Practice Essentials
Hypopharyngeal cancer is a term used for tumors of a subsite of the upper aerodigestive tract, and like most other subsite designations, the distinction is anatomic rather than pathophysiologic within the group of head and neck malignancies. [1] The hypopharynx is the region between the oropharynx above (at the level of the hyoid bone) and the esophageal inlet below (at the lower end of the cricoid cartilage). Embryologically, the larynx interjects into the hypopharynx anteriorly and is therefore considered a separate structure.
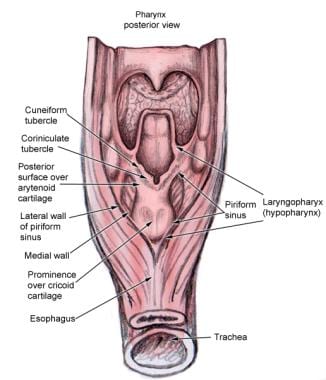
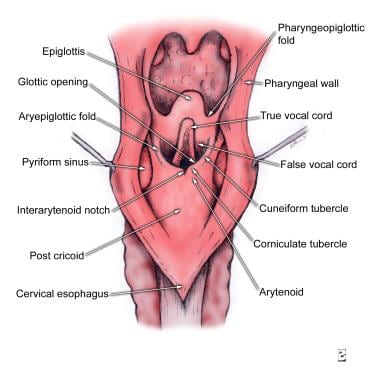
Hypopharyngeal cancers are often named for their location, including pyriform sinus, lateral pharyngeal wall, posterior pharyngeal wall, or postcricoid pharynx (see images below). Most arise in the pyriform sinus. In the United States and Canada, 65-85% of hypopharyngeal carcinomas involve the pyriform sinuses, 10-20% involve the posterior pharyngeal wall, and 5-15% involve the postcricoid area. [2]
 The hypopharynx is the longest of the 3 segments of the pharynx. It is wide superiorly and progressively narrows toward the level of the cricopharyngeal muscle. It is bounded anteriorly by the posterior face of the cricoid cartilage. The parts of the hypopharynx that lie partly to each side of the larynx form the pyriform sinuses or fossae.
The hypopharynx is the longest of the 3 segments of the pharynx. It is wide superiorly and progressively narrows toward the level of the cricopharyngeal muscle. It is bounded anteriorly by the posterior face of the cricoid cartilage. The parts of the hypopharynx that lie partly to each side of the larynx form the pyriform sinuses or fossae.
As in other head and neck cancer sites, more than 95% of hypopharyngeal malignancies arise from the epithelium of the mucosa and, therefore, are squamous cell cancers. Premalignant mucosal lesions evolve into hyperproliferative lesions that develop the capacity to enlarge, to invade local structures, to invade lymphatics to spread to regional lymph nodes, and to invade vascular channels to metastasize to other organs.
Signs and symptoms of hypopharyngeal cancer
Symptoms of hypopharyngeal cancer include the following:
-
Dysphagia
-
Chronic sore throat
-
Foreign body sensation in the throat or referred otalgia
Other symptoms, which usually develop later, include the following:
-
Weight loss
-
Hemoptysis
-
Laryngeal stridor
-
Hoarseness - When the vocal cord becomes affected by direct extension into the arytenoid cartilage or the recurrent laryngeal nerve
Workup in hypopharyngeal cancer
Lab studies include the following:
-
Complete blood count (CBC)
-
Hepatic enzymes
-
Serum creatinine
-
Prothrombin time (PT) and activated partial thromboplastin time (aPTT)
-
Serum albumin
-
Serum calcium
-
Thyroid stimulating hormone (TSH)
Imaging studies include the following:
-
Chest radiography
-
Computed tomography (CT) or magnetic resonance imaging (MRI) scan of oral cavity and neck
-
Positron emission tomography (PET) scan
-
Abdominal CT scan
-
Bone scan
Diagnostic procedures include the following:
-
Biopsy
-
Triple endoscopy (panendoscopy)
Management of hypopharyngeal cancer
The management of hypopharyngeal cancer can be broken down based on stage, as follows:
-
T1/T2 - Radiotherapy alone (commonly 66-70 Gy) or surgery (possibly with postoperative irradiation, depending on the pathology findings); larynx preservation therapy is typically possible and is strongly favored
-
T3/T4 (resectable) - Partial or total laryngopharyngectomy, neck dissection, postoperative radiotherapy, or radiotherapy alone with altered fractionation or concurrent chemoradiotherapy or participation in prospective clinical trials
-
Unresectable or medically unstable - (1) Radiotherapy alone with altered fractionation or concurrent chemoradiotherapy or (2) participation in prospective clinical trials including the study of induction chemotherapy
Prognosis
The biological behavior of carcinoma of the hypopharynx differs greatly from that of carcinoma of the larynx. Carcinomas of the hypopharynx are usually poorly differentiated and patients are usually asymptomatic; early presentations are unfortunately uncommon. In fact, T1 N0 cases (see Staging in Workup) account for only 1-2% of all patients seen.
Most patients have no symptoms to bring them to medical attention until their disease is advanced, at which point the prognosis is poor. The rate of metastases is high, with nodal involvement present in 50-70% of cases at presentation. Of patients with hypopharyngeal cancers, 70% have stage III disease at presentation. Cervical lymph node metastases occur as the presenting symptom in approximately 50% of cases. The frequency of distant metastases is also among the highest of all head and neck cancers. [3]
The aforementioned study by Kuo and colleagues found that the 5-year overall survival rate for hypopharyngeal cancer rose significantly from 1988-1990 and from 1991-1995 but that no significant changes in survival rate could be demonstrated for other years. The investigators also found that survival was significantly affected by the following factors [4] :
-
Age: Worse in patients aged 65-74 years, 75-84 years, or 85 years or older than in those aged 18-54 years
-
Race: Worse in white patients than in patients of other non-African races
-
T category: Worse in cases of category T2, T3, or T4 than in T1
-
N category: Worse in cases of category N2 or N3 than in N0 [5]
-
Treatment modality: Worse when treatment involved no surgery or radiation, radiation without surgery, or surgery without radiation than when therapy included surgery and radiation combined
As stated, prognosis in hypopharyngeal cancer varies with the stage. The 5-year survival rate with small (T1-T2) lesions is about 60%, but with T3-T4 lesions or multiple node involvement, survival falls to 17-32%. Five-year survival for all stages is approximately 30%. A study by Lo et al indicated that in patients with resectable stage 4 hypopharyngeal cancer, a lymph node ratio of 0.113 or greater is a significant risk factor for disease recurrence and signals a poor prognosis for overall survival. [6]
Morbidity in hypopharyngeal cancer is predominantly due to the primary tumor itself causing pain, bleeding, poor swallowing (with subsequent malnutrition), or aspiration. Very advanced tumors may cause airway obstruction as they grow into the larynx. Laryngectomy is often needed, leading to permanent loss of voice and permanent tracheostomy. Functional problems from surgical or radiation treatment can include swallowing dysfunction, recurrent aspiration pneumonias, neck fibrosis, facial edema, and pain.
Epidemiology
Frequency
Cancer that arises in the hypopharynx represents approximately 7% of all cancers of the upper aerodigestive tract. The incidence of laryngeal cancer is 4-5 times that of hypopharyngeal cancer. All pharyngeal subsites accounted for approximately 124,000 cancer cases worldwide in 2002.
In a retrospective cohort study, Kuo et al reported a decline in the incidence of hypopharyngeal cancer in the United States by an average of -2.0% annually between 1973 and 2010. The study involved 3958 adults with the disease, with information culled from the Surveillance, Epidemiology, and End Results (SEER) program database. [4]
A study by Jakobsen et al found that between 1980 and 2014, the age-adjusted incidence rate for hypopharyngeal cancer in Denmark rose from 0.3 per 100,000 to 1.1 per 100,000 (a 4.1% per year increase). [7]
Race
African Americans have had an increasing incidence of cancers of all pharyngeal subsites since the early 1970s.
Sex
US incidence indicates an approximate male-to-female ratio of 3:1. Women have a higher incidence of postcricoid cancers related to nutritional deficiencies (Plummer-Vinson syndrome) than men. The prognosis for women generally is better than that for men.
Age
The incidence of hypopharyngeal cancer rises in people older than 40 years; it is rare in people younger than 30 years. The mean age at presentation is 65 years. Patients diagnosed with hypopharyngeal cancer are typically men aged 55-70 years with a history of tobacco use and/or alcohol ingestion.
Clinical Presentation
History
In general, hypopharyngeal cancers involve a tumor that is relatively more silent than other head and neck cancer tumors. Larger lesions are required to produce symptoms. The time between initial symptoms and diagnosis is longer than that for laryngeal tumors or other cancers because of the relatively few early symptoms and the difficulty of physical examination in this region.
Symptoms of hypopharyngeal cancer include dysphagia, chronic sore throat, and foreign body sensation in the throat or referred otalgia. (Otalgia is pain referred to the ear via the Arnold nerve, a division of the 10th cranial nerve. It suggests an underlying malignancy.) For hypopharyngeal cancer, a metastatic node in the neck is often the presenting symptom. An asymptomatic mass in the neck, usually a jugulodigastric or jugulo-omohyoid lymph node, is present in 20% of patients. The average duration of symptoms before presentation is 2-4 months.
Other symptoms, which usually develop later, include weight loss, hemoptysis, laryngeal stridor, and hoarseness when the vocal cord becomes affected by direct extension into the arytenoid cartilage or the recurrent laryngeal nerve. Of patients with hypopharyngeal cancers, 70% have stage III disease at presentation.
-
Neck mass: Cervical lymph node metastases occur as the presenting symptom in approximately 50% of cases. As many as 70% of patients with pyriform sinus lesions have palpable lymph nodes upon initial clinical examination.
-
Sore throat
Typically, pain is unilateral and well localized.
Often, pain radiates to the ears.
Patients commonly undergo one or more courses of empiric antibiotics without response.
-
Hoarseness: This indicates either involvement of the recurrent laryngeal nerve, which runs deep to the anterior wall of the pyriform sinus, or direct invasion of the larynx (see image below).
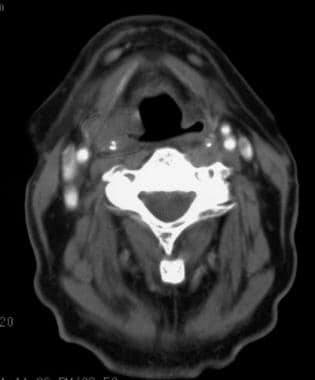 Patient presenting with hoarseness and dysphagia. CT scan demonstrated bulky right pyriform sinus tumor eroding through thyroid cartilage, with displacement of supraglottic airway. Total laryngectomy would have been required, because the patient placed a high value on retaining the ability to talk, chemoradiotherapy was chosen. Following chemoradiotherapy, note persistent fullness in tumor bed. Endoscopy revealed edema and scarring, but the biopsy was negative for tumor. Continued vigilance is needed in this situation.
Patient presenting with hoarseness and dysphagia. CT scan demonstrated bulky right pyriform sinus tumor eroding through thyroid cartilage, with displacement of supraglottic airway. Total laryngectomy would have been required, because the patient placed a high value on retaining the ability to talk, chemoradiotherapy was chosen. Following chemoradiotherapy, note persistent fullness in tumor bed. Endoscopy revealed edema and scarring, but the biopsy was negative for tumor. Continued vigilance is needed in this situation.
-
Dysphagia (See image below. See related CME at Diagnostic Evaluation of Dysphagia.)
