Practice Essentials
Of the approximately 80,620 cases of non-Hodgkin lymphoma (NHL) expected to be diagnosed in 2024 in the United States, [1] approximately 20% are likely to be follicular lymphomas. [2] No sex preponderance is seen for follicular lymphomas, but the incidence increases with age and varies across racial groups. See the image below.
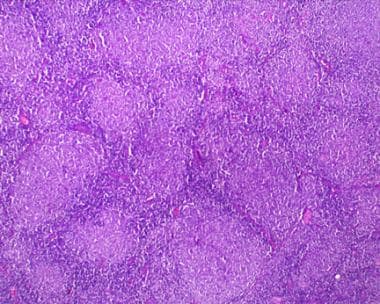 Follicular lymphoma, low-power view. Note the nodular pattern reminiscent of germinal centers. Photograph courtesy of Aamir Ehsan, MD.
Follicular lymphoma, low-power view. Note the nodular pattern reminiscent of germinal centers. Photograph courtesy of Aamir Ehsan, MD.
Signs and symptoms
Follicular lymphoma is a type of non-Hodgkin lymphoma that is often asymptomatic and indolent. It most commonly presents as a painless, slowly progressive adenopathy. Systemic symptoms, such as fever, drenching night sweats, or weight loss in excess of 10% of ideal body weight, or asthenia, are infrequent at presentation but can be observed in later stages of the disease.
Symptoms related to bone marrow dysfunction, such as anemia, leukopenia, or thrombocytopenia, are rare at presentation but can also be observed in the later stages of the disease. Lymphocytosis, reflecting blood involvement, may also be present.
Despite the fact that most follicular lymphomas are advanced at the time of diagnosis, many patients may not require treatment for prolonged periods of time, and the median survival of patients with follicular lymphomas has historically been approximately 8-10 years. [2] Literature since the rituximab era has shown a further increase in overall survival. [3, 4]
Diagnosis
During the physical evaluation, all lymph node areas and the reticuloendothelial system should be examined. Involved nodes typically are nontender, firm, and rubbery in consistency. The throat, liver, and spleen should also be examined. Splenomegaly is present in approximately 50% of patients at presentation, and hepatosplenomegaly may occur.
A complete blood cell count (CBC) with differential should be obtained, including examination of the peripheral blood smear if the differential is abnormal. A chemistry panel and lactate dehydrogenase (LDH) level should be obtained.
A CT scan of the chest, abdomen, and pelvis can determine whether abdominal or pelvic adenopathy is present. Positron emission tomography (PET) scanning may also be useful in certain clinical settings, such as localized disease or when transformed disease is suspected. [5]
Biopsy is essential to establish a diagnosis of lymphoma. Obtain an excisional biopsy (or, if that is not possible, a core biopsy) of an involved node. If the disease is extranodal, a surgical biopsy sample should be obtained from the involved organ.
Because the chromosomal t(14;18) translocation is found in the majority of patients with follicular lymphoma, bone marrow aspiration and chromosome analysis can also help establish the diagnosis.
Staging and grading
Most patients with follicular lymphoma present at an advanced stage, and most patients have bone marrow involvement at diagnosis. Staging is as follows:
-
Stage I – One involved lymph node or lymph node area
-
Stage II – Two or more involved lymph nodes or lymph node areas on the same side of diaphragm
-
Stage III – Involved lymph node or lymph node areas on both sides of diaphragm
-
Stage IV – Disseminated disease, such as bone marrow, liver, or central nervous system involvement
Management
Treatment varies based on the stage of the disease. Early-stage, localized disease may be treated with radiation therapy or excision in certain cases. Observation is recommended for patients with advanced disease until they develop systemic symptoms or disease that threatens organ function.
Multiagent chemotherapy in combination with rituximab is the most common first-line treatment strategy for follicular lymphoma. Combination chemotherapy regimens vary and include the following:
-
Rituximab, cyclophosphamide, vincristine, prednisone (R-CVP) [6]
-
Rituximab, cyclophosphamide, doxorubicin, vincristine, prednisone (R-CHOP) [7]
-
CHOP immediately followed by tositumomab/iodine-131 radioimmunotherapy (CHOP-RIT) [8]
-
Bendamustine plus rituximab [9]
Single agents tend to be less effective than combination chemotherapy, but are appropriate for selected patients because they may be simpler to administer, induce less toxicity, and palliate symptoms. Single agents include the following:
-
Chlorambucil
-
Fludarabine
-
Bendamustine
-
Rituximab
-
Tazemetostat
-
Pi3K inhibitors (idelalisib, copanlisib, duvelisib)
-
Mosunetuzumab
-
Dual inhibitor of PI3K and casein kinase epsilon (umbralisib)
Etiology and Pathophysiology
The t(14;18) chromosomal translocation is both a genetic hallmark of follicular lymphoma and critical early event in its development. The translocation results in deregulation of the bcl2 proto-oncogene, which confers a survival advantage to the affected cells by preventing apoptotic death. By itself, t(14;18) does not account for the development of follicular lymphoma—t(14;18)-positive cells can be found in healthy individuals—but high t(14;18) frequency in blood appears to be a predictive biomarker for follicular lymphoma, occurring years before diagnosis. [12] .
Viruses and chemicals
Viruses have been implicated as etiologic factors for lymphomas, including the Epstein-Barr virus (EBV), human T-cell lymphotropic virus (HTLV) type I, and the herpesvirus associated with Kaposi sarcoma (ie, human herpesvirus [HHV]-8 ). Hepatitis B and C viruses are also associated with risk for lymphoma. Nevertheless, these viruses have been linked mostly to diffuse or high-grade lymphomas.
Chemicals, such as defoliants (eg, Agent Orange) and hair dyes, have been associated with lymphoma.
Immunodeficiency states
Congenital immunodeficiencies have been associated with lymphoma. Acquired immunodeficiencies may include infection with the human immunodeficiency virus (HIV). Most lymphomas associated with HIV are intermediate-grade or high-grade lymphomas.
Patients who have been on immunosuppressant drugs after organ transplantation may develop lymphoma. Most of these lymphomas are diffuse or high-grade lymphomas.
Autoimmune diseases and the treatments for them (eg, methotrexate) that may allow lymphomagenesis are known to be associated with an increased risk of lymphoma. [13]
Epidemiology
In the United States, non-Hodgkin lymphoma (NHL) is the seventh most frequently diagnosed malignancy in men and the sixth most common in women. The American Cancer Society estimates that 80,620 cases of NHL will be diagnosed in 2024. [1] Follicular lymphomas constitute approximately 20% of NHLs. [2] No sex preponderance is seen.
