 response, with an expansion of interleukin 10 secreting CD4+ T cells; such an immunological pattern involves a muted Th1 response. [29]
Malignancy and cancer treatment
In the industrialized world, the most common causes of secondary lymphedema are malignancy and its treatment. This means that the disease can arise from obstruction from metastatic cancer or primary lymphoma or can be secondary to radical lymph node dissection and excision.
Although lymphatics are thought to regenerate after transection via surgery, when combined with radiotherapy to the area, the risk of lymphedema increases because of scarring and fibrosis of the tissue. The most commonly affected area is the axillary region after mastectomy and radical dissection for breast cancer.
Lymphedema can also be seen after regional dissection of pelvic, para-aortic, and neck lymph nodes. Other associated neoplastic diseases are Hodgkin lymphoma, metastatic prostate cancer, cervical cancer, breast cancer, Kaposi sarcoma, and melanoma.
The concept of Ruocco’s immunocompromised cutaneous district may explain the association of lymphedema with opportunistic infections, including viral warts, tumors (including angiosarcoma, basal cell carcinoma, squamous cell carcinoma, and sebaceous carcinoma), and immune reactions. [30, 31]
Other causes
Morbid obesity frequently causes impairment of lymphatic return and commonly results in lymphedema, as shown in the image below. This entity can be termed massive localized lymphedema [7, 8] or obesity-related lymphedema.

Lymphedema is also associated with the following etiologies (see the image below):
-
Trauma
-
Varicose vein surgery
-
Congestive heart failure
-
Portal hypertension
-
Peripheral vascular surgery
-
Lipectomy
-
Burns
-
Burn scar excision
-
Insect bites
-
Extrinsic pressure
 Lymphedema in a patient with hypertension, diabetes, and impaired cardiac function.
Lymphedema in a patient with hypertension, diabetes, and impaired cardiac function.
Recurrent episodes of cellulitis or streptococcal lymphangitis have also been linked to the development of lymphedema.
Rarely, herpes simplex infection can cause lymphangitis and resultant lymphedema. In one reported case, a patient with herpetic whitlow presented with acquired lymphedema of the hand. [32]
The peptide adrenomedullin (AM) is encoded by the ADM gene. One report sought to determine if a deficiency in AM predisposes to secondary lymphedema. [33] Endogenous AM was determined to play an important role in secondary lymphedema pathogenesis.
Another interesting report [34] notes a 75-year-old woman with a monoclonal gammopathy of uncertain significance (MGUS) and rapidly progressive lipolymphedema. The researchers speculated that MGUS and lymphedema might be due to initial fibrogenesis worsening preexisting lipedema.
Anatomy
Before embarking on the treatment of lymphedema, a thorough knowledge of the relevant anatomy is essential. Blind-ended lymphatic capillaries arise within the interstitial spaces of the dermal papillae. These unvalved, superficial dermal lymphatics drain into interconnected subdermal channels, which parallel the superficial venous system. These subsequently drain into the deeper, epifascial system of valved trunks lined with smooth muscle cells and located just above the deep fascia of the extremity.
This system is responsible for the drainage of lymph from the skin and subcutaneous tissues. Valves provide for unidirectional flow towards regional lymph nodes and eventually the venous circulation in the neck. Flow is achieved by variations of tissue pressure through skeletal muscle contractions, pulsatile blood flow, and contractions of the spiral smooth muscle fibers surrounding larger lymphatic channels. (See the images below.)
A deeper-valved subfascial system of lymphatics is responsible for the drainage of lymph from the fascia, muscles, joints, ligaments, periosteum, and bone. This subfascial system parallels the deep venous system of the extremity.
The epifascial and subfascial systems normally function independently, although valved connections do exist in the popliteal, inguinal, antecubital, and axillary regions where lymph nodes form interconnected chains. These connections probably do not function under normal conditions; however, in lymphedema, some reversed flow through perforators from the epifascial to the subfascial system may occur as a mechanism of decompression of the epifascial system.
However, the derangement in lymphedema is almost always exclusive to the epifascial lymphatic system, with the subfascial system being uninvolved. Thus, the surgical approaches to lymphedema focus on the epifascial system.