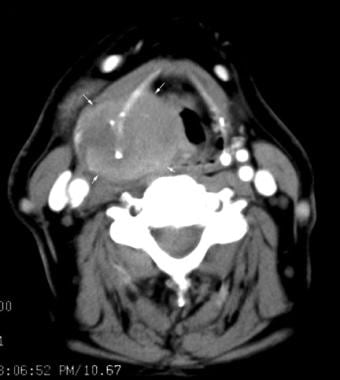 Patient presenting with hoarseness and dysphagia. CT scan demonstrates bulky right pyriform sinus tumor (white arrows) eroding through thyroid cartilage, with displacement of supraglottic airway. A total laryngectomy would have been required, because the patient placed a high value on retaining the ability to talk, chemoradiotherapy was chosen.
Patient presenting with hoarseness and dysphagia. CT scan demonstrates bulky right pyriform sinus tumor (white arrows) eroding through thyroid cartilage, with displacement of supraglottic airway. A total laryngectomy would have been required, because the patient placed a high value on retaining the ability to talk, chemoradiotherapy was chosen.
See the list below:
Tumor invasion often causes a combination of painful swallowing (odynophagia) and neuromuscular dysfunction (dysphagia). Patients frequently report food sticking in the upper esophagus or upper throat; this is because the hypopharynx is involved in the coordination of the swallowing function around the larynx.
Aspiration is occasionally seen.
Weight loss and malnutrition are common at presentation.
-
Otalgia: Referred pain to the ear is mediated by branches of the tenth cranial nerve (see image below). Invasion of the laryngeal nerve causes spread of neuropathic impulses to the auricular nerve (sensory to posterior external auditory canal and back of pinna).
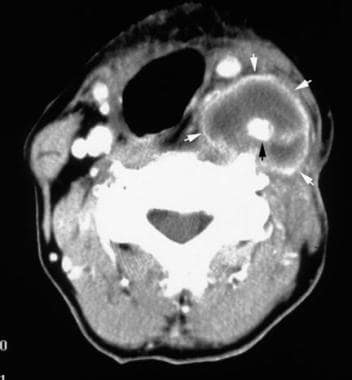 Patient presented with hoarseness and otalgia. On MRI, there was a bulky left pyriform sinus tumor with an area of gadolinium enhancement extending to the carotid sheath. This T4 tumor was unresectable, and the patient was treated with chemoradiation. Despite a good response to chemoradiotherapy, the evaluation for progressive neck pain 4 months later revealed a bulky recurrence in the left neck. Note tumor (white arrows) surrounding the carotid artery (black arrow).
Patient presented with hoarseness and otalgia. On MRI, there was a bulky left pyriform sinus tumor with an area of gadolinium enhancement extending to the carotid sheath. This T4 tumor was unresectable, and the patient was treated with chemoradiation. Despite a good response to chemoradiotherapy, the evaluation for progressive neck pain 4 months later revealed a bulky recurrence in the left neck. Note tumor (white arrows) surrounding the carotid artery (black arrow).
-
Hemoptysis
-
Halitosis: Fetid breath is due to saprophytic bacterial overgrowth in fungating necrotic tumors.



Physical Examination
Assessment begins in the office with a thorough head and neck examination, including inspection, palpation, and indirect or fiberoptic examination. Flexible fiberoptic endoscopic examination is important to attempt to localize and stage the primary tumor. Because of the patient's gag reflex, a flexible fiberoptic examination is the preferred examination technique and often allows the mucosa of the hypopharynx to be well examined. Hypopharyngeal cancer is typically advanced at presentation, and an obvious abnormality is usually present in either the pharynx or the neck. Occasionally, only subtle signs such as submucosal fullness or unilateral pooling of saliva are present. Typical findings of hypopharyngeal cancer include mucosal ulceration; pooling of the saliva in the pyriform fossa; edema of the arytenoids; or fixation of the cricoarytenoid joint, true vocal cords, or both.
During the flexible laryngoscopy, the assessment of vocal cord mobility or fixation is important for staging purposes. The patient who puffs out his or her cheeks or performs a Valsalva maneuver may distend the pyriform fossae for inspection.
The neck should be examined in a systematic fashion. Any lymph nodes should be assessed with regard to size, location, and mobility. On neck examination, loss of the grating sensation (laryngeal crepitus) of the laryngeal cartilages over the prevertebral tissues may indicate deep pharyngeal wall involvement.
-
Oral examination
The hypopharynx is not visible directly, but other regional pathologies, including the synchronous oral cavity or oropharyngeal tumors, might be seen.
Asymmetry of tonsillar pillars can be a clue to a tumor invading the palatopharyngeus muscle at insertion to the inferior constrictor muscle.
-
Larynx and pharynx examinations
The mirror examination is the quickest and simplest screening tool, but it cannot reveal lower pyriform sinus or postcricoid lesions. Fiberoptic laryngoscopy is the examination of choice.
Findings include mass lesions, hyperkeratotic or erythematous mucosal lesions, ulcerations, and vocal cord paralysis.
-
Neck examination
Examine and document the size, location, and number of palpable lymph nodes in all cervical and supraclavicular node-bearing areas.
Palpate and wiggle the larynx from side to side. Tenderness suggests invasion, while loss of normal tracheal crepitus suggests invasion of prevertebral tissue or a large postcricoid tumor.
-
Head examination
Assess cranial nerve function.
Assess jaw mobility. Trismus suggests invasion of pterygoid muscles.
Areas of mass lesions or tenderness are suggestive of regional metastases.
-
General examination for distant metastases and comorbidities
Examination of the lungs may reveal chronic obstructive pulmonary disease (COPD). Chest radiography may demonstrate metastases, synchronous lesions, or effusions suggesting metastases to pleura or lymphatic obstruction.
Examination of the heart may demonstrate congestive heart failure (CHF) or right-sided failure and pulmonary hypertension.
Examination of the extremities may reveal peripheral vascular disease or clubbing suggestive of advanced lung disease or synchronous lung cancer.
Hepatomegaly with a hard irregular contour suggests metastatic disease.
General neurologic examination may show toxic or metabolic encephalopathy or neuropathy. Focal neurologic findings suggest brain metastases or prior cerebrovascular accident (CVA).
Perform a peripheral lymph node examination to assess for possible distant lymph node metastases.
Natural History of Hypopharyngeal Squamous Cell Carcinomas
See the list below:
-
In general, 30% of patients have local disease at the time of diagnosis, 60% have local regional disease, and 10% present with distant metastases. In the United States, most hypopharyngeal tumors (60-70%) arise in the pyriform sinus, 25% are found in the posterior pharyngeal wall, and 5% are found in the posterior cricoid region.
-
Most patients present with large T3 or T4 tumors (see Staging in Workup).
-
Medial wall pyriform sinus tumors usually spread along the mucosal surface to the aryepiglottic folds and can invade into the larynx by involving the paraglottic space.
-
Tumors of the lateral wall and apex commonly invade the thyroid cartilage.
-
Once the tumor penetrates the constrictor muscle, it can spread along the fascial planes to the base of skull.
-
Because of the abundant lymphatics in the region and the extent of the primary tumor at diagnosis, metastasis to the regional lymph nodes is common.
Pathology
More than 95% of hypopharyngeal tumors are squamous cell carcinoma, less than 60% are keratinizing, 33% are nonkeratinizing, and all are usually poorly differentiated. Variants include basaloid squamous cell carcinoma, superficial spreading cancer, sebaceous cancer, adenosquamous cancer, and signet-ring and verrucous types. Uncommon histologic types include adenocarcinoma, lymphoma, and sarcoma.
Studies have reported that tumor margins are usually infiltrating (80%) but can be pushing (20%). Unsuspected submucosal spread can extend beyond 1 cm of visible tumor margins. Skip lesions or multifocal areas of disease are not unusual.
Etiology and Risk Factors
Patients diagnosed with hypopharyngeal cancer are typically men aged 55-70 years with a history of tobacco use, alcohol ingestion, or both. The combined use of tobacco and alcohol has a synergistic effect on the incidence of hypopharyngeal cancer. [8]
One exception is an increased incidence of postcricoid cancer in women aged 30-50 years with Plummer-Vinson or Paterson-Kelly syndrome. This syndrome includes dysphagia, hypopharyngeal and esophageal webs, weight loss, and iron deficiency anemia. Currently in the United States, because of the reduced incidence of Plummer-Vinson syndrome, postcricoid carcinoma is more common in men.
Asbestos may pose an independent risk for the development of hypopharyngeal cancer. [9]
The etiology of squamous cell cancers is similar for most anatomic subsites. Tobacco and ethanol are the principle carcinogens responsible. Long-term exposure causes progressive cellular dysregulation by alteration of tumor suppressor genes such as TP53, amplification of proto-oncogenes such as cyclin D1, and damage to regulatory factors such as transforming growth factor–beta (TGF-beta) and retinoic acid receptors. The progression from normal mucosa to cancer correlates with accumulation of genetic abnormalities.
The role of human papilloma virus (HPV) in cancers of the hypopharynx is unclear, although it may play more of a role in cancers of the oropharynx and oral cavity. Nonsmokers with cancers of the head and neck are more likely to have detectable HPV, although this is less common than hypopharyngeal cancer in persons who smoke.
-
Clinically, the mucosa first develops dysplastic lesions that may appear white (leukoplakia) or red (erythroplasia), and with time and continued carcinogen exposure, lesions can develop into frank malignancy.
-
Nutritional and metabolic deficiencies are implicated in rare instances. Plummer-Vinson syndrome, mucosal webbing of the postcricoid area with iron deficiency, is associated with a higher incidence of cancer in that region. This is most common in women from northern Europe, including nonsmokers. The pathophysiology is not clear.
-
Genetic factors are under investigation. Heritable polymorphisms of expression of enzymes that activate tobacco-related protocarcinogens (eg, aryl hydrocarbon hydroxylase) and detoxify carcinogens (eg, glutathione S-transferase) have been identified. Certain polymorphisms in the alcohol dehydrogenase genes may increase the risk of oral and pharyngeal cancers related to alcohol consumption. Racial differences in the metabolism of carcinogens may be a possible cause of the increasing incidence in African Americans.
-
Clinical testing for peripheral blood lymphocyte chromosome fragility shows promise for identifying individuals at high risk of primary and secondary head and neck cancers, but it is still investigational.
-
Deficient DNA repair mechanisms increase susceptibility to head, neck, and other cancers. Clinically recognized syndromes include xeroderma pigmentosum, Bloom syndrome, ataxia-telangiectasia, and Fanconi anemia. Head and neck cancers are not constituents of the most common cancer family syndromes, which include nonpolyposis colorectal cancer, Li-Fraumeni, or BRCA1/BRCA2 mutation kindreds.
Risk factors
See the list below:
-
The main risk factors associated with this disease are alcohol and tobacco use. Alcohol is a significant cofactor in the development of hypopharyngeal cancer. It can act as a promoter of the mutagenic effects of tobacco-derived substances. Smoking cessation is associated with improved response to radiation, improved survival, and lower risk of second primary cancers.
-
Lower hypopharyngeal tumors can be associated with iron and vitamin C deficiencies. For example, Plummer-Vinson syndrome is characterized by hypopharyngeal webs, dysphagia, weight loss, and iron deficiency anemia. This syndrome has historically been associated with a high incidence of postcricoid carcinomas in Northern European women who do not smoke.
-
Chronic irritation of the pharynx from gastroesophageal or laryngotracheal reflux of the gastric contents has also been associated with the development of tumors in the posterior cricoid region, and such symptoms need to be addressed in the overall management of the tumor.
-
Regional differences have been reported and are apparent when cases in the United States are compared with those in Europe, Asia, or Africa.
In the United States, two thirds of tumors arise in the pyriform sinus region.
Women in Northern European countries who do not smoke develop postcricoid squamous cell carcinoma because of its association with Plummer-Vinson syndrome. This cause has greatly decreased with improved nutrition.