In general, age-adjusted incidence rates of NHL are higher in more developed countries. The incidence of follicular lymphoma, like that of other NHLs, increases with age; these conditions are extremely rare in children, though the World Health Organization has delineated a pediatric variant. The median age at diagnosis is 65-74 years. [14] The age-adjusted incidence rates of NHL varied from 3.7-14 cases per 100,000 person years from 1983-1987 in different countries.
Variations in racial incidence are found throughout the world. The incidence of follicular lymphomas is low in China and Japan, but people of Ashkenazi Jewish ancestry have a higher incidence of lymphoma. In the United States, the incidence is 2-3 times higher in Whites than in Blacks. [15]
Clinical Evaluation
Follicular lymphoma most commonly presents as a painless, slowly progressive adenopathy. Some patients have waxing and waning adenopathy.
Systemic symptoms, such as fever, drenching night sweats, and/or weight loss in excess of 10% of ideal body weight, are infrequent at presentation but can be observed in later stages of the disease. Transformation to an intermediate-grade or high-grade lymphoma should be considered when a patient develops systemic symptoms or rapid enlargement of a lymph node.
Symptoms related to bone marrow dysfunction, such as anemia, leukopenia, or thrombocytopenia, are rare at presentation but can also be observed in the later stages of the disease.
During the physical evaluation, all lymph node areas and the reticuloendothelial system should be examined, including the pre- and post-auricular, submandibular, cervical, supraclavicular, axillary, epitrochlear, inguinal, and popliteal areas. Involved nodes typically are nontender, firm, and rubbery in consistency.
In addition, the throat should be examined for involvement of the oropharyngeal lymphoid tissue (ie, Waldeyer ring), and particular attention should be given to the abdominal examination (eg, liver and spleen), as splenomegaly is present in approximately 50% of patients at presentation and hepatosplenomegaly may occur.
Most lymphomas originate from lymph node tissue and can frequently involve other organs. Lymphomas can involve any organ, including the skin and GI tract, and they can cause detrimental effects by organ invasion and by obstruction of anatomic structures by a tumoral mass. [16, 17] For example, ureteral obstruction by enlarged lymph nodes can lead to renal failure.
Staging
Most patients with follicular lymphoma present at an advanced stage, and most patients have bone marrow involvement at diagnosis. Staging is as follows:
-
Stage I - One involved lymph node or lymph node area
-
Stage II - Two or more involved lymph nodes or lymph node areas on the same side of diaphragm
-
Stage III - Involved lymph node or lymph node areas on both sides of diaphragm
-
Stage IV - Disseminated disease, such as bone marrow, liver, or central nervous system (CNS) involvement
See also Pathologic classification systems under Histologic Findings and Follicular Lymphoma (Non-Hodgkin Lymphoma) Staging
Differential Diagnosis
Autoimmune disorders and chronic infections as well as the following conditions should be evaluated as part of the differential diagnosis of follicular lymphomas:
-
Lymphoplasmacytic lymphoma (eg, Waldenström macroglobulinemia)
Routine Laboratory Tests
A complete blood cell count (CBC) and differential should be obtained, along with examination of the peripheral blood smear if the differential is abnormal. Frequently, abnormal lymphocytes can be identified in the blood smear, reflecting involvement of the blood
Blood chemistries, including lactate dehydrogenase (LDH) levels, uric acid levels, liver function tests, and creatinine measurements should be assessed. LDH is an indicator of tumor load, and an elevated level is a negative prognostic factor.
Hyperuricemia may be observed upon presentation or during therapy. Allopurinol should be considered in patients with hyperuricemia and before treatment to prevent uric acid nephropathy.
Increased creatinine levels can be observed in patients with renal obstruction caused by lymphadenopathy, and increased alkaline phosphatase and bilirubin measurements can be observed in patients with biliary obstruction due to lymphadenopathy or involvement of the liver.
If treatment with rituximab is being considered, serology for hepatitis B (ie, hepatitis B surface antigen, core antibody, and surface antibody) and hepatitis C should be obtained. Rituximab carries a black box warning for reactivation of hepatitis B infection, including fatal cases. Data regarding rituximab-induced hepatitis C reactivation are controversial, but life-threatening hepatic flares are a possibility, especially in patients with active hepatitis or cirrhosis, and in those treated with regimens containing rituximab and chemotherapy that includes corticosteroids. [18]
CT and PET Scanning
CT scans of the chest, abdomen, and pelvis should be performed to determine whether adenopathy is present. CT scans allow visualization of the kidneys, ureters, and the hepatobiliary system. In some cases, those organs are affected by obstruction due to lymphadenopathy or by parenchymal involvement with lymphoma.
Positron emission tomography (PET) scanning complements standard radiologic testing, but only a minority of patients will be diagnosed with a higher stage of disease. This imaging modality can distinguish between viable tumor and fibrosis in patients with residual lymphadenopathy after therapy, but because the majority of follicular lymphoma cases are not curable, such a finding may not change management. [5] This is in contrast to Hodgkin lymphoma and intermediate-grade lymphoma, in which a positive PET scan might prompt salvage chemotherapy or radiation because the treatment goal in those diseases is cure.
Biopsies
The role of the surgeon is to obtain an excisional biopsy adequate to establish the diagnosis. The surgeon should be instructed about the proper handling of the specimen and the special tests that may be required. A discussion of these issues with the pathologist before the biopsy is performed is often helpful.
Pathologic diagnosis from biopsy specimen
Biopsy is essential to establish a diagnosis of lymphoma. Obtain an excisional biopsy of an involved node. Note that a needle aspiration is not adequate for the initial diagnosis of lymphoma. [19] If the disease is extranodal, a surgical biopsy sample should be obtained from the involved organ. If an excisional or incisional biopsy cannot be obtained because of location, a core biopsy may be acceptable.
Posterior iliac crest bone marrow aspiration and biopsies
Although a diagnosis of follicular lymphoma can be established based on histologic findings from lymph nodes and involvement of the bone marrow can be diagnosed using morphologic criteria, cytogenetic analysis of bone marrow cells should be performed because the t(14;18) chromosomal translocation is found in the majority of patients with follicular lymphoma and can help establish the diagnosis. Fluorescence in situ hybridization (FISH) testing for a t(14;18) chromosomal translocation may also be useful.