Epidemiology
Occurrence in the United States
In the United States, lymphedema most often occurs after breast cancer surgery, especially in patients who, after undergoing axillary lymphadenectomy, receive radiation therapy. Within this population, 10-40% develop some degree of ipsilateral upper extremity lymphedema. [12, 35]
Although not reported as often as postmastectomy-induced lymphedema, obesity is also one of the most common causes of lymphedema seen in practice today.
The primary lymphedemas occur in 1 of 10,000 individuals, with lymphedema praecox accounting for 80% of cases. The incidence of congenital lymphedema is unknown because most patients have been reported in small, case-based studies.
International occurrence
Worldwide, the most common cause of lymphedema is filariasis infection. More than 100 million people are affected in endemic areas worldwide. [12, 36]
Sex-related demographics
Primary lymphedema occurs most often in females. Lymphedema praecox, the most common primary form, affects 1 in 100,000 females and 1 in 400,000 males. Similarly, females account for 70-80% of cases of congenital lymphedema.
Age-related demographics
Secondary lymphedema can affect persons of any age group, with the onset being determined by the disease’s primary cause. [37] Hereditary (primary) lymphedema can be divided into 3 groups based on the age of onset of clinical lymphedema, as follows:
-
Congenital lymphedema - Usually manifests from birth to age 1 year
-
Lymphedema praecox - Occurs between the ages of 1 and 35 years; it most commonly occurs in adolescents
-
Lymphedema tarda - Manifests after age 35 years
Prognosis
The outcome for persons with lymphedema depends on its chronicity, the complications that result, and the underlying disease state that caused the lymphedema. (Primary lymphedema usually does not progress, with the condition stabilizing after several years of activity.)
Patients with chronic lymphedema for 10 years have a 10% risk of developing lymphangiosarcoma, the most dreaded complication of this disease. Patients with this tumor commonly present with a reddish purple discoloration or nodule that tends to form satellite lesions. It may be confused with Kaposi sarcoma or traumatic ecchymosis. This tumor is highly aggressive, requires radical amputation of the involved extremity, and has a very poor prognosis. [38, 39, 40, 41, 42, 43, 44]
The 5-year survival rate for lymphangiosarcoma is less than 10%, with the average survival following diagnosis being 19 months. This malignant degeneration is most commonly observed in patients with postmastectomy lymphedema (Stewart-Treves syndrome), in whom the incidence is estimated to be 0.5%. [45]
Other neoplasms identified in areas of chronic lymphedema are squamous cell carcinoma, Kaposi sarcoma, [43, 46] B-cell lymphoma, [47] and malignant fibrous histiocytoma.
Complications of lymphedema also include recurrent bouts of cellulitis and/or lymphangitis, bacterial and fungal infections, lymphangio-adenitis, deep venous thrombosis, severe functional impairment, cosmetic embarrassment, and necessary amputation. Some patients may develop protein-losing enteropathy and visceral involvement. Chylous ascites and chylothorax can develop but are rare. Amyloidosis has been described as a complication of primary lymphedema. [48, 49]
Complications following surgery are common and include partial wound separation, seroma, hematoma, skin necrosis, and exacerbation of foot or hand edema.
-
Lymphedema in a patient with hypertension, diabetes, and impaired cardiac function.
-
Morbidly obese patient with lymphedema.
-
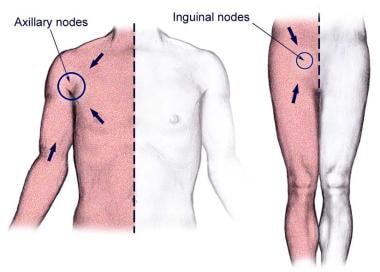
The body quadrants of superficial lymph drainage.
-
(1) Normal lymphatic flow in (a) deep systems and (b) superficial systems. Note the small collateral vessels interconnecting the 2 systems. (2) Lymphedema develops from obstruction, dilation of valves, valvular insufficiency, and subsequent reversal of lymphatic flow.
-
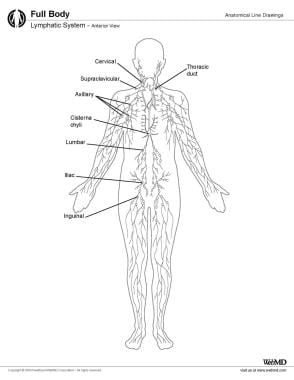
Lymphatic system, anterior view.