A report from Egypt indicated that postcricoid tumors were the most common (50%) hypopharyngeal tumors in the patients studied, but no clear evidence was available to explain why this site predominated. [10]
-
Ultimately, the possible biologic factors responsible for the development of these tumors await further investigation. Genetic deficiencies that affect the metabolism of tobacco-related and other carcinogens and malfunctions in DNA repair mechanisms and cell-cycle regulation may play a role.
Workup
The workup includes an initial history and physical examination, including a well conducted flexible fiberoptic endoscopic examination. The flexible fiberoptic examination is the preferred examination to determine the mucosal anatomy because of the location of the hypopharynx and the patient's gag reflex. This examination is complementary to imaging studies, which permit an evaluation of deeper anatomic structures but do not allow an adequate view of the mucosal anatomy. Imaging studies should be not be considered as a replacement for a flexible fiberoptic examination. [11]
See related CME at New Ways to Investigate Esophageal Function: pH, Impedance, Manometry, Capsules, and More. (Slides With Transcript).
Differentials
Differential diagnoses include the following:
Lab studies
See the list below:
-
Complete blood count (CBC)
During general assessment of bone marrow function, check for the presence of anemia due to chronic disease, metabolic derangements, or occult blood loss. Macrocytic RBCs may hint at chronic alcohol abuse common in this population. Thrombocytopenia may suggest hypersplenism or nutritional deficiency.
A CBC helps to assess the patient's ability to tolerate myelosuppressive chemotherapy and radiotherapy.
-
Hepatic enzymes: Check for underlying liver disease or liver metastases.
-
Serum creatinine
Assess renal function for general tolerance to therapy.
Measure 24-hour creatinine clearance if the serum creatinine concentration is elevated and cisplatin chemotherapy is under consideration.
-
Prothrombin time (PT) and activated partial thromboplastin time (aPTT): These are used to assess the safety of biopsy and other surgical procedures. Prolonged results may indicate hepatic insufficiency.
-
Serum albumin: Assess the nutritional status.
-
Serum calcium: Paraneoplastic hypercalcemia is common with head and neck cancer, even if it is not metastatic.
-
Thyroid stimulating hormone (TSH): Check for underlying hypothyroidism. Radiation induces hypothyroidism in approximately 30-40% of patients. This risk may be greater in the era of intensity-modulated radiation therapy (IMRT). This may happen more quickly and more severely in those with hypothyroidism prior to treatment.
Imaging studies
See the list below:
-
Chest radiography
Check for lung metastases, synchronous lung cancer, and comorbid heart or lung disease. Because of the morbidity associated with definitive treatment in the neck, excluding the presence of distant metastasis (especially to the lungs) is often advisable in patients who present with significant cervical nodal metastasis, which increases the risk of distant metastasis.
If hypopharynx cancer is aggressive (T4, N2-N3, or poorly differentiated histology), consider chest CT scan or positron emission tomography (PET) scan for most sensitive detection of metastases.
Barium swallow is not usually used unless the lesion is too large to introduce a scope, but its findings can help determine the inferior border of the lesion and the involvement of the esophageal inlet. If used, perform this test after the physical examination and with anesthesia because it can obscure tissues until the barium passes.
This may be helpful in patients with no obvious abnormality found on physical examination.
Negative swallow study findings with progressive or continuous symptoms should not preclude an endoscopic examination
Superficial mucosal lesions in the pyriform sinus are seen on barium studies, although this is not the imaging modality of choice.
-
CT scan or MRI of oral cavity and neck
In patients with hypopharyngeal cancer, CT scan and MRI are used to visualize the primary tumor and regional lymph nodes prior to definitive treatment. These modalities provide information about the location and extent of tumor involvement and demonstrate the interface of tumor with bone, fat, muscles, soft tissues, blood vessels, dura, and brain.
The contrast-enhanced CT scan is typically used as the initial imaging modality to assess local tumor extent and evaluate lymph nodes. Perform a CT scan of the head and neck with contrast to assist with delineation of cartilage and bone invasion, lymph node metastasis, and extralaryngeal invasion. As a single modality, this is generally more useful for staging hypopharyngeal cancers.
MRI provides no clear superiority to CT scan in all cases. MRI (with gadolinium) is better for delineating soft tissue extension, while CT scan (with bone windows) is better for delineating bone invasion. MRI is most often used to study lesions that suggest submucosal spread toward the esophagus on CT scans.
-
PET scan: The role of PET scanning is emerging in initial assessment of patients with head and neck cancer, especially those with locally advanced disease, nodal involvement (particularly when MRI or CT scan findings are equivocal), suspicion of metastatic disease, or for evaluation of an unknown primary site. The use of fluorodeoxyglucose positron emission tomography (FDG-PET) has been demonstrated to be useful in staging head and neck carcinomas, including squamous cell carcinoma of the hypopharynx. FDG-PET may improve pretreatment staging, identification of an occult primary site, estimation of treatment response, and differentiation of early recurrence from scar tissue.
Integrated PET/CT overcomes poor anatomic localization of PET together with the morphologic data revealed by CT.
PET/CT is helpful in locating and localizing occult primary and regional disease and differentiating between malignant disease and posttreatment changes.
-
Abdominal CT scan: If alkaline phosphatase and gamma-glutamyltransferase (GGT) levels are elevated, consider an abdominal CT scan to rule out liver metastases.
-
Bone scan: If alkaline phosphatase levels are elevated and GGT levels are normal, consider a bone scan to rule out bone metastases.
Other tests
Perform an ECG because a high incidence of cardiovascular disease exists in this patient population.
A full dental evaluation is required before radiotherapy is initiated. This step is critical because of xerostomia caused by radiotherapy, which can lead to dental decay and osteoradionecrosis. Nonrestorable teeth should be extracted, and fluoride trays should be made. If teeth are extracted, include a healing period of 10-14 days before initiating radiotherapy. Good dental and oral hygiene should be emphasized during and after radiotherapy.
If a partial laryngeal surgery is being considered as part of the management plan, pulmonary function tests should be obtained.
Diagnostic procedures
See the list below:
-
Biopsy is necessary to establish the diagnosis. It is usually performed during a triple endoscopy.
-
An examination under anesthesia is critical for obtaining a biopsy and defining the anatomic extent of disease, particularly the superior and inferior extent, as well as the involvement of the prevertebral fascia. Posterior pharyngeal wall lesions are better visualized using direct laryngoscopy.
-
Triple endoscopy, also known as panendoscopy, can be used to assist in defining the inferior extent of the tumor (ie, involvement of the esophageal inlet) and to look for skip lesions and second primary tumors. However, it can be controversial. The necessity of triple endoscopy is being debated; an integrated PET/CT may obviate the need for triple endoscopy. The use of triple endoscopy is based more on symptoms. Esophagoscopy can be difficult to perform if the tumor is large and has caused significant stenosis. In addition, in the absence of findings or symptoms, routine bronchoscopy may not be cost effective.
It is an operating room procedure, performed by an otolaryngologist surgeon.
With the patient under mask general anesthesia, the entire oral cavity and throat are palpated and visually inspected, including direct-vision laryngoscopy. The extent of the tumor can be most accurately ascertained in this manner.
Biopsies of all suspicious lesions are taken. Bronchoscopy and esophagoscopy are performed to rule out synchronous cancers.
Multiple synchronous pharyngeal tumors can be found in approximately 15% of cases.
Synchronous lung or esophageal tumors can be found in approximately 5-10% of cases.
Histologic findings
Most hypopharyngeal cancers are squamous cell neoplasms. Nearly 100% of head and neck cancers overexpress epidermal growth factor receptor (EGFR), although the clinical significance is still unclear. Sarcomas, plasmacytomas, non-Hodgkin lymphomas, and metastatic lesions can be encountered in rare instances.
Histologic factors that denote a higher risk tumor include lymphovascular invasion, perineural invasion, or poorly differentiated cell morphology.
Staging: T stage and risk of nodal disease
Summation of examination and radiographic findings into prognostic categories, using the American Joint Committee on Cancer (AJCC) designations of tumor (T), nodal (N), and metastatic (M) categories, assists in treatment selection and planning.
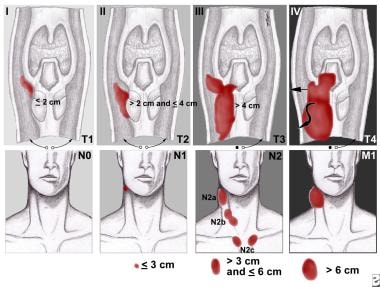
The staging of primary hypopharyngeal tumors is as follows (see image below):
See the list below:
-
TX: The primary tumor cannot be assessed.
-
T0: No evidence of primary tumor is present.
-
TIS: The tumor is carcinoma in situ.
-
T1: The tumor is limited to one subsite of the hypopharynx and is 2 cm or less at its greatest dimension.
-
T2: The tumor involves more than one subsite of the hypopharynx or an adjacent site or is larger than 2 cm but not larger than 4 cm at its greatest diameter without fixation of the hemilarynx.
-
T3: The tumor is larger than 4 cm at its greatest dimension or involves fixation of the hemilarynx.
-
T4: In 2003, the sixth edition of the tumor, node, metastasis (TNM) classification introduced a subdivision of T4 into T4a (low risk) and T4b (high risk) to reflect the probability of a reasonable opportunity for disease control (T4a) compared with a near certainty of a poor outcome (T4b).
T4a – The tumor invades the thyroid/cricoid cartilage, hyoid bone, thyroid gland, esophagus, or central compartment soft tissues, including prelaryngeal strap muscles and subcutaneous fat.
T4b - The tumor invades the prevertebral fascia, encases the carotid artery, or involves mediastinal structures.
The staging of the regional lymph nodes is as follows:
-
NX: The regional lymph nodes cannot be assessed.
-
N0: No regional lymph node metastasis is present.
-
N1: Metastasis is found in a single ipsilateral node (≤ 3 cm at its greatest dimension).
-
N2: Metastasis is found in a single ipsilateral lymph node (>3 cm but < 6 cm in greatest dimension) or in multiple ipsilateral lymph nodes (none >6 cm at greatest dimension).
N2a - Metastasis in a single ipsilateral lymph node (>3 cm but < 6 cm at its greatest dimension)
N2b - Metastasis in multiple ipsilateral lymph nodes (none >6 cm at greatest dimension)
N2c - Metastasis in bilateral or contralateral lymph nodes (none >6 cm at greatest dimension)
-
N3: Metastasis is found in a lymph node larger than 6 cm at its greatest dimension.
The staging of distant metastasis is as follows:
-
M0: No distant metastasis is present.
-
M1: Distant metastasis (eg, lung, mediastinal lymph nodes, skeletal, hepatic) is present.
Table 1. Hypopharyngeal Cancer Staging (Open Table in a new window)
Stage |
Grouping |
||
Stage 0 |
TIS |
N0 |
M0 |
Stage I |
T1 |
N0 |
M0 |
Stage II |
T2 |
N0 |
M0 |
Stage III |
T3 |
N0 |
M0 |
T1 |
N1 |
M0 |
|
T2 |
N1 |
M0 |
|
T3 |
N1 |
M0 |
|
Stage IVA |
T4 |
N0 |
M0 |
T4 |
N1 |
M0 |
|
Any T |
N2 |
M0 |
|
Stage IVB |
Any T |
N3 |
M0 |
Stage IVC |
Any T |
Any N |
M1 |
Risk of nodal disease based on T stage is as follows:
-
T1 - Risk of nodal disease 60%
-
T2 - Risk of nodal disease 60-70%
-
T3 - Risk of nodal disease 84%
-
T4 - Risk of nodal disease 84%
Anatomy
The hypopharynx, or laryngopharynx, is the longest and most inferior portion of the 3 segments of the pharynx and links the oropharynx to the esophagus (see images below). It is located posterior to the cartilaginous structures of the larynx. It is wide superiorly and progressively narrows toward the level of the cricopharyngeal muscle. The hypopharynx is a continuous area; the oropharynx is above it and the cervical esophagus through the cricopharyngeal sphincter is below it. This region is known as the pharyngoesophageal junction or postcricoid area. It is bounded anteriorly by the posterior face of the cricoid cartilage. The hypopharynx extends from the hyoid bone to the cricoid cartilage and is further subdivided into the regions of the pyriform sinus, pharyngeal wall, and posterior cricoid.