Immunophenotyping
National Comprehensive Cancer Network (NCCN) guidelines consider immunophenotyping essential for establishing the diagnosis of follicular lymphoma. [20] The immunohistochemistry (IHC) panel should include the following:
-
CD20
-
CD3
-
CD5
-
CD10
-
BCL2
-
BCL6
-
CD21 or CD23
The IHC panel may be performed with or without cell surface marker analysis of the following by flow cytometry with a peripheral blood and/or biopsy specimen:
-
Kappa/lambda
-
CD19
-
CD20
-
CD5
-
CD23
-
CD10
The typical immunophenotype of follicular lymphoma is as follows:
-
CD10+
-
BCL2+
-
CD23+/-
-
CD43-
-
CD5-
-
CD20+
-
BCL6+
-
Rare cases of follicular lymphoma may be CD10- or BCL2-
In certain circumstances, the following studies may be useful [20] :
-
Molecular analysis to detect antigen receptor gene rearrangements; BCL2 rearrangements
-
Karyotype or FISH: t(14;18); BCL6, 1p36, IRF4/MUM1 rearrangements
-
IHC panel: Ki-67g; IRF4/MUM1 for FL grade 3, cyclin D1
-
Next-generation sequencing panel including TNFRSF14 and STAT6 mutation
Acquired nonrandom chromosomal translocations
The most common acquired nonrandom chromosomal translocation in patients with follicular lymphomas is the t(14;18) translocation, which is found in more than 80% of cases. [21] This chromosomal translocation brings the bcl2 proto-oncogene under the transcriptional influence of the immunoglobulin heavy-chain gene, leading to the overexpression of a functionally normal bcl-2 protein. Overexpression of the bcl-2 protein, a protein of the mitochondrial membrane, confers a survival advantage to the cancer cells by inhibiting programmed cell death (apoptosis). Although the exact mechanism of action of bcl-2 is unclear, its interaction with other homologues is felt to determine the likelihood of a cell undergoing apoptosis.
The detection of the t(14;18) product by polymerase chain reaction (PCR) is used frequently in the diagnosis and follow-up of patients with follicular lymphomas. Nevertheless, this translocation has been detected in healthy patients and in patients with other types of tumors.
Histologic Findings
The most common diagnostic pitfall is to confuse follicular lymphomas with other types of lymphomas. The diagnosis of lymphomas is complex, and tissue biopsies should be reviewed by pathologists with experience in interpreting lymph node biopsies and other diagnostic material.
Follicular lymphomas exhibit a follicular or nodular pattern of growth reminiscent of germinal centers. This follicular pattern of growth contrasts with diffuse lymphomas, which usually are intermediate or high-grade neoplasms (see the following images).
Follicular lymphoma, low-power view. Note the nodular pattern reminiscent of germinal centers. Photograph courtesy of Aamir Ehsan, MD.
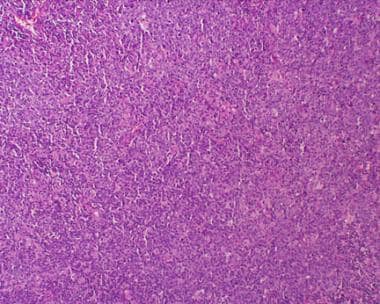
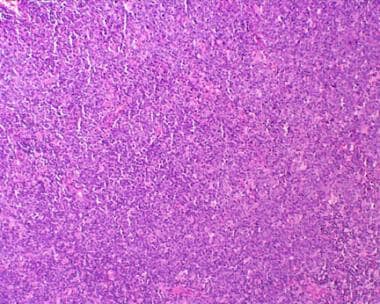 Diffuse lymphoma. Note the absence of the nodular pattern observed in follicular lymphomas. Photograph courtesy of Aamir Ehsan, MD.
Diffuse lymphoma. Note the absence of the nodular pattern observed in follicular lymphomas. Photograph courtesy of Aamir Ehsan, MD.
Pathologic classification systems
Several pathologic classification systems have been used since the late 1960s, including the following:
-
Rappaport
-
Lukes-Collins
-
Kiel
-
National Cancer Institute Working Formulation [22]
-
Revised European-American Classification of Lymphoid Neoplasms (REAL) [23]
-
World Health Organization (WHO)
Early classification systems relied solely on the architecture and cytologic appearance of lymph nodes. As more sophisticated tests became available, immunophenotypic, cytogenetic, and molecular criteria were incorporated in the diagnosis of lymphomas.
The Working Formulation, originally proposed in 1982, combined results from six major classification systems and grouped lymphomas by morphology and clinical behavior into, low, intermediate, or high grade, with 10 subgroups labeled A to J. [22] With advances in immunologic and genetic techniques, the Working Formulation became obsolete, but it is still used for historical data comparisons. [22]
In 1994, the REAL classification attempted to apply immunophenotypic and genetic features in identifying distinct clinicopathologic NHL entities. [23] REAL was based on the premise that a classification should attempt to define disease entities using all available information, including morphology characteristics and immunophenotypic, genetic, and clinical features.
The WHO classification, introduced in 2001 and updated in 2008, 2016, and 2022, further elaborated upon the REAL approach. This classification divides NHL into two groups: those of B-cell origin and those of T-cell/natural killer (NK)–cell origin. [24, 25]
Prior versions of the WHO classification divided follicular lymphoma into grades 1-3, based on the number of centroblasts per high-power field (hpf), as follows [26] :
-
Grade 1: 0-5 centroblasts per hpf
-
Grade 2: 6-15 centroblasts per hpf
-
Grade 3: > 15 centroblasts per hpf
Grade 3 disease is subdivided into grade 3A, in which centrocytes are present,and grade 3B, in which folllicles composed of centrocytes are present.
