Background
Immunodeficiency diseases are commonly classified into disorders that affect one or more of the 4 major limbs of the immune system. These limbs are (1) B cells, ie, humoral immunity; (2) T cells, ie, cell-mediated immunity; (3) phagocytes; and (4) complement.
B-cell immunity is mediated by the immunoglobulins and is commonly referred to as humoral immunity. Humoral immunity is differentiated from T-cell immunity, which is commonly referred to as cellular immunity, and from phagocytic cell immune function. Immunoglobulins, which are protein molecules that contain antibody activity, are produced by the terminal cells of B-cell differentiation known as plasma cells. Immunoglobulins have important roles in humoral immunity, and they consist of 5 major classes or isotypes: immunoglobulin G (IgG), immunoglobulin A (IgA), immunoglobulin M (IgM), immunoglobulin D (IgD), and immunoglobulin E (IgE). The most abundant class of immunoglobulins in the blood is IgG (73%), which has a molecular weight of 150 kd. IgG is present in plasma and external secretions and is expressed on the B-cell membrane.
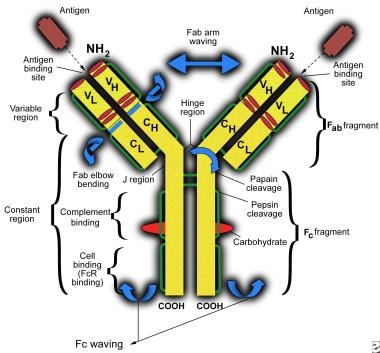 Immunoglobulin G deficiency. Schematic representation of an immunoglobulin G molecule. CH indicates constant region of heavy chain; CL, constant region of light chain; VH, variable region of heavy chain; and VL, variable region of light chain.
Immunoglobulin G deficiency. Schematic representation of an immunoglobulin G molecule. CH indicates constant region of heavy chain; CL, constant region of light chain; VH, variable region of heavy chain; and VL, variable region of light chain.
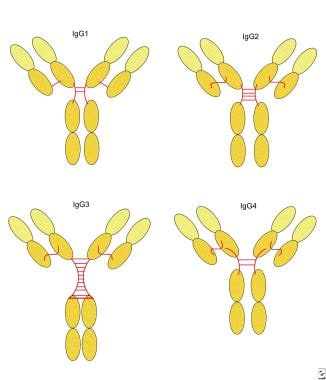
IgG is further subdivided into 4 subclasses: IgG1, IgG2, IgG3, and IgG4. Fortunately, for ease of recall, the serum concentrations of the subclasses directly correlate with their numerical nomenclature, such that IgG1 is found in greater concentrations than IgG2, and so forth.
In 1952, Bruton described classic X-linked agammaglobulinemia due to B-cell deficiency in an 8-year-old boy. The child presented with frequent pyogenic infections, repeated episodes of sepsis with the same serotypes of pneumococcus, and multiple episodes of mumps, yet he had no antibodies against these pathogens. Serum protein electrophoresis had just become available, and it revealed that the g fraction was missing from the child’s blood. Subsequently, patients were described who had detectable lymphoid tissue and B-cells but had decreased IgG levels and/or lacked specific antibodies. These conditions are now recognized as fitting the categories of hyper-IgM syndromes and common variable immunodeficiency (CVID). A new subset of the latter was recently characterized by reduced C1 esterase inhibitor levels. [1]
In the early 1960s, following the discovery of the IgG subclasses, certain associations were also recognized between individual subclass deficiencies, decreased ability to respond to certain types of antigens (ie, bacterial polysaccharides), and recurrent infection. IgG deficiencies may occur as isolated deficiencies (eg, selective IgG deficiency) or in association with deficiencies of other immunoglobulin types. Moreover, even if the total IgG concentration is normal, deficiencies of one or more individual IgG subclasses, significant decreases in specific IgG antibodies, or both may be observed.
Ig G deficiency in children with recurrent respiratory infections with and without history of allergy was evaluated. [2] A variable IgG deficiency was documented in less than one-third of the subjects, but that provided no asistance in the differential diagnostics of the allergic background of these children.
For information on deficiencies of other immunoglobulin types, see the Medscape Reference articles IgA Deficiency, IgD Deficiency, and IgM Deficiency.
Pathophysiology
B and T cells are responsible for specific immunity, otherwise known as adaptive immunity. Adaptive immune responses require rearrangement of the genes responsible for the specific recognition structures, ie, immunoglobulins for humoral immunity and T-cell receptors for cellular immunity. Inability to form these recognition structures or blocks in the differentiation and development of either of these cell types results in primary immune deficiency. Abnormal production of these cells may also be observed in clinical states in which production of abnormal cell types is pathologically excessive (eg, lymphoproliferative diseases such as lymphoma and leukemia) or in immunodeficiency disorders in which production is aberrantly low. [3] Humoral immune defects can also result from excessive loss of antibody proteins (eg, protein-losing enteropathy, certain forms of nephritis), even though the B-cell mass may be normal in those conditions.