The hypopharynx is the longest of the 3 segments of the pharynx. It is wide superiorly and progressively narrows toward the level of the cricopharyngeal muscle. It is bounded anteriorly by the posterior face of the cricoid cartilage. The parts of the hypopharynx that lie partly to each side of the larynx form the pyriform sinuses or fossae.
See the list below:
-
Pyriform sinuses: The parts of the hypopharynx that lie partly to each side of the larynx form the pyriform sinuses or fossae, so named for their pear shape. The pyriform sinuses are bound laterally by the thyroid cartilage and medially by the lateral surface of the aryepiglottic fold, arytenoids, and cricoid cartilages. It is posteriorly open. The apex, or most inferior extent, lies below the vocal cords and, occasionally, below the cricoid cartilage. The superior extent is bordered by the pharyngoepiglottic mucosal fold that extends from the lateral pharyngeal wall to the epiglottis. The pyriform sinuses extend from the glossoepiglottic folds to the upper esophagus.
-
Posterior pharyngeal wall: The posterior pharyngeal wall extends from the level of the hyoid bone to the inferior aspect of the cricopharyngeus muscle. It is formed by the constrictor muscles and is in direct contact with the prevertebral fascia.
-
Pharyngoesophageal junction (postcricoid area): The posterior cricoid area is the posterior surface of the larynx and extends from the arytenoids to the inferior edge of the cricoid cartilage and beginning of the esophagus. The superior laryngeal nerve lies deep to the mucosa of the lateral wall of the pyriform fossa. The constrictor muscles, covered with mucous membrane, form the posterior wall of the hypopharynx. It extends from the level of the floor of the vallecula to the level of the cricoarytenoid joint. The anterior wall of the hypopharynx is bounded by the larynx.
The pharyngeal plexus of nerves, which receives contributions from the glossopharyngeal and vagus nerves, supplies the innervation of the hypopharynx. The vagus nerve supplies motor innervation to the constrictors. Sensory information from the hypopharynx travels along the glossopharyngeal nerve and the internal laryngeal branch of the superior laryngeal nerve, which arises from the vagus nerve.
The primary lymphatic drainage of the hypopharynx includes the jugulodigastric lymph nodes and middle jugular chains. The spinal accessory and retropharyngeal and paratracheal lymph nodes communicate freely.
The pyriform sinuses are drained by a network of lymphatics, which drain primarily to the upper and middle jugular nodes, posterior cervical nodes, and retropharyngeal lymph nodes. Lymphatics of the posterior wall of the hypopharynx drain to the jugular nodes and retropharyngeal nodes. Postcricoid lymphatics drain to the middle and lower jugular nodes and to the paratracheal nodes. [12]
Table 2. Distribution of Involved Lymph Nodes (Open Table in a new window)
Site |
Submaxillary (Level I), % |
Upper Jugular (Level II), % |
Mid Jugular (Level III), % |
Lower Jugular (Level IV), % |
Pharyngeal wall |
20 |
80 |
40 |
40 |
Pyriform sinus |
0 |
67 |
33 |
7 |
*As found after elective modified neck dissection by Byers et al [13] |
||||
See the list below:
-
In recent years, conformal radiotherapy techniques such as intensity-modulated radiotherapy (IMRT) have placed an emphasis on axial anatomy. An understanding of the axial anatomy is especially important in the accurate delineation of the nodal regions at risk for occult nodal metastasis. The nomenclature used is analogous to the surgical nomenclature used to delineate the nodal groups in the cervical neck. The anatomic delineation of nodal groups in the neck is as follows:
Level I: The posterior border is defined by the posterior edge of the submandibular gland.
Level II: The superior extent is defined by the mastoid tip and the caudal edge of the lateral C1 process. The inferior extent is defined by the cranial edge of the hyoid bone. The lateral edge is bordered by the sternocleidomastoid muscle.
Level III: This cervical nodal group is bordered anterolaterally by the sternocleidomastoid muscle and begins superiorly at the cranial edge of the hyoid bone. The inferior edge is bordered by the inferior edge of the cricoid cartilage.
Level IV: This cervical nodal group is bordered by the sternocleidomastoid muscle, begins at the inferior edge of the cricoid cartilage, and extends to 2 cm superior to the supraclavicular joint.
Level V: This posterior neck chain is defined anteriorly by the posterior edge of the sternocleidomastoid and the scalene muscle. It begins superiorly at the cranial edge of the hyoid bone and inferiorly at the transverse cervical vessels.
Level VI: This nodal group is defined superiorly by the caudal edge of the thyroid gland and inferiorly by the sternal manubrium. It is defined laterally by the medial edge of the sternocleidomastoid muscle and medially by the trachea. It is limited posteriorly by the common carotid artery.
Consensus guidelines for the accurate delineation of the clinical node-negative neck from several cooperative organizations (eg, Danish Head and Neck Cancer Group [DAHANCA], European Organization for Research and Treatment of Cancer [EORTC], French Head and Neck Cancer Group [GORTEC]) are available from the Radiation Therapy Oncology Group.
The intimate association between the hypopharynx and the larynx, oropharynx, and esophagus allows for certain dissemination routes of malignant disease. Pyriform sinus carcinomas may spread submucosally into the posterior wall of the hypopharynx, the postcricoid region, or the aryepiglottic fold. Large tumors also extend up into the paraglottic fat, the pre-epiglottic fat, and the base of the tongue. Tumors that arise from the lateral wall or apex of the pyriform sinus often have already invaded the thyroid cartilage. Lesions of the medial wall of the pyriform sinus may spread along the aryepiglottic fold into the false vocal cord and arytenoid cartilage. Medial wall lesions occasionally invade paraglottic and pre-epiglottic fat. They may also grow posteriorly into the postcricoid region and then cross the midline to involve the contralateral pyriform sinus.
Medical Treatment
Pretreatment Care
Consider the following consultations:
-
Dentist: Repair or extract damaged teeth prior to radiation therapy. The risk of osteoradionecrosis of bone is increased with poor dental hygiene or extractions performed after high-dose radiation. Dental prophylaxis with fluoride is important during and after radiation due to loss of saliva. Bisphosphonates should be used with caution in this population due to the risk of mandibular osteonecrosis.
-
Nutritionist: Malnutrition is common at presentation and worsens following surgery, radiation, or both. At diagnosis, obtain nutritional evaluation and recommendations for ongoing nutrition support and follow-up.
-
Speech/swallowing therapist: Specialists in this field should direct rehabilitation for speech and swallowing function. This can include training in electrolarynx use following laryngectomy, evaluation of posttreatment function (and risk of aspiration) by observation and barium swallow, and mouth and throat exercises to regain coordination of swallowing and phonation.
Consider feeding tube placement if oral feeding is likely to be disrupted by therapy. At least 75% of patients undergoing chemoradiotherapy require a feeding tube. Prophylactic placement is often recommended when a patient is unlikely to be able to complete therapy without nutritional support through a feeding tube. This has several advantages, including minimizing the risk of unnecessary interruptions in the radiotherapy, which can result in reduced efficacy of the radiotherapy. In addition, prophylactic feeding tube placement helps to minimize the weight loss that often occurs before a decision is made during a course of radiotherapy to place a feeding tube.
In recent years, concerns have arisen that the sole reliance on a feeding tube, particularly when placed prophylactically, could contribute to postradiotherapy swallowing difficulties, possibly due to weakness of the swallowing muscles. When a feeding tube is placed, patients should be counseled to continue to swallow as much as possible during treatment and to use the feeding tube as part of a graduated strategy to provide increasing nutritional support with decreasing abilities to maintain a complete oral diet. A nutritionist should direct the choice and amount of tube feedings and supplements.
Emergency tracheotomy may be required in 5-15% of patients.
Chemotherapy, Radiation Therapy, and Combined Therapy
The traditional goal of hypopharyngeal cancer management is to achieve the highest locoregional control with the least functional injury, preserving respiratory function, deglutination, and phonation. In recent years, several new treatment options in the management of head and neck cancers have made this goal easier to achieve. This includes modern conservative surgical approaches that involve robotic assistance and laser dissection and new radiotherapy techniques such as intensity-modulated radiation therapy (IMRT) for increased conformal irradiation, including emerging techniques such as partial larynx radiation and the use of biologic agents such as the monoclonal antibody cetuximab (Erbitux), which specifically binds and prevents the activation of the epidermal growth factor receptor (EGFR). [14]
Despite these new treatment modalities, an optimal treatment strategy for head and neck cancers, including hypopharyngeal cancers, is difficult to determine because no randomized study comparing outcomes following surgery with outcomes following radiation or chemoradiation has been completed. Randomized studies are needed because this study model minimizes the risk of skewed results; for example, if earlier-stage cancers are treated with one treatment approach while advanced-stage cancers are treated with a different approach, the study may incorrectly conclude that the two treatment approaches differ in efficacy. This is commonly a problem with chart review studies from treating institutions because each institution has their bias when selecting particular stages of cancers for particular types of treatment.
As a result, consensus guidelines have been published to guide clinical decisions. These include efforts by the National Comprehensive Cancer Network (http://www.nccn.org/ ). The American Society of Clinical Oncology has also published treatment guidelines for cancers of the larynx, which may be useful for decisions of offering larynx preservation therapy or not. [15]
No single therapeutic regimen offers a clear-cut superior survival advantage over other regimens. Laryngopharyngectomy and neck dissection followed by radiation therapy have been the most frequently used surgical therapies for hypopharyngeal cancers. Combined chemotherapy and radiation therapy directed at the primary tumor are the most common nonsurgical approaches for advanced tumors, either due to a large primary tumor size or the presence of large or multiple lymph node metastasis. Radiation therapy alone can be considered in patients with medical conditions that make the administration of chemotherapy with radiation alone for early tumors without cervical nodal involvement.
The management of hypopharyngeal cancer can be broken down based on stage, as follows:
-
T1/T2 - Radiotherapy alone (commonly 66-70 Gy) or surgery (possibly with postoperative irradiation, depending on the pathology findings). Larynx preservation therapy is typically possible and is strongly favored.
-
T3/T4 (resectable) - Partial or total laryngopharyngectomy, neck dissection, postoperative radiotherapy, or radiotherapy alone with altered fractionation or concurrent chemoradiotherapy or participation in prospective clinical trials.
-
Unresectable or medically unstable - (1) Radiotherapy alone with altered fractionation or concurrent chemoradiotherapy or (2) participation in prospective clinical trials including the study of induction chemotherapy.
Radiotherapy, chemotherapy, and surgical treatment are summarized as follows (see below for further discussion):
-
Radiation therapy
Radiation therapy as a curative treatment is feasible for T1 lesions and small T2 lesions.
If a standard fractionation scheme is used, published experience supports the use of various total doses to the gross tumor ranging from 66-70 Gy with a conventional daily fractionation schedule. A dose of 70 Gy is generally favored. If the tumor involves the postcricoid region or the pyriform sinus, the posterior pharyngeal wall usually receives 50-55 Gy in order to treat the retropharyngeal nodes prophylactically. The nodes in the supraclavicular region usually receive prophylactic radiation to approximately 50 Gy.