In the current version (5th edition), grading of follicular lymphoma is considered optional, as it has shown poor reproducibility and questionable clinical significance; outcomes among patients with grades 1, 2, and 3A follicular lymphoma do not appear to be significantly different. Instead, grades 1, 2 and 3A are termed classic follicular lymphoma. [25]
The 5th edition classifies FL as follows:
-
In situ follicular B-cell neoplasm (previously called in situ follicular neoplasia)
-
Follicular lymphoma
-
Pediatric-type follicular lymphoma
-
Duodenal-type follicular lymphoma
The term in situ follicular neoplasm reflects the low risk of progression to lymphoma in these cases. Pediatric-type FL is a localized clonal proliferation characterized by large, expansile, highly proliferative follicles that often have prominent blastoid follicular center cells rather than classic centroblasts (or centrocytes); BCL2 rearrangements must not be present, but there may be some BCL2 protein expression. It is termed pediatric-type because cases may rarely occur in older individuals. Pediatric-type FL carries an excellent prognosis; a conservative therapeutic approach may be sufficient. [24]
The intestines, especially the duodenum, are a frequent site of extranodal follicular lymphoma. These cases are frequently found in the second part of the duodenum as polyps. Survival appears to be excellent even without treatment. However, 85% of duodenal lymphomas can spread to the jejunum and ileum. [27]
The International Consensus Classification (ICC) has retained the grading for follicular lymphoma (ie, 1-2, 3A and 3B). [28] ICC grades 1–2 are managed according to the treatment recommendations for classic follicular lymphoma, while grade 3B (follicular large B-cell lymphoma) is commonly treated as diffuse large B-cell lymphoma (DLBCL). Follicular lymphoma of any grade that contains any area of DLBCL should be diagnosed and treated as a DLBCL. National Comprehensive Cancer Network (NCCN) guidelines note that grade 3 follicular lymphoma is an area of controversy, with some experts treating grade 3A as follicular lymphoma and others treating it as DLBCL. [20]
Importantly, progression to diffuse large-cell lymphoma occurs in 10-50% of patients, depending on the duration of disease presence. Transformation to diffuse large-cell lymphoma frequently is associated with rapid progression of the disease, including increasing adenopathy, development of systemic symptoms, and infiltration of extranodal sites.
Progression to large-cell lymphoma can be a poor prognostic factor. Many patients who experience transformation succumb to the disease, especially those who have received many lines of previous therapy. See the following image.
 A patient with follicular lymphoma who was diagnosed 6 years earlier presents to his hematologist's office because of rapidly growing lymphadenopathy and onset of fever, severe night sweats, and weight loss. In the past, he had been treated with chlorambucil and prednisone when his submandibular lymph nodes became large enough to make him uncomfortable. This treatment had worked well, and he has not required any treatment recently. A biopsy of an involved lymph node is obtained. The diagnosis is transformation to diffuse non-Hodgkin lymphoma.
A patient with follicular lymphoma who was diagnosed 6 years earlier presents to his hematologist's office because of rapidly growing lymphadenopathy and onset of fever, severe night sweats, and weight loss. In the past, he had been treated with chlorambucil and prednisone when his submandibular lymph nodes became large enough to make him uncomfortable. This treatment had worked well, and he has not required any treatment recently. A biopsy of an involved lymph node is obtained. The diagnosis is transformation to diffuse non-Hodgkin lymphoma.
Xerri et al have demonstrated that high levels of MUM1 positivity are associated with shorter progression-free survival, based on analysis of the patient samples from the PRIMA study and correlating the patient outcomes. [29] Another study of 46 cases of follicular lymphoma was also able to correlate high levels of MUM1 expression with high-grade subtype and poorer outcome because of the propensity for transformation. [30]
Management Overview
Most patients with follicular lymphoma do not require hospitalization during the early stages of the disease. However, patients with bulky disease at the time of treatment should be followed closely for tumor lysis syndrome. Allopurinol should be considered in these patients.
Physicians who have training and/or experience in antineoplastic agents should be the ones to order the following:
-
Alkylating agents (eg, bendamustine, chlorambucil, cyclophosphamide): These agents inhibit cell growth and proliferation. [31]
-
Antimetabolites (eg, fludarabine): These agents interfere with metabolic pathways necessary for the survival of target cells.
-
Anthracyclines (eg, doxorubicin, mitoxantrone): These drugs inhibit DNA synthesis.
-
Vinca alkaloids (eg, vincristine): These drugs inhibit cell growth and proliferation at the mitotic phase of the cell cycle.
-
Corticosteroids (eg, prednisone): These agents have anti-inflammatory effects in many organ system disorders. Corticosteroids are also lympholytic and modify the body's immune responses to diverse stimuli.
-
Monoclonal antibodies (eg, rituximab, obinutuzumab, tositumomab and iodine-131, ibritumomab tiuxetan): These agents bind to target cells and recruit immune-effector functions to mediate target-cell lysis. [32, 31]
-
PI3K Inhibitors (eg, idelalisib, copanlisib, duvelisib, umbralisib): These agents inhibit key cell-signaling pathways, inducing apoptosis and inhibiting proliferation of premalignant B cells
-
EZH2 inhibitors (eg, tazemetostat): These agents prevent and decreases histone methylation which alters gene expression patterns associated with cancer pathways and results in decreased tumor cell proliferation in EZH2-mutated cancer cells
-
Other agents
- Umbralisib - Dual inhibitor of PI3K and casein kinase epsilon
For more information, see Follicular Lymphoma (Non-Hodgkin Lymphoma) Treatment Protocols
Patient education
Patients should be educated regarding the signs and symptoms of progression of the disease, including new systemic symptoms, new lymphadenopathy, or rapidly enlarging lymphadenopathy.
Similar to patients with chronic lymphocytic leukemia, patients with follicular lymphoma also are more prone to infections and should be instructed to contact their physician early if they develop signs or symptoms of infection. Administration of rituximab may lead to hypogammaglobulinemia.
For patient education information, see Lymphoma.
Radiotherapy - Localized Disease
The rare patient who presents with localized disease should be treated with radiation therapy with curative intent; approximately half of these patients will be cured with radiation alone.
Despite guidelines that recommend radiation therapy for stage I follicular lymphoma, other treatment approaches have been used successfully. In a large study of patients with stage I follicular lymphoma, Friedberg et al found that treatment approaches such as rituximab/chemotherapy and systemic therapy plus radiation resulted in similar excellent outcomes. [33] Unfortunately, fewer than 10% of patients with follicular lymphoma present with localized disease.
A retrospective analysis of 120 treatment-naïve, low-tumor-burden patients with follicular lymphoma among more than 1000 patients enrolled in a population-based French registry underwent a watchful waiting strategy. [34] The median time to treatment in this group was 55 months. Their outcome was comparable to 242 patients with similar features receiving frontline rituximab-based therapy. Therefore, low-tumor-burden patients with follicular lymphoma can be managed with a watch-and-wait approach.
Observation - Asymptomatic Advanced Disease
The treatment for advanced stage disease is considered palliative, because most follicular lymphomas are disseminated and incurable at the time of diagnosis. Many experts recommend observation until the patient develops systemic symptoms, such as fever, weight loss, or bulky lymphadenopathy, because early therapy has not been shown to impact overall survival. [35] Patients in whom treatment is deferred should be followed closely for complications such as ureteral or biliary obstruction. No universally accepted first-line treatment strategy exists for stage III/IV follicular lymphoma.