IgG is well distributed in intravascular and extravascular spaces and is important in the secondary antibody responses (immune memory). It plays an important role in host defense against infection. IgG protects tissues from bacteria, viruses, and toxins. Different subclasses of IgG neutralize bacterial toxins, activate complement, and enhance phagocytosis by opsonization. [4]
Importantly, note that a low IgG level, with normal IgA and IgM levels, does not necessarily equate with antibody deficiency. The evaluation of specific antibody responses is essential for the diagnosis and for appropriate treatment.
For ease of discussion, IgG deficiencies may be divided into 2 categories. The first is selective IgG deficiency, which consists of an isolated deficiency of IgG with normal levels of IgA, IgM, IgD, and IgE. The second is a deficiency of IgG accompanied by inadequate levels of other immunoglobulin isotypes. This may occur in various conditions, including X-linked agammaglobulinemia (X-LA), common variable immunodeficiency (CVID), and hyper-IgM syndromes.
These disorders occur in persons of any age or sex. Selective immunoglobulin deficiencies were previously referred to as late-onset agammaglobulinemia, and now they are classified under the general designation of antibody deficiency. Both pediatric and adult populations may be affected by specific or selective antibody deficiencies, CVID, or both. See Common variable immunodeficiency for more details.
IgA deficiency is the most common immune deficiency. Although some "normal" blood donors may be found to be deficient in IgA, approximately 20% of patients who lack IgA are also deficient in IgG2 and IgG4. These individuals appear to have a greater risk of infection than patients with isolated IgA deficiency.
Epidemiology
Frequency
Although the frequency of isolated IgG deficiency is not known with certainty, deficiencies in specific IgG antibody or IgG subclass is probably more common and occurs in families with common variable immunodeficiency (CVID). Some reports indicate that the prevalence of IgG deficiency may be 1 case per 10,000 persons.
Mortality/Morbidity
Early diagnosis and treatment of IgG deficiency is essential to prevent and control both morbidity and mortality. IgG subclass deficiency is associated with shorter treatment-free and overall survival in chronic lymphocytic leukemia. [5]
IgG subclass levels are highly variable, even within individuals at different points in time. Their development in early childhood varies from subclass to subclass; IgG 2 is the slowest to reach adult values. Additional deficiencies may become apparent because of defective switching between different IgG subclasses.
Demographics
Both children and adults are affected. Children younger than 24 months cannot make much IgG2; hence, measuring the IgG2 subclass concentration before this age is not meaningful.
The most common subclass deficiency in early childhood is IgG2 deficiency; in adults, IgG1 and IgG3 deficiencies predominate. IgG1 accounts for a higher proportion of the total IgG in children as compared to adults. Although children rapidly attain adult levels of IgG1 and IgG3, the development of IgG2 and IgG4 is slower. In some children, maturation of the full range of IgG subclasses may be delayed until the teenage years. Note the figure below.
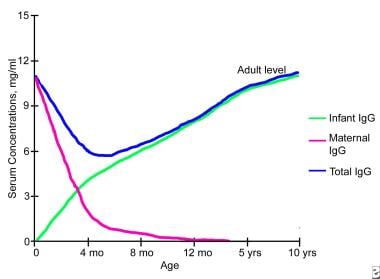 Immunoglobulin G deficiency. Changes in serum immunoglobulin G concentrations during infancy and childhood.
Immunoglobulin G deficiency. Changes in serum immunoglobulin G concentrations during infancy and childhood.
One recent study found an isolated IgG3 subclass deficiency was the most common IgG subclass deficiency in Thai children. IgG3 subclass deficiency, either isolated or combined with other IgG subclass deficiency, was found in 85.5% of 55 children, most of whom were first evaluated for recurrent sinusitis. [6]
-
Immunoglobulin G deficiency. Schematic representation of an immunoglobulin G molecule. CH indicates constant region of heavy chain; CL, constant region of light chain; VH, variable region of heavy chain; and VL, variable region of light chain.
-
Immunoglobulin G deficiency. Human immunoglobulin G subclasses.
-
Immunoglobulin G deficiency. Changes in serum immunoglobulin G concentrations during infancy and childhood.
-
Immunoglobulin G deficiency. Schematic representation of the molecular interaction of CD40 on B cells, with CD40L on T cells involved in the switch from immunoglobulin M to immunoglobulin G.