Altered fractionation has also been recommended based on the results of a large multi-institutional study conducted by the Radiation Therapy Oncology Group (RTOG). [16] See below. This trial enrolled patients with squamous cell carcinomas of various sites in the head and neck including the hypopharynx. The results demonstrated that both an accelerated schedule using a concomitant boost or a hyperfractionation schedule improved the probability of local-regional cancer control in the head and neck.
This study validated the radiobiologic basis for these altered radiotherapy schedules. For the accelerated schedule, this was based on the hypothesis that a tumor stress response to the radiation would result in an increase in the number of tumor clonogens, hence benefiting from administering the planned total dose of radiation over a shorter treatment time to minimize the additional tumor cells. The basis of the hyperfractionation schedule was to achieve a safer increase in the total radio therapy dose by administering smaller doses per fraction or treatment. To avoid the potential adverse effects of prolonging the overall duration of the radiotherapy as a result of the reduced dose per fraction, twice daily fractions were administered.
While both altered fractionation schedules appear to be superior to conventional daily fractionation schedules, the specific use for hypopharynx cancers must be carefully considered due to the potential for increased side-effects. Of the two schedules found to be superior when compared to once daily fractionation schedules, hyperfractionation is likely to be favored due to the results of a recent large individual patient-based meta-analysis. [17] This meta-analysis demonstrated an improvement in survival and control of the local-regional cancer. Hyperfractionation schedules administer a typical total dose to the gross tumor between of 76.8–79.2 Gy in 64–66 fractions of 1.2 Gy each twice a day with 6 or more hours between treatments.
-
Concurrent chemoradiation
Concurrent chemoradiotherapy is recommended for more advanced but resectable hypopharyngeal carcinomas (for organ preservation indications) and for unresectable indications. As with altered fractionation, the use of concurrent chemoradiation for resectable hypopharyngeal cancers must be carefully considered due to the increased acute toxicities and the potential for late injury to the normal tissues result in compromised organ function.
The basis for this comes from randomized trials including head and neck squamous cell carcinoma (HNSCC) from several tumor sites not restricted to the hypopharynx. A large patient-based meta-analysis [2] demonstrated a small but significant improvement in the overall survival of patients receiving concurrent chemotherapy to radiotherapy alone.
Cisplatin is considered the best agent to use with radiation in the treatment of hypopharyngeal cancer, though published experience with the combination of cisplatin and 5-fluorouracil (5-FU) also exist. It is unclear if the addition of 5-FU increases the treatment benefits compared to cisplatin alone when it is administered together with radiotherapy. As such, these concerns must be balanced with the potential for increased side effects with the addition of 5-FU.
-
Induction chemotherapy followed by radiation therapy alone
Historically, chemotherapy administered before definitive radiotherapy was used to improve on the results of conventionally fractionated radiotherapy alone. This was used for unresectable HNSCC and eventually for the use of resectable HNSCC as it has been observed that HNSCC that demonstrated a very good response to several cycles of induction chemotherapy before radiotherapy was associated with an improved probability for radioresponsiveness and improved overall survival. This lead to several randomized trials determining if induction chemotherapy followed by local-regional therapy, be it surgery or radiotherapy was beneficial or not to local-regional therapy alone. [17]
These trials were not specific for hypopharyngeal cancers alone. However, the general interpretation suggested that induction chemotherapy can reduce the risk of distant metastasis but that overall survival was only modestly improved in patients with unresectable cancer and not in resectable cancers. The use of induction chemotherapy did not improve the control of the local-regional cancer, which remained disappointing. As such, efforts have focused on the study of chemotherapy administered concurrently with radiotherapy (see above) and in recent years, the re-introduction of induction chemotherapy followed by concurrent chemoradiotherapy.
The European Organization for Research and Treatment of Cancer (EORTC) conducted a trial of voice preservation in patients with resectable advanced hypopharyngeal cancer. This study demonstrated that the larynx could be preserved with nonsurgical management without any compromise to the overall survival compared to treatment primarily via surgery.
This trial randomized 194 patients, of which 37% had stage IV disease. Only 3% of patients randomized to induction chemotherapy had stage T4 disease, whereas 23% had stage T2 cancers. Most patients were stage T3. Patients were randomized to surgery followed by postoperative radiotherapy or to induction chemotherapy consisting of cisplatin and 5-FU for a potential maximum of 3 cycles. Patients randomized to this arm were assessed after each cycle of chemotherapy to determine the clinical response. Patients demonstrating either a complete response after 3 cycles went on to receive conventionally fractionated daily radiotherapy. Those who did not demonstrate a favorable response went to have surgery consisting of a total laryngectomy.
The incidence of nodal metastases was high. A complete response was achieved in the primary tumor in more than 50% of the patients randomized to chemotherapy, and 43% had no evidence of disease above the clavicles after chemotherapy.
In 1996, the EORTC published the preliminary results of their trial. Three-year survival rates were significantly better among patients randomized to chemotherapy (57%) compared with immediate surgery (43%). At 5 years, however, the differences were no longer significant. The 5-year survival rate with a functional larynx was 35%. The trial demonstrated a reduction of distant. [18]
Despite the ability for induction chemotherapy to reduce the incidence of distant metastasis, the ability of induction chemotherapy to translate this into a consistent improvement in overall survival, especially in resectable HNSCC including the hypopharynx site, seems to be limited. This raises questions about its role in addition to local-regional therapy with radiotherapy alone. In fact, a large patient-based meta-analysis [2] of the EORTC trial (described above) and of two other larynx randomized trials studying induction chemotherapy in respectable HNSCC would support a lack of improvement in overall survival. In fact, the hazard ratio suggested the potential for an adverse impact on overall survival prompting the authors of the meta-analysis to recommend caution with regards to its routine generalized use.
In recent years, the addition of Taxotere to the standard regimen of cisplatin and 5-fluorouracil has been demonstrated to have increased activity renewing interest in the use of docetaxel /cisplatin /fluorouracil (TPF) induction chemotherapy for locally advanced HNSCC.
The results of a large European trial randomizing patients with locally advanced unresectable stage III and IV HNSCC to TPF vs PF induction chemotherapy for 4 cycles followed by conventionally fractionated radiotherapy were recently reported (EORTC 24971). [19] Approximately 30% of the patients enrolled had a hypopharynx primary site carcinoma. Response was not used to determine if patients could proceed to radiotherapy. Rather, disease progression, inadequate bone marrow function, incomplete resolution of the mucositis, and non-healing dental wounds precluded local-regional radiotherapy.
This study demonstrated an improvement in both the progression-free survival and overall survival. The incidence of distant metastasis was comparable between the two arms.
In summary, induction chemotherapy appears to have a more favorable therapeutic ratio (risk vs benefit) for unresectable HNSCC as compared to resectable HNSCC, including the hypopharynx site. How induction TPF followed by radiotherapy alone compares to concurrent chemoradiotherapy with regards to efficacy for unresectable HNSCC is unclear at this time.
-
Induction chemotherapy followed by concurrent chemoradiation
Several completed and ongoing randomized trials are studying the role of induction chemotherapy to concurrent chemoradiotherapy for both resectable and unresectable HNSCC.
Spanish investigators reported the results of a phase III randomized trial of TPF vs PF induction chemotherapy followed by concurrent chemoradiotherapy for locally advanced resectable and unresectable HNSCC. [20] These investigators demonstrated an improvement in the overall survival only in patients with unresectable HNSCC. This finding is consistent with the findings by Vermorken et al [19] (see above) and would favor the addition of Taxotere in unresectable HNSCC as part of an induction regimen if this is elected. However, these investigators concluded that the role for induction chemotherapy would be significantly aided by the results of ongoing randomized trials evaluating induction chemotherapy followed by concurrent chemoradiation to patients receiving only concurrent chemoradiation.
A US study of TPF vs PF induction chemotherapy followed by concurrent chemoradiation with weekly carboplatin and standard fractionated radiotherapy was recently reported. [21]
This trial randomized 501 patients with both resectable and unresectable locally-advanced HNSCC. Approximately one third of the study patients were enrolled with resectable disease for organ preservation indications.
The incidence of distant metastasis was the same between the two induction chemotherapy arms.
As with the Vermorken study, [19] the addition of Taxotere to the induction chemotherapy regimen improved the overall survival.
-
Postoperative concurrent chemoradiation
The indications for postoperative radiotherapy have been the subject of a number of clinical studies attempting to define risk groups and to identify improvements with the use of postoperative radiotherapy with either altered fractionation or with concurrent chemotherapy. In general, studies have attempted to identify groups of patients with a low, intermediate, or high risk of cancer recurrence.
Determining which risk factors constitute a low and intermediate risk group is controversial. Despite this controversy, investigators from the MD Anderson Cancer Center demonstrated in a prospective trial that patients with an intermediate risk for cancer recurrence who received postoperative radiotherapy had the same local-regional control rates as patients who did not demonstrate any adverse pathologic factors in the resected cancer and who did not receive postoperative radiotherapy. [22] Although patients in this portion of the study were not randomized, the strengths of these observations are that all patients were prospectively treated, observed, or both and that the outcome of the intermediate risk group did not significantly differ from that of the group with no risk factors for recurrence. This observation supports the use of postoperative radiotherapy using daily radiation treatments at a dose of 180-5760 cGy.
In general, patients who present with a positive surgical margin or with nodal extracapsular extension are at a high risk for recurrence. In this group of patients, 2 large randomized clinical trials have demonstrated that patients with these risk factors should receive concurrent chemoradiotherapy with cisplatin (100 mg/m2 on days 1, 22, and 43 of radiotherapy) and that this results in cancer control rates that are superior to those of radiation alone.
In recent years, two significant independent randomized trials randomizing patients with head and neck cancers including hypopharyngeal carcinomas that demonstrated high-risk pathologic features following surgery, to either postoperative radiotherapy or postoperative chemoradiation have been reported. [23, 24] Both trials randomized patients to conventionally fractionated radiotherapy or to the same radiotherapy schedule with concurrent high dose cisplatin (100 mg/m2) for 3 cycles during the radiotherapy. Both of these studies demonstrated that concurrent cisplatin improved both the probability of local-regional disease control and disease-free survival.
While both trials were very similar in design showing benefit in patients with high-risk tumor features on pathologic evaluation, the study eligibility differed. This has contributed to the debate regarding which high-risk features should be considered for concurrent postoperative chemoradiation. [25] In general, patients demonstrating a positive surgical margin (defined as cancer at the mucosal margin) or the presence of nodal metastasis with extracapsular extension (ECE) should be recommended to receive concurrent cisplatin.
Debate exists as to the risk versus the benefit of concurrent chemoradiotherapy for patients with multiple nodal metastasis without ECE or tumors with a close surgical margin typically defined as less than 5 mm.
-
A third randomized trial demonstrated that postoperative radiotherapy should be started as soon as possible after surgery to ensure optimal treatment results. As such, coordination between surgeons and radiation and medical oncologists is critical. [22] This study randomized patients to either conventionally fractionated radiotherapy alone or to an accelerated radiotherapy schedule using a delayed concomitant (twice daily) boost schedule in the final 2 weeks of the radiotherapy schedule. This study demonstrated a nonsignificant improvement in the local-regional disease control and overall survival. These results confirm the importance of time but as they were not statistically significant, formal treatment recommendations with an accelerated fractionation schedule cannot be made.