Single-Agent Therapy
Single-agent therapy has been an option for patients with symptomatic disease. [36] Single agents tend to have lower response rates and provide a shorter duration of disease control than do combination chemotherapy regimens. Nonetheless, they are appropriate for selected patients because they may be simpler to administer, induce less toxicity, and palliate symptoms.
Chlorambucil
Chlorambucil is an oral alkylating agent that is often reserved for elderly patients with a poor performance status or those who wish to defer intravenous therapy. Few patients will have a complete response, and there is no impact on overall survival.
Fludarabine
Single-agent fludarabine must be administered intravenously; this agent causes a significant degree of myelosuppression and immunosuppression, and there is also some concern that therapy with fludarabine may impair the ability to collect hematopoietic stem cells for an autologous stem cell transplantation. Fludarabine is associated with higher response rates than single-agent chlorambucil, but it has no impact on overall survival.
Bendamustine
Single-agent bendamustine can be well tolerated, aside from neutropenia and thrombocytopenia. However, as with many other chemotherapy agents, there is a risk of secondary myelodysplastic syndrome (MDS), particularly in patients who will require subsequent chemotherapy.
Rituximab
Rituximab (Rituxan, Truxima), a monoclonal antibody targeting the CD20 antigen expressed on the cell surface of most lymphoma cells, has demonstrated efficacy as a single agent and as part of combination chemotherapy regimens. It is generally well tolerated but is significantly more expensive than most other therapies. Clinical trials using rituximab as maintenance therapy have suggested that this strategy prolonged progression-free survival in patients who had an objective response or stable disease following rituximab monotherapy. [37, 38, 39, 40, 41]
A study by Vidal et al concluded that rituximab maintenance remains the standard of care for refractory or relapsed follicular lymphoma. [42]
Rituximab combined with hyaluronidase human, which increases subcutaneous tissue permeability, was approved by the FDA in 2017. A study by Davies et al concluded that subcutaneous rituximab/hyaluronidase (Rituxan Hycela) can be safely administered with similar efficacy to intravenous rituximab. [43] The study randomized 410 patients to receive rituximab subcutaneously or intravenously. Overall response rates (ORRs) as well as adverse reaction rates were similar in the two arms. The most common grade 3 adverse event was neutropenia.
Rituximab/hyaluronidase indications include the following:
-
Relapsed or refractory follicular lymphoma (FL), as a single agent
-
Previously untreated FL, in combination with first-line chemotherapy
-
In patients achieving a complete or partial response to rituximab in combination with chemotherapy, as single-agent maintenance therapy
-
Nonprogressing FL (eg, stable disease), as a single agent after first-line cyclophosphamide, vincristine, and prednisone (CVP) chemotherapy
All patients must receive at least one full dose of rituximab IV infusion before starting rituximab/hyaluronidase.
Tazemetostat
Tazemetostat is an inhibitor of the methyltransferase EZH2, and of some EZH2 gain-of-function mutations including Y646X, A682G, and A692V. It suppresses proliferation of B-cell lymphoma cell lines in vitro and demonstrates greater effect on the inhibition of proliferation of lymphoma cell lines with mutant EZH2.
In 2020, the FDA granted accelerated approval to tazemetostat (Tazverik), an EZH2 inhibitor, for adults with relapsed or refractory FL whose tumors are positive for an EZH2 mutation and who have received at least two prior systemic therapies, and for adults with relapsed/refractory FL who have no satisfactory alternative treatment options.
Approval was based on two open-label, single-arm cohorts of a multicenter trial in patients with histologically confirmed FL after at least two prior systemic therapies. Patients received tazemetostat 800 mg PO BID until confirmed disease progression or unacceptable toxicity. ORR in 42 patients with EZH2-mutant FL was 69%, with 12% complete responses and 57% partial responses. Median duration of response in these patients was 10.9 months. The ORR in 53 patients with EZH2 wild-type FL was 34%, with 4% complete responses and 30% partial responses. Median duration of response was 13 months. [44]
Idelalisib
Idelalisib (Zydelig), an oral phosphoinositide 3-kinase (PI3K) delta inhibitor, received accelerated approval from the FDA in 2014 for relapsed follicular B-cell NHL in patients who have received at least two prior systemic therapies. The accelerated approval was based on a phase 2 open-label study involving 125 patients with indolent non-Hodgkin lymphomas that had not responded to treatment with rituximab and an alkylating agent or had relapsed within 6 months afterward. [45]
The response rate was 57% (71 of 125 patients), with 6% meeting the criteria for a complete response. The median time to a response was 1.9 months, the median duration of response was 12.5 months, and the median progression-free survival was 11 months. Similar response rates were observed across all subtypes of indolent NHL. [35]
Possible adverse effects of idelalisib include pneumonitis, diarrhea from colitis, hepatitis, and neutropenia. Several studies with idelalisib were halted due to toxicities related to development of Pneumocystis jiroveci pneumonia (PJP) and reactivation of cytomegalovirus (CMV) infection. Therefore, PJP prophylaxis is strongly recommended.
Copanlisib
Copanlisib, a pan-PI3k inhibitor, received FDA approval for FL that has failed to respond to two prior therapies. Unlike idelalisib, copanlisib is given intravenously. Approval was based on a phase 2 trial in 142 patients with FL in whom two prior lines of therapy had failed. [46] The objective response rate was 59%, with 12% complete responses. The median duration of response was 22.6 months. The median progression-free survival was 11.2 months, with the median overall survival not yet reached. The adverse effects of the drug include transient hyperglycemia, transient hypertension, neutropenia, and lung infection.
Duvelisib
Duvelisib is a selective oral small molecule inhibitor of PI3K-delta and PI3K-gamma. Inhibiting PI3K induces growth inhibition and reduces viability in cell lines derived from malignant B cells. It is indicated for adults with relapsed/refractory follicular cell lymphoma after at least two prior systemic therapies. Approval resulted from results of a phase 2 trial. At 18-month follow-up of the 83 patients enrolled, 36 had responded, which included 1 (1%) complete response and 35 (42%) partial responses, for an ORR of 43%; 83% of evaluable patients with FL treated with duvelisib had a reduction in the size of their target lymph nodes. [47]
Mosunetuzumab
Mosunetuzumab is a bispecific T-cell engaging antibody that binds to the CD3 receptor expressed on the surface of T-cells and CD20 expressed on the surface of lymphoma cells. It gained accelerated approval from the FDA in 2022 for relapsed or refractory follicular lymphoma after at least two lines of systemic therapy.
Approval was based on the phase 2 GO29781 study. After more than 2 years of follow-up, the ORR was 78%, the complete response rate was 60%, the 24-month duration of response rate was 53%, and the 24-month duration rate of complete response was 63%. Median progression-free survival and overall survival were 24 months. The 2-year progression-free survival and overall survival rates were 48% and 87%, respectively. [48]
Umbralisib
Umbralisib is a dual inhibitor of PI3K-delta and casein kinase (CK1) 1-epsilon expressed on malignant B cells. It was granted accelerated approval for relapsed or refractory FL in adults who received at least three prior systemic therapies. Approval was based on a multicenter, open-label trial in 117 patients with relapsed or refractory FL after two prior systemic therapies. Efficacy was based on ORR and duration of response assessed by an independent review committee. The ORR was 43% (95% CI: 33.6-52.2) with 3.4% of patients achieving complete responses and 39% achieving partial response. Median duration of response was 11.1 months (95% CI: 8.3-16.4). [49]
Multiagent Chemotherapy
Combining multiagent chemotherapy and rituximab is the most common first-line treatment strategy in the United States. Several studies have compared combination chemotherapy with and without rituximab; the rituximab-containing regimens generally produce a higher response rate and a more durable response. A meta-analysis confirmed an improvement in overall survival in patients with follicular lymphoma associated with the addition of rituximab to combination chemotherapy regimens. [50] Relapse of follicular lymphoma within 24 months following rituximab-containing chemotherapy is associated with poor outcome, including high risk for death. [51]
Rituximab-containing regimens
Combination chemotherapy regimens vary and include the following:
-
Rituximab, cyclophosphamide, vincristine, prednisone (R-CVP) [6]
-
Rituximab, cyclophosphamide, doxorubicin, vincristine, prednisone (R-CHOP) [7]
-
Fludarabine, cyclophosphamide, rituximab (FCR)
-
Rituximab, fludarabine, cyclophosphamide, mitoxantrone (R-FCM)
-
Fludarabine, rituximab (FR)
-
Bendamustine, rituximab (BR)
-
Lenalidomide (Revlimid), rituximab (R2, R-squared)
Rituximab has been evaluated as maintenance chemotherapy in patients with follicular lymphoma after initial chemotherapy. In a large European study, rituximab given every 2 months for 2 years increased disease-free survival, but not overall survival. [52]
In a retrospective analysis of 356 patients with treatment-naïve, advanced-stage, grade 1-2 follicular lymphoma, the 3-year progression-free survival rates with different regimens were as follows [53] :
-
R-CHOP: 60%
-
R-CHOP with maintenance rituximab: 72%
-
Bendamustine/rituximab: 63%
-
Bendamustine/rituximab with maintenance rituximab: 97%
-
R 2 (rituximab plus lenalidomide [Revlimid]): 87%
A study by Fowler et al also investigated the combination of rituximab with lenalidomide in 110 patients with previously untreated indolent lymphoma. [10] Of the 110 patients studied, 50 patients had follicular lymphoma. The complete response rate was 87% and 11% had partial response. The RELEVANCE trial is an ongoing randomized study examining the role of R2 in comparison with rituximab plus chemotherapy as frontline therapy for follicular lymphoma. On interim analysis, R2 was found to have similar efficacy to rituximab plus chemotherapy. The two regimens had different safety profiles, with more grade 3/4 neutropenia in the rituximab-chemotherapy arm than in the R2 arm (50% versus 32%, respectively). [54] These results offer the encouraging prospect of having a non-chemotherapeutic alternative for these patients.
In 2019, the FDA approved lenalidomide in combination with a rituximab product for the treatment of previously treated follicular lymphoma or marginal zone lymphoma—the first nonchemotherapeutic regimen approved for this indication. Approval was based on the AUGMENT study, in which the objective response was 80% in the lenalidomide plus rituximab arm compared with 55% in the control arm, and median progression-free survival rates were 39.4 months versus 14.1 months, respectively. [11] In 2020, the National Institute for Health and Care Excellence (NICE) in the United Kingdom approved lenalidomide in combination with rituximab as an option for previously treated follicular lymphoma in adults. [55]
Obinutuzumab
Obinutuzumab (Gazyva) is a monoclonal antibody that targets the CD20 antigen expressed on the surface of pre B- and mature B-lymphocytes. In 2016, the FDA approved obinutuzumab for follicular lymphoma that is refractory to, or has relapsed after, a rituximab-containing regimen. Approval was based on the phase 3 GADOLIN study (n=396) comparing obinutuzumab plus bendamustine with bendamustine alone. On interim analysis, median progression-free survival was 14 months for bendamustine alone and 29 months for obinutuzumab plus bendamustine (P < 0.0001). [31]
Obinutuzumab is administered with bendamustine for six 28-day cycles, as follows:
-
Cycle 1: Obinutuzumab 1000 mg IV on days 1, 8, and 15 plus bendamustine 90 mg/m 2/day IV on days 1 and 2
-
Cycles 2-6: Obinutuzumab 1000 mg IV on day 1 plus bendamustine 90 mg/m 2/day IV on days 1 and 2
-
Monotherapy: Patients who achieve stable disease, complete response, or partial response to the first 6 cycles should continue on obinutuzumab 1000 mg IV every 2 months for 2 years.
Obinutuzumab plus chemotherapy with obinutuzumab maintenance was compared with rituximab plus chemotherapy with rituximab maintenance in 1202 patients with previously untreated advanced-stage follicular lymphoma (either bulky stage II or stage III or IV). [56] In this study, The progression-free survival at 3 years was 80% in the obinutuzumab-containing arm versus 73.3% in the rituximab-containing arm. The hazard ratio of progression, death, or relapse was 0.66. However, the rate of infusion-related reactions was higher in the obinutuzumab arm. The combination of obintuzumab with chemotherapy was approved by FDA in 2017.
Hematopoietic Stem Cell Transplantation
Hematopoietic stem cell transplantation (HSCT) has a role in the treatment of follicular lymphoma, especially in younger patients with relapsed or recurrent disease. [57] HSCT is generally reserved for patients with relapsed or refractory disease.
Allogeneic HSCT can induce long-term remissions in patients with follicular lymphoma, but transplant-related mortality is high. [58] Autologous HSCT has a low transplant-associated mortality and prolongs progression-free survival; in a randomized, controlled trial, improvement in overall patient survival was observed. [59] However, most patients eventually relapse after undergoing this therapy, and there is an increased rate of secondary malignancies.