Radiation Therapy and Combined Therapy
Indications for radiotherapy include the following:
-
Definitive treatment
Resectable cancer for organ preservation
Adequate function of the laryngopharynx
Unresectable cancer
Cancer that involves the prevertebral fascia
Cancer that encases the carotid artery
Indications for postoperative radiotherapy include the following:
-
Primary indications
Positive or close margins (< 5 mm)
T4 tumors
Invasion of cartilage, bone, or soft tissues by the primary tumor
-
Neck indications
Two or more lymph nodes with metastasis
Extracapsular extension
Radiotherapy techniques
Radiotherapy volumes should include the lower nasopharynx, retropharyngeal lymph nodes, oropharynx, hypopharynx, and upper cervical esophagus (see images below). Traditionally, opposed lateral fields have been used to treat volumes that encompass the base of skull and upper cervical lymph nodes. A low anterior neck field was used to irradiate the tracheostoma and lower cervical lymph nodes. A small cord block at the posterior lower corner of the lateral fields was used to ensure that the spinal cord did not overlap.
The hypopharynx is the longest of the 3 segments of the pharynx. It is wide superiorly and progressively narrows toward the level of the cricopharyngeal muscle. It is bounded anteriorly by the posterior face of the cricoid cartilage. The parts of the hypopharynx that lie partly to each side of the larynx form the pyriform sinuses or fossae.
With the advent of intensity-modulated radiation therapy (IMRT) techniques, an increased emphasis on cross-sectional anatomy is required for successful radiotherapy planning. The radiation oncologist must be familiar with the normal primary site anatomy and the location of possible nodal metastasis to outline the regions that require radiation accurately and to determine the sufficient doses. This technique also places a greater onus on the radiation oncologist to understand the mucosal spread pattern, especially at the primary site, which may be under appreciated with cross-sectional anatomic imaging.
The total prescribed doses used for primary radiotherapy are 70-72 Gy. Prescribed doses for postoperative regimens are 60-66 Gy, depending on the pathologic margin status. The dose per fraction in head and neck tumors should be 200 cGy when daily radiotherapy is used alone. Dose reductions to 180 cGy or less (ie, 120 cGy twice a day) can be used if the fractionation schedule is altered or radiation is combined with chemotherapy. When IMRT is used, these doses can be delivered by sequentially reducing the volume of irradiation, as has been done with traditional nonconformal techniques. With this serial cone-down technique, more conventional radiotherapy doses per fraction are used.
The advantages of the IMRT technique, which include a reduction in the risk of permanent xerostomia especially with advanced neck disease, must be balanced with the use of a conformal irradiation technique on a moving target (ie, larynx) and the risk of geographic underdosing of the cancer. The quantification and the direction of laryngeal motion during a course of radiotherapy has not been well described in the published literature.
Alternatively, an attractive, yet still evolving, prescription technique of simultaneously delivering larger doses to specified areas (typically in areas of known gross tumor involvement) has gained popularity. This has been referred to as dose painting, simultaneous modulated accelerated radiation therapy (SMART) or simultaneous in-field boost (SIB). This prescription technique exploits the ability to conform radiation doses not only to avoid normal tissues but also to concentrate them in areas of known cancer involvement.
Typical gross tumor doses that have been simultaneously administered to the gross tumor region have ranged from 210-240 cGy, whereas the areas of potential subclinical involvement can receive doses of 165-200 cGy. This effectively reduces the time needed to deliver a potential curative dose of radiation and has been postulated by many investigators to be a form of accelerated altered fractionation, which has been shown in clinical trials to improve locoregional cancer control rates in the head and neck. However, the optimal dose per fraction utilizing this IMRT prescription technique remains the subject of further study.
This IMRT prescription technique may also increase the risk of late complications, which have traditionally been associated with the use of larger doses per fraction. As such, caution is recommended. This is due to the increased heterogeneous spectrum of dose associated with the IMRT technique. In fact, a well-conducted phase I dose escalation study conducted by investigators at the Medical College of Virginia demonstrated that the maximum tolerated dose using a simultaneous in-field boost technique was 2.36 Gy in 30 fractions for a total dose of 70.8 Gy (Lauve, 2004). Of note, patients with HNSCC of all tumor sites excluding the larynx were enrolled. As such, further caution for the use of dose painting IMRT techniques for the larynx is advised. As such, this technique continues to evolve with further clinical study to define the optimal fraction sizes. Even so, the dose heterogeneity inherent to the IMRT technique should be recognized because it limits comparisons between treatment plans.
Chemoradiation therapy
The European Organization for Research and Treatment of Cancer (EORTC) performed a study in which patients with locally advanced hypopharyngeal cancers were randomized to either (1) receive 2-3 cycles of induction chemotherapy with cisplatin and 5-fluorouracil followed by radiotherapy in responders or (2) undergo surgery followed by radiotherapy. [18] Patients who did not respond to chemotherapy underwent surgery and postoperative radiotherapy. Patients who did not undergo surgery who had residual or recurrent disease after definitive radiotherapy were also offered surgical salvage.
The response rate to chemotherapy was 78%. Treatment failure rates at local, regional, and second primary sites in the immediate-surgery arm (12%, 19%, 16%, respectively) were similar to those in the induction chemotherapy arm (17%, 23%, 13%, respectively). The 3- and 5-year disease-free survival rates were also similar. Patients in the immediate-surgery arm had 3- and 5-year disease-free survival rates of 32% and 27%, respectively. Patients in the induction chemotherapy arm had 3- and 5-year survival rates of 43% and 25%, respectively. However, fewer failures occurred at distant sites in the chemotherapy arm (25%) than in the immediate-surgery surgery arm (36%; P = 0.041). Survival was statistically equivalent between the 2 patient groups. Larynx preservation was possible in two thirds of surviving patients, and survival with an intact larynx was 28% at 3 years.
A recent metaanalysis in Lancet examined 63 trials of local-regional treatment with or without chemotherapy and found a small absolute survival benefit of 4% at 2 and 5 years in favor of chemotherapy. [2] In general, multiple recent studies have shown that concurrent chemoradiation therapy can offer local control and survival rates that are better than those of radiotherapy alone. However, this therapy is associated with increased morbidity and acute adverse effects. Neoadjuvant and adjuvant chemotherapy regimens have not proven beneficial and are still subjects of clinical studies, particularly the use of induction chemotherapy.
Altered fractionation
The Radiation Therapy Oncology Group (RTOG) completed a trial in 2000 that evaluated 1,113 patients with locally advanced head and neck cancer who were randomized to 4 different radiotherapy regimens, as follows:
-
Standard fractionation at 2 Gy per fraction per day, 5 days per week to 70 Gy per 35 fractions for 7 weeks
-
Hyperfractionation at 1.2 Gy per fraction, twice daily, 5 days per week to 81.6 Gy per 68 fractions for 7 weeks
-
Accelerated fractionation with a split at 1.6 per fraction, twice daily, 5 days per week to 67.2 Gy per 42 fractions for 6 weeks, including a 2-week rest after 38.4 Gy
-
Accelerated fractionation with concomitant boost at 1.8 Gy per fraction per day, 5 days per week and 1.5 Gy per fraction per day to the boost field as a second daily treatment for the last 12 treatments
Patients treated with hyperfractionation and accelerated fractionation with a delayed concomitant boost had significantly better local and regional control. The hyperfractionation schedule achieved this by giving twice-daily treatments but at smaller dose per treatment, with each daily treatment 6 hours apart. The smaller doses per treatment allowed a higher total dose to be delivered without an increase in the risk of late complications.
A trend toward improved disease-free survival was observed, but no difference was noted in overall survival after a median follow-up of 23 months. These results were achieved at a cost of increased acute adverse effects but not late effects.
Table 3. Results at 2-Year Endpoints (Open Table in a new window)
Result |
Standard, %
|
Hyperfractionation, %
|
Accelerated Fractionation With Split, % |
Accelerated Fractionation With Boost, %
|
Local control |
46 |
54.4 |
47.5 |
54.5 |
Disease-free survival |
31.7 |
37.6 |
33.2 |
39.3 |
Overall survival |
46.1 |
54.5 |
46.2 |
50.9 |
This randomized trial demonstrated that, in general, the use of altered fractionation, hyperfractionation, and delayed concomitant boost–accelerated radiotherapy schedule is superior to conventional daily fractionation when radiotherapy alone is used. Of the 1,113 patients analyzed and reported on, only 141 patients (13%) had hypopharyngeal cancer. The randomized study stratified patients based on site and considered hypopharyngeal and laryngeal cancers as one group. The results reported have not separately analyzed whether the improvements found when an altered fractionation schedule was used were also seen in the hypopharynx.
Concurrent biologic therapy
In the past 10 years, the development of agents that target components within cancer cells and not normal tissues has been of tremendous interest. The hope is that more cancer-specific therapy that offers the promise of reduced toxicities can be developed.
A very attractive molecular target has been the EGFR, which is a transmembrane protein that appears to be overexpressed in the vast majority of head and neck carcinoma cells. More significantly, preclinical studies in various tumor model systems demonstrated that various favorable cancer therapeutic effects could be achieved when the function of this protein was inhibited. The preclinical models demonstrated that this was due to the integral role of EGFR in mediating signals between the extracellular environment and the cell itself. Studies have demonstrated that inhibiting this protein could arrest cell growth, inhibit tumor vessel growth, enhance chemosensitivity, and enhance radiosensitivity, which is significant in the management of head and neck cancers.
These preclinical studies have led to the development of a host of monoclonal antibodies that have specific binding properties against EGFR. The earliest antibody was referred to as C225 or cetuximab (Erbitux). It has been the subject of a large phase III randomized clinical trial in patients with locoregional advanced head and neck carcinomas, including cancers of the hypopharynx. Bonner and colleagues have recently reported the results of this study. Four hundred twenty-four patients were randomized to receive either radiotherapy alone (traditional 3-field technique) or radiotherapy with weekly Erbitux administration following an initial loading dose before the start of radiotherapy. The overall survival rate was significantly improved with the addition of Erbitux
This improved cure rate appears to be due to an improvement in eradicating the cancer in the head and neck, with no evidence of activity in cancers that may have metastasized. The rate of radiation-induced mucositis was similar between the groups, which was of greater significance. This confirmed the selective-targeting activity of Erbitux. How this regimen compares with more traditional chemoradiotherapy regimens is unknown at this time.
Conclusions
The preferred method of hypopharyngeal carcinoma management remains controversial, with a wide variety of techniques reported throughout the literature. The approach to management requires consideration of the tumor's natural history, the patient's performance status, the extent of disease, and the presence and extent of lymph node metastasis. Surgery and irradiation, either alone or in combination, are the standard therapeutic modalities. Induction and concurrent chemotherapy with radiotherapy have been recently used to prolong survival and to preserve organ function.
Several reports in the literature suggest that surgery offers better results than primary radiotherapy. The recent care evaluation study conducted by Hoffman et al found that the survival rate was best in patients treated with surgery only (50.4%), similar in patients who underwent combined surgery and radiotherapy (48%), and worse in those who received irradiation only (25.8%). [26] However, this was not a randomized study, and selection bias may have been an issue in the choices of treatment. The study also ran from 1980-1992, and advances in treatment have been made since that time.
Results from the community to academic centers also vary. Garden et al from MD Anderson Cancer Center reported on the treatment of early squamous cell carcinoma of the hypopharynx with twice-daily radiotherapy alone. Their results showed 2-year actuarial local control rates of 89% for T1 disease and 77% for T2 disease. The actuarial 2- and 5-year survival rates in all patients (T1/T2) were 72% and 52%, respectively, which appears comparable with the results of surgery. [27]
In late-stage disease, surgery with postoperative radiotherapy appears to offer survival results that are equivalent to those of chemoradiation regimens, according to the EORTC study and Zelefsky et al. [28] Nonsurgical regimens offer patients the opportunity to preserve their larynx. The difficulty is that a preserved larynx does not necessarily equate to a functioning larynx. Long-term dysphagia and the need for a tracheostomy negatively affect quality of life, as does the loss of a laryngeal voice following surgery. For this reason, some centers tend to favor chemotherapy and radiotherapy for T3 lesions that still have reasonably good function and surgical resection followed by postoperative radiotherapy for more advanced primary lesions.
More data on quality of life are needed to compare the overall outcomes of surgical and nonsurgical groups. Chemotherapy and radiation regimens would be more appealing if their acute and chronic toxicities were reduced. Various investigations are ongoing to determine which patients will respond to chemotherapy and radiotherapy, and multiple trials are being conducted with various agents such as amifostine (a radioprotective agent) to reduce acute and chronic toxicities of these combined regimens. Ultimately, the poor overall survival rate of the disease has not changed, and more studies are necessary to find a more efficacious treatment overall.
Metastases
The incidence of bilateral neck disease is 10-20%. Because of the high incidence of lymph node involvement and the risk of contralateral neck disease, bilateral neck nodes should be treated, especially for midline tumors. In patients who present with clinical positive nodal metastasis, contralateral neck treatment in particular should be considered because the risk of occult contralateral neck metastasis may be as high as 25%.
The location of the lymph node metastasis is an important consideration in the treatment of hypopharyngeal cancers. In necks that are clinically negative, the lymphatic drainage is to the cervical nodal groups, with level II and III nodal regions typically involved. In necks that are clinically positive, not only is the risk of occult contralateral neck metastasis increased, but the risk of involvement of level I and V must also be considered because the risk is approximately 10% for these sites. This is likely due to an alteration in the lymphatic flow pattern found in clinically involved nodes, typically in the level II and III regions of the anterior cervical neck. The increased risk of retropharyngeal lymph node metastasis in patients with cervical lymph node metastasis is more significant (as high as 90%) when compared with patients without cervical lymph node metastasis.
This altered lymphatic spread pattern is also influenced by the location of the cancer within the hypopharynx. For cancers that involve the pharyngeal wall, as opposed to the pyriform sinus, the risk of level I and V nodal metastasis appears to be as high as 20%.
Patients with cancers of the hypopharynx, particularly cancers that involve the postcricoid region (with or without extension into the cervical esophagus), are also at an increased risk of paratracheal lymph node metastasis. This risk may be as high as 35% and increases in the presence of cervical nodal metastasis. Treatment for these cancers should be considered in patients with mucosal involvement of the postcricoid region, with or without extension into the cervical esophagus.
Eight percent to 26% of patients present with a second primary tumor that is either synchronous (current) or metachronous (sequential). The secondary malignancies usually occur in the oropharynx, lung, and esophagus. Synchronous primary tumors are rare (7.4%). Metachronous lesions are more common and can occur at a rate of 4-7% per year. Overall, some series report second primary tumors as a cause of death in 16% of patients.
Comorbid Conditions
See the list below:
-
General medical care for comorbid conditions is essential to see the patient through cancer therapy.
-
The head and neck cancer patient population has a high prevalence of tobacco-related and alcohol-related comorbid diseases, including cardiovascular disease, chronic obstructive pulmonary disease (COPD), liver dysfunction, malnutrition, alcohol abuse, and tobacco addiction.
-
If cancer surgery is planned, obtain preoperative medical consultation and perioperative or postoperative care.
-
If radiation is used in therapy, radiation-induced mucositis pain requires therapy, including narcotic analgesics via oral, feeding tube, transdermal, or parenteral routes.
Medications Used to Treat Hypopharyngeal Cancer
Chemotherapeutic agents are used in conjunction with surgery, radiotherapy, or both. Various chemotherapy agents demonstrate single-agent response rates of 15-38%. The platinum compounds, 5-fluorouracil, taxanes, and cetuximab demonstrate radiosensitizing properties, making them logical choices for combination chemoradiotherapy. The optimal combination is not established. The following tables are not in order of preference but include some of the frequently used agents.
Antineoplastic agents
These agents inhibit cell growth and differentiation.
Cisplatin (Platinol)
Cisplatin is a platinum-containing compound that exerts its antineoplastic effect by covalently binding to DNA with preferential binding to N-7 position of guanine and adenosine. It can react with 2 different sites on DNA to cause cross-links. Platinum complex also can bind to nucleus and cytoplasmic protein. A bifunctional alkylating agent, once activated to aquated form in cell, binds to DNA, resulting in interstrand and intrastrand cross-linking and denaturation of double helix.
Adult dosing varies with setting and schedule. Modify the dose based on CrCl. Avoid cisplatin if the CrCl < 60 mL/min. Pediatric dosing has not been established.
Cisplatin is a pregnancy category D drug.
Fluorouracil (Efudex, Adrucil, Fluoroplex)
Fluorouracil is a cycle-specific agent that has activity as single agent and has for many years been combined with the biochemical modulator leucovorin. Fluorouracil has been shown to be effective in an adjuvant setting. It is a classic antimetabolite anticancer drug with a chemical structure similar to endogenous intermediates or building blocks of DNA or RNA synthesis.
5-FU inhibits tumor cell growth through at least 3 different mechanisms that ultimately disrupt DNA synthesis or cellular viability. These effects depend on intracellular conversion of 5-FU into 5-FdUMP, 5-FUTP, and 5-FdUTP. 5-FdUMP inhibits thymidylate synthase (key enzyme in DNA synthesis). 5-FUTP is incorporated into RNA and interferes with RNA processing, and 5-FdUTP is incorporated into DNA, leading to cytotoxic DNA strand breaks. Fluorouracil is useful in symptom palliation for patients with progressive disease.
Adult dosing varies with setting and schedule. Pediatric dosing has not been established.
Fluorouracil is a pregnancy category D drug.
Paclitaxel (Taxol)
The mechanisms of action of paclitaxel are tubulin polymerization and microtubule stabilization, which in turn inhibits mitosis and may result in breakage of chromosomes. In vitro data suggest use as radiosensitizer, with a 38% response rate as a single agent.
Adult dosing varies with setting and schedule. Pediatric dosing has not been established.
Paclitaxel is a pregnancy category D drug.
Methotrexate (Folex, Rheumatrex)
Methotrexate is an antimetabolite that inhibits DNA synthesis and cell reproduction in malignant cells; it can suppress the immune system. A satisfactory response is seen in 3-6 wk following administration. Methotrexate is often used in low weekly doses for palliation; the single-agent response rate is 31%.
Adult dosing varies with setting and schedule. Pediatric dosing has not been established.
Methotrexate is a pregnancy category X drug.
Docetaxel (Taxotere)
Docetaxel is a semisynthetic taxane, a class of drugs that inhibits cancer cell growth by promoting assembly and blocking the disassembly of microtubules, thereby preventing cancer cell division, leading to cell death. It is indicated in combination with cisplatin and 5-fluorouracil for induction therapy of locally advanced squamous cell carcinoma of the head and neck (SCCHN) before patients undergo chemoradiotherapy and surgery.
Adult dosing varies with setting and schedule. Pediatric dosing has not been established.
Docetaxel is a pregnancy category D drug.
Cetuximab (Erbitux)
Cetuximab is indicated for use in combination with radiation therapy to treat patients with squamous cell cancer of the head and neck (SCCHN) that cannot be removed by surgery. It is also approved for monotherapy to treat patients whose head and neck cancer has metastasized despite the use of standard chemotherapy. Cetuximab is a recombinant, human/mouse chimeric monoclonal antibody that specifically binds to the extracellular domain of human epidermal growth factor receptors (EGFR, HER1, c-ErbB-1). Cetuximab-bound EGF receptor inhibits activation of receptor-associated kinases, resulting in inhibition of cell growth, induction of apoptosis, and decreased production of matrix metalloproteinase and vascular endothelial growth factor.
Adult dosing varies with setting and schedule. Pediatric dosing has not been established.
Cetuximab is a pregnancy category C drug.
Antidotes, folic acid antagonists
These agents are used to potentiate effects of 5-fluorouracil.
Leucovorin (Folinic Acid, Wellcovorin)
Leucovorin is a reduced form of folic acid that does not require enzymatic reduction reaction for activation. It allows for purine and pyrimidine synthesis, both of which are needed for normal erythropoiesis. Leucovorin is a derivative of folic acid used only as an adjunct to 5-fluorouracil.
Adult dosing varies with setting and schedule. Pediatric dosing has not been established.
Leucovorin is a pregnancy category C drug.
Surgical Treatment
Indications
An experienced otolaryngologist (head and neck) surgeon working with radiation and medical oncologists in a team approach should direct surgical care of the patient. T1-T2 tumors show similar outcomes with radiation or surgery. The timing of surgery, chemotherapy, and radiation should be determined by the treating physicians based on the staging and clinical features of the tumor. Medical and technical operability needs to be determined by addressing the following questions:
-
Can the whole patient tolerate curative surgery?
-
Can the cancer be resected with clear margins and acceptable morbidity?
A retrospective study by Tassler et al indicated that patients with hypopharyngeal SCC treated initially with surgery (total laryngectomy with pharyngectomy), followed by adjuvant therapy, have better survival outcomes than do those who are treated nonoperatively. [29]
Early hypopharyngeal cancer
Early carcinomas of the hypopharynx are not common. Small lesions, particularly of the lateral or posterior wall, may be amenable to partial pharyngectomy or partial laryngopharyngectomy (PLP). [30] In these cases, radiation may be the therapy of choice, offering better functional outcome and the ability to address occult cervical nodal disease. [3]
Pyriform fossa cancer
Lesions that do not extend into the apex of the pyriform fossa, the posterior wall, or the postcricoid may be resected while preserving the larynx, but extension to the apex or involvement of the postcricoid area indicates advanced (T3 or T4) disease and dictates laryngopharyngectomy. Tumors isolated to the lateral wall of the pyriform fossa may be treated with a partial pharyngectomy and resection of the upper thyroid ala. Extension to the medial wall of the pyriform fossa without vocal cord fixation may be managed with a partial laryngopharyngectomy (PLP).
Postcricoid cancer
Most patients with postcricoid cancer develop symptoms at a later stage of their disease. Thus, tumors in this site are usually large and require a laryngopharyngectomy. Extension into the esophagus necessitates a pharyngoesophagectomy and reconstruction. Paraesophageal and paratracheal lymph node dissection with hemithyroidectomy is usually also indicated.
Posterior wall cancer
Tumors in this site can be localized and may present an opportunity for wide excision through a suprahyoid pharyngotomy. On the other hand, submucosal spread and fixation to prevertebral structures complicate resection. If the involvement of the prevertebral structures is extensive, the patient may not be a suitable surgical candidate.
Various primary surgical options are used to manage hypopharyngeal cancers. These options have the potential to produce favorable local control and functional outcomes in appropriately selected patients.
For T1/T2 lesions, both primary radiotherapy and conservation surgical approaches are often viable choices. Conservation surgery may be precluded in favor of radiotherapy in individuals with poor underlying pulmonary function or poor overall functional status, which prevents them from tolerating minor aspiration in the early postoperative period. Similarly, tumor involvement of certain anatomic subsites (eg, pyriform apex or postcricoid region) may also preclude larynx-sparing procedures and favor radiotherapy. Most T4 lesions and many extensive T3 tumors with poor residual laryngeal function warrant more radical primary surgical therapies.
The absence of functional outcome data that compare conservation surgery with nonsurgical approaches complicates the treatment decision.
Conservation procedures
See the list below:
-
Partial lateral pharyngectomy: Certain smaller tumors confined to the lateral pyriform sinus wall may be completely excised using lateral pharyngotomy and primary closure; this approach provides excellent swallowing outcomes. This is a long-established technique. In a recent series of 30 cases, the 3-year local control rate using this approach was 88.5%. [26, 30]
-
Supraglottic hemipharyngolaryngectomy: Originally described by Ogura et al, this procedure is essentially an extension of the traditional supraglottic laryngectomy to include the pyriform sinus mucosa on one side. [31] It requires the arytenoids and true vocal folds to be mobile and free of tumor. Although high local control rates have been reported for small tumors of the upper pyriform sinus, [32] the broad application of this procedure has been limited by concerns over high recurrence rates for more extensive pyriform lesions.