A study by Al Khabori et al determined that available evidence indicates autologous transplantation in first remission is not indicated; however, the best time for transplantation is unclear. [60] Lunning et al compared outcomes in 44 patients with relapsed and refractory follicular lymphoma who underwent either autologous or allogeneic HSCT, and found that in patients whose remission had lasted for 12 months or less, event-free survival at 3 years was significantly greater with allogeneic versus autologous HSCT (80% versus 42%, respectively; P < 0.015). [61]
Targeted Radioimmunotherapy
Follicular lymphoma is inherently radiosensitive, so the development of targeted radioimmunotherapy [62] to the CD20 marker expressed on B cells has been a significant advance. {ref51This technique enables the delivery of cytocidal doses of radiation to all sites of disseminated disease. Two agents are available for this type of treatment: iodine-131 (131I)–labeled tositumomab (Bexxar) and yttrium-90 (90Y)–labeled ibritumomab tiuxetan (Zevalin). [63] Both agents have produced high response rates in patients with relapsed or refractory and treatment-naive follicular lymphoma. [64, 65, 66]
Initial studies of 131I–labeled tositumomab and 90Y–labeled ibritumomab tiuxetan demonstrated improvements in progression-free survival but not in overall patient survival.
The use of radioimmunoconjugate agents is limited in the United States by the need for highly trained staff and specialized equipment, the expense of therapy, the risk for secondary malignancies, and the relatively short duration of follow-up.
Consultations
Radiation therapy with curative intent should be used in patients with stage I disease, and although this represents a minority of cases of follicular lymphoma, one may seek consultation with a radiation oncologist. Radiation therapy also can be used to treat localized or bulky lymphadenopathy that is causing obstruction or when a more urgent response is desired to relieve obstruction. Radiation therapy is usually tolerated well, and in many instances can spare the patient the need for additional chemotherapy. The radiation oncologist is also involved in the care of patients receiving radioimmunotherapy.
It is recommended that surgeons consult with pathologists before obtaining biopsy specimens to discuss the proper handling of the specimen and the special tests required.
Posttreatment Follow-up
Patients should be monitored periodically to facilitate early treatment of complications of the disease, such as biliary, ureteral, or bronchial obstruction due to increased adenopathy. See also Clinical Evaluation for follow-up evaluation in patients.
Prognosis and Prognostic Factors
The overall survival rate of patients with grade 1-2 follicular lymphoma has steadily improved in recent decades. [67] In a study of patients with follicular lymphoma from a Spanish registry who were prospectively enrolled from 1980 to 2013, median overall survival was over 20 years. [68]
The Follicular Lymphoma International Prognostic Index (FLIPI) is predictive of survival in patients with follicular lymphomas. [69] Patients who have 4 or more of the following adverse prognostic factors have a 10-year survival rate of approximately 36% (compared with 71% for those with 1 or none of these variables):
-
Age > 60 y
-
Ann Arbor Stage III-IV
-
Lactate dehydrogenase (LDH) level above the upper limit of normal
-
Hemoglobin level less than 12 g/dL
-
Four or more nodal sites of disease
In 2009, the International Follicular Lymphoma Prognostic Factor Project published an updated score, FLIPI2. The FLIPI2 includes the following risk factors (as with FLIPI1, each factor is worth 1 point) [70] :
-
Age > 60y
-
β2-microglobulin (B2M) above the upper limit of normal
-
Bone marrow involvement
-
Hemoglobin level < 12 g/dL
-
Longest diameter of the largest involved node > 6 cm
Based on the FLIPI2 score, patients can be categorized as follows [70] :
-
Low risk (0 or 1 point)
-
Intermediate risk (2 points)
-
High risk (≥3 points)
With this model, relapse-free and overall survival rates at 5 years are as follows:
-
0-1 risk factors: 79%
-
Two risk factors: 51%
-
Three or more risk factors: 20%
Vitamin D insufficiency has been linked with increased risk of early clinical failure in follicular lymphoma. Kelly et al reported that in follicular lymphoma patients undergoing chemotherapy, progression-free survival was worse in those who had vitamin D insufficiency. [71] In a prospective study of 642 patients with follicular lymphoma, 19% of whom had vitamin D level less than 20 ng/mL, Tracy et al reported that vitamin D insufficiency was associated with inferior lymphoma-specific survival and overall survival regardless of the treatment used (obesrvation, immunotherapy, or chemotherapy). [72]
Guidelines Summary
Guidelines contributors: Priyank P Patel, MD , Hematology/Oncology Fellow, Roswell Park Cancer Institute, University at Buffalo, Francisco J Hernandez-Ilizaliturri, MD, Chief, Lymphoma and Myeloma Section; Professor of Medicine, Department of Medical Oncology; Director of The Lymphoma Translational Research Program; Associate Professor of Immunology, Roswell Park Cancer Institute
Diagnosis
In addition to its general guidance on diagnosis of lymphoma, the National Comprehensive Cancer Network (NCCN) recommends the following studies to establish a diagnosis of follicular lymphoma (FL) [20] :
-
Immunohistochemistry panel: CD20, CD3, CD5, CD10, BCL2 BCL6, CD21 or CD23 with or without
-
Cell surface marker analysis by flow cytometry: kappa/lambda, CD19, CD20, CD5, CD23, CD10
European Society for Medical Oncology (ESMO) guidelines are in agreement with the NCCN that diagnosis follows the WHO classification and excisional biopsy is preferred. Core biopsy is considered only in cases where lymph nodes are not easily accessible. Fine-needle aspiration is not recommended. [73]
Risk Stratification
The Groupe d’Etude des Lymphomes Folliculaires (GELF) recommends the following criteria for identifying patients in whom immediate therapy is necessary [74] :
-
Three nodes in three distinct areas, with each node ≥3 cm in diameter
-
A tumor ≥7 cm in diameter
-
Presence of systemic symptoms
-
Symptomatic spleen enlargement
-
Ascites or pleural effusion
-
Cytopenias (leukocytes < 1.0 x 10 9/L and/or platelets < 100 x 10 9/L)
-
Leukemia (> 5.0 x 10 9/L malignant cells)
The NCCN recommends both the GELF criteria and the 2004 Follicular Lymphoma International Prognostic Index (FLIPI) for risk stratification. [20] (See Prognosis and Prognostic Factors.) FLIPI1 and FLIPI2 are used to predict prognosis but are not used to select treatment options.
Treatment
The NCCN and ESMO offer similar treatment recommendations, as follows [20, 73] :
-
Involved-site radiation therapy (ISRT), 24-30 Gy, is the preferred treatment option for stage I or II
-
If significant toxicity is expected from radiotherapy, initial observation may be more appropriate
-
Other first-line treatment options include rituximab, alone or in combination with other agents, and radioimmunotherapy
-
Combination treatment with involved-field radiation therapy (IFRT) and chemotherapy (see below) and/or radioimmunotherapy is recommended for more advanced stages
-
In asymptomatic patients with advanced-stage, low tumor burden disease, initiate treatment when the patients become symptomatic, as there is no survival advantage with immediate treatment versus a watch-and-wait approach
For first-line therapy, the NCCN recommends rituximab alone in patients with low tumor burden. In those with high tumor burden, the NCCN lists the following regimens as preferred first-line therapy [20] :
-
Bendamustine plus obinutuzumab or rituximab
-
CHOP (cyclophosphamide, doxorubicin [hydroxydaunorubicin], vincristine [Oncovin], prednisone) plus obinutuzumab or rituximab
-
CVP (cyclophosphamide, vincristine, prednisone) plus obinutuzumab or rituximab
-
Lenalidomide plus rituximab
Maintenance therapy with rituximab or obinutizumab may be considered in high-burden cases.
For second-line and subsequent therapy of FL, the NCCN recommends the following as preferred regimens [20] :
-
Bendamustine plus obinutuzumab or rituximab
-
CHOP plus obinutuzumab or rituximab
-
CVP plus obinutuzumab or rituximab
-
Lenalidomide plus rituximab
For elderly or infirm patients who are unlikely to tolerate those regimens, the NCCN recommends the following as first-line, second-line, and subsequent regimens:
-
Rituximab (preferred) (375 mg/m 2 weekly for 4 doses)
-
Chlorambucil, alone or plus rituximab
-
Cyclophosphamide, alone or plus rituximab
For third-line and subsequent therapy, the NCCN recommends second-line therapies not previously given, or T-cell engager therapy with one of the following as preferred regimens:
-
Bispecific antibody therapy with mosunetuzumab-axgb
-
CD19-directed chimeric antigen receptor (CAR) T-cell therapy with axicabtagene ciloleucel or tisagenlecleucel
Questions & Answers
Overview
What are the signs and symptoms of follicular lymphoma?
How is follicular lymphoma diagnosed?
How is follicular lymphoma staged?
How is follicular lymphoma graded?
How is follicular lymphoma treated?
What causes follicular lymphoma?
What is the pathophysiology of follicular lymphoma?
What is the prevalence of follicular lymphoma?
Which clinical history findings are characteristic of follicular lymphoma?
Which physical findings are characteristic of follicular lymphoma?
What are the stages of follicular lymphoma?
What is included in the differential diagnoses of follicular lymphoma?
What is the role of lab testing in the workup of follicular lymphoma?
What is the role of imaging studies in the workup of follicular lymphoma?
What is the role of biopsy in the workup of follicular lymphoma?
What is the role of bone marrow aspiration in the diagnosis of follicular lymphoma?
What is the role of immunophenotyping in the diagnosis of follicular lymphoma?
What is the role of PCR in the workup of follicular lymphoma?
Which histologic findings are characteristic of follicular lymphoma?
Which pathologic classification systems are used to diagnose follicular lymphoma?
What is the WHO classification of follicular lymphoma?
Which medications are used in the treatment of follicular lymphoma?
What is included in patient education about follicular lymphoma?
What is the role of radiotherapy in the treatment of follicular lymphoma?
What is the role of observation in the treatment of follicular lymphoma?
What is the role of duvelisib in the treatment of follicular lymphoma?
What is the role of single-agent therapy in the treatment of follicular lymphoma?
What is the role of chlorambucil in the treatment of follicular lymphoma?
What is the role of fludarabine in the treatment of follicular lymphoma?
What is the role of bendamustine in the treatment of follicular lymphoma?
What is the role of rituximab in the treatment of follicular lymphoma?
What is the role of idelalisib (Zydelig) in the treatment of follicular lymphoma?
What is the role of copanlisib in the treatment of follicular lymphoma?
What is the most common first-line treatment of follicular lymphoma in the US?
Which combination chemotherapy regimens are used in the treatment of follicular lymphoma?
What is the efficacy of combination chemotherapy regimens in the treatment of follicular lymphoma?
What is the role of obinutuzumab (Gazyva) in the treatment of follicular lymphoma?
How is obinutuzumab administered in the treatment of follicular lymphoma?
What is the role of targeted radioimmunotherapy in the treatment of follicular lymphoma?
Which specialist consultations are beneficial to patients with follicular lymphoma?
What posttreatment follow-up are indicated in the treatment of follicular lymphoma?
What is the prognosis of follicular lymphoma?
What are the most commonly used classification schemas for follicular lymphoma?
What the WHO guidelines for grading follicular lymphoma?
What are the NCCN diagnostic guidelines for follicular lymphoma?
What are the GELF criteria for risk stratification in follicular lymphoma?
What is the FLIPI2 for risk stratification of follicular lymphoma?
What are the NCCN and ESMO treatment guidelines for follicular lymphoma?
What are the NCCN treatment guidelines for follicular lymphoma?
-
Follicular lymphoma, low-power view. Note the nodular pattern reminiscent of germinal centers. Photograph courtesy of Aamir Ehsan, MD.
-
Diffuse lymphoma. Note the absence of the nodular pattern observed in follicular lymphomas. Photograph courtesy of Aamir Ehsan, MD.
-
A patient with follicular lymphoma who was diagnosed 6 years earlier presents to his hematologist's office because of rapidly growing lymphadenopathy and onset of fever, severe night sweats, and weight loss. In the past, he had been treated with chlorambucil and prednisone when his submandibular lymph nodes became large enough to make him uncomfortable. This treatment had worked well, and he has not required any treatment recently. A biopsy of an involved lymph node is obtained. The diagnosis is transformation to diffuse non-Hodgkin lymphoma.
Tables

What would you like to print?
- Practice Essentials
- Etiology and Pathophysiology
- Epidemiology
- Clinical Evaluation
- Staging
- Differential Diagnosis
- Routine Laboratory Tests
- CT and PET Scanning
- Biopsies
- Histologic Findings
- Management Overview
- Radiotherapy - Localized Disease
- Observation - Asymptomatic Advanced Disease
- Single-Agent Therapy
- Multiagent Chemotherapy
- Hematopoietic Stem Cell Transplantation
- Targeted Radioimmunotherapy
- Consultations
- Posttreatment Follow-up
- Prognosis and Prognostic Factors
- Guidelines Summary
- Questions & Answers
- Show All
- Media Gallery
- References