-
Supracricoid hemilaryngopharyngectomy: A more broadly applicable procedure than the supraglottic hemipharyngolaryngectomy, supracricoid hemilaryngopharyngectomy can be used to safely encompass more extensive T2 pyriform lesions; this procedure involves resection of the entire ipsilateral thyroid ala, true and false vocal fold, preepiglottic space, and arytenoid en bloc. Early decannulation is usually possible, and rates of local control and laryngeal preservation exceed 90%. [33] Although the postoperative course is often marked by a gradual recovery of swallowing ability, more than 90% of patients no longer depended on gastrostomy tube at one year after the operation in the largest published series. [34]
-
Posterior partial pharyngectomy: Occasionally, limited midline posterior pharyngeal wall tumors are amenable to this approach, which involves creating an anterior opening into the vallecula above the hyoid bone. This allows direct exposure and resection of the posterior wall, typically to the depth of the prevertebral fascia.
-
Transoral CO2 laser resection: This approach involves specialized transoral endoscopes with an operating microscope coupled to a CO2 laser. In principle, this approach can be used to excise all hypopharyngeal lesions that are candidates for open conservation surgery, provided that adequate transoral exposure can be obtained. Transoral laser surgery holds the added theoretical advantage of not violating other normal anatomic structures of the anterior neck, as is required for the described open approaches; thus, it promotes better functional outcomes. Although an 87% local control rate has been described using transoral laser procedures in a series of 129 pyriform sinus cancers, [35] these techniques have not been widely adopted, in part because of their technical difficulty and absence of data that fully substantiate functional outcomes that are superior to those of open conservation procedures or nonsurgical therapy.
Radical surgery
Primary surgical procedures that do not spare the larynx are typically reserved for T4a tumors, as well as for some smaller tumors in which laryngeal function after primary chemoradiotherapy is expected to be poor. In contrast, small lesions that involve the pyriform sinus apex or postcricoid region may require total laryngectomy for surgical cure and are thus deemed better candidates for nonsurgical therapy to attempt organ preservation.
A study by Cho et al indicated that partial laryngopharyngectomy is as effective as total laryngopharyngectomy in the treatment of cartilage invasion in patients with hypopharyngeal squamous cell carcinoma (SCC). In the study, 28 patients with thyroid or cricoid cartilage invasion by hypopharyngeal SCC underwent the partial or total procedure, with no significant difference in disease recurrence between the two groups (58.3% vs 50.0%, respectively). Moreover, partial laryngopharyngectomy was not found to decrease the 5-year disease-free and disease-specific survival rates compared with the total procedure. Decannulation was possible in nine of the 12 patients who underwent the partial surgery (75%), with the decannulated patients retaining intelligible speech. About 43% of the partial laryngopharyngectomy patients received gastrostomy tubes, compared with just 6.2% of the total surgery group. [36]
Individuals who require total laryngectomy with limited partial pharyngectomy may be amenable to primary closure with good swallowing function; however, pedicled or free-tissue transfer is often required to achieve pharyngeal closure. Likewise, tumors that require total laryngopharyngectomy invariably require free-tissue transfer for successful, if imperfect, restoration of swallowing function.
Reconstruction is often accomplished using pectoralis major pedicled myocutaneous flaps for smaller partial pharyngectomy defects. Larger defects can be reconstructed either free-tissue transfer of jejunum or various tubed fasciocutaneous free flaps (eg, radial forearm or anterolateral thigh). Gastric pullup techniques may be required to reconstruct excisions that produce long esophagectomy defects that are required to control extensive inferior submucosal extension.
A national study in England, by Nouraei et al, of patients treated with laryngopharyngectomy for laryngeal and hypopharyngeal cancers, found lower mortality rates for patients who underwent pharyngeal reconstruction with radial forearm or anterolateral thigh flaps than for those whose reconstruction involved jejunum flaps. The inhospital mortality rate for the pharyngolaryngectomy patients was 6% but reached 11% in those who underwent gastric pullup. Patients had a 5-year survival rate of 57%. [37]
In 2011, Professor Alex Seifalian et al of the University College of London produced the first completely synthetic trachea. Made of nanocomposite material, the synthetic trachea was transplanted into a patient whose own windpipe was damaged by cancer. [38] The operation was performed in Sweden at the Karolinska University Hospital in conjunction with the Karolinska Institute.
The synthetic windpipe’s wide and porous surface area allowed the stem cells taken from the patient's bone marrow and lining cells from the nose to be seeded with the patient's tissue. Within days, a synthetic windpipe, which essentially was the patient’s own, was created in a revolving bio-reactor and then transplanted into the patient. This technique allows the patient to provide the stem cells to create the new trachea, avoiding a long waiting period to find a donor and eliminating the need for anti-suppressant drugs that other transplant patients must take.
Contraindications
Some surgeons consider prevertebral musculature or c-spine involvement, massive mediastinal nodal enlargement, and carotid artery involvement to be contraindications to surgery. These cases usually represent advanced and aggressive disease.
Preoperative details
Prior to treatment, the risks and benefits of treatment options should be frankly discussed with the patient. In cases of hypopharyngeal cancer, this should specifically address possible severe swallowing and speech dysfunction. A speech language pathologist should evaluate the patient before treatment. Before a treatment option is chosen, the patient's psychosocial factors should be considered.
Surgical therapy
See the list below:
-
Partial laryngopharyngectomy (PLP) for tumors of the medial pyriform sinus
Selected patients without pyriform sinus apex involvement may be treated with PLP. Involvement of the apex of the pyriform sinus, extensive submucosal spread, and deep invasion of the lateral pyriform sinus wall are contraindications for this procedure.
The operation is an extension of the supraglottic laryngectomy and involves the combination of suprahyoid and lateral pharyngotomy approaches. Interarytenoid and aryepiglottic cuts allow excision of the ipsilateral arytenoid and pyriform sinus, with cuts similar to those of a supraglottic laryngectomy on the contralateral side.
-
Near-total laryngopharyngectomy
Near-total laryngopharyngectomy preserves one uninvolved arytenoid with a portion of the thyroid cartilage, recurrent laryngeal nerve, and a thyroarytenoid muscle to allow creation of a mucosa-lined tracheoesophageal shunt for voice. Breathing is facilitated with a tracheostomy.
Near-total laryngopharyngectomy can be considered in patients with T2 and T3 lesions of the pyriform sinus in whom total laryngectomy is contemplated.
Near-total laryngopharyngectomy involves an en bloc resection of the paralaryngeal space, including the ipsilateral cricoid. Conservation procedures preserve the cricoid ring, but, in the case of pyriform apex involvement, resection would require stripping the mucosa off the cricoid, which prevents an en bloc resection. Similarly, pyriform sinus cancers cause early vocal cord fixation due to paralaryngeal space invasion. Thus, vocal cord fixation is not a contraindication to a near-total laryngopharyngectomy.
The resected specimen from a near-total laryngopharyngectomy includes the entire hemilarynx from the base of the tongue to the trachea, the pyriform sinus, and part of the posterior pharyngeal wall, if indicated. If the resulting defect requires reconstruction with a flap, near-total laryngectomy can still be performed. The remaining contralateral posterior glottic tissues are reconstructed to form a semirigid glottic shunt to allow phonation and effective swallowing.
Reconstruction of the pharyngeal defect with a skin graft or myocutaneous flap is usually necessary to prevent pharyngeal stenosis.
Near-total laryngopharyngectomy is not recommended for patients in whom radiation treatment has failed or those with postcricoid or interarytenoid tumors, bilateral cord fixation, tumors approaching the midline posteriorly, and bilateral palpable nodes.
-
Total laryngopharyngectomy (see image below)
See the list below:
A total laryngopharyngectomy involves surgical ablation of the larynx, hypopharynx, and upper cervical esophagus.
The commonly accepted indications for this procedure include hypopharyngeal carcinoma or laryngeal carcinoma that involves the hypopharynx.
-
Total laryngopharyngectomy with esophagectomy
Another procedure for more advanced-stage hypopharyngeal or laryngeal tumors is total laryngopharyngectomy with esophagectomy. This procedure involves the removal of the larynx, circumferential hypopharynx, and varying lengths of the esophagus.
Lesions that involve the cervical esophagus, postcricoid area, large areas of the pyriform sinus, and posterior pharyngeal wall with larynx are resected, which leaves a circumferential defect.
-
Extended total laryngectomy for tumors of the pyriform sinus
For hypopharyngeal tumors that are too large for conservation procedures, extended total laryngectomy allows resection of the larynx and pharynx, often with preservation of 3 cm of residual mucosa. This residual mucosa allows primary closure of the pharynx without the need for tissue transposition. If insufficient mucosa remains, pedicled or free tissue transfer patch flaps may be inset into the defect site for reconstruction.
The tendency for submucosal spread of hypopharyngeal tumors mandates wide margins, and primary closure is often not possible. These procedures often require free tissue transfer for closure (see image below).
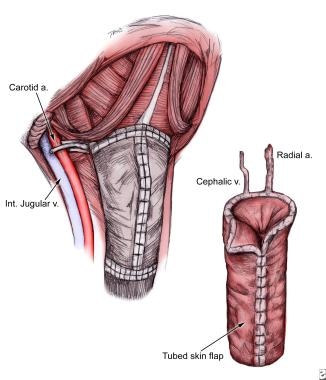 The tendency for submucosal spread of advanced hypopharyngeal tumors mandates wide margins, and primary closure is often not possible. These procedures often require free tissue transfer for closure.
The tendency for submucosal spread of advanced hypopharyngeal tumors mandates wide margins, and primary closure is often not possible. These procedures often require free tissue transfer for closure.
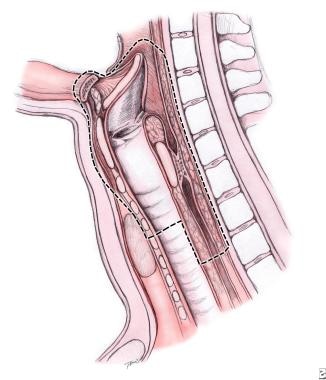

Hypopharyngeal tumors metastasize to the neck early. This is most likely in pyriform fossa tumors and least likely in postcricoid tumors. Bilateral neck metastasis may develop because of rich submucosal lymphatics, which cross the midline. In addition, many patients who have no clinical findings for the neck are found to harbor occult metastasis. Because of the high incidence of clinically positive nodes with hypopharyngeal carcinoma, treating both neck nodes at the time of treatment of the primary tumor is prudent. The site and stage of the patient's tumor and the method of treatment of the primary disease dictate the mode of treatment for the neck.
Follow-up and Complications
Further inpatient care
Initial studies suggested that secondary chemoprevention with 13-cis -retinoic acid (Accutane) showed promise in reducing the risk of second primary cancers; however, more recent long-term follow up of a randomized trial showed no benefit.
Further outpatient care
See the list below:
-
Smoking cessation is associated with improved response to radiation, improved survival, and lower risk of second primary cancers.
-
Close monitoring is required during radiation, chemotherapy, or both for evaluating tumor response, management of adverse effects, nutritional support, pain medications, and psychosocial support.
-
Reevaluate the disease status periodically due to high risk of recurrence. Perform a neck examination and fiberoptic laryngoscopy every 1-3 months for 1-2 years after the initial treatment and 2-4 times per year thereafter. If PET scan was informative at initial diagnosis, consider repeating not sooner than 4 months after radiation or surgery; prior to this time, the inflammation from treatment may give a false-positive reading.
-
Monitor for second primary cancers (incidence of approximately 3% per y) once or twice per year.
Chest x-ray films for detection of lung cancer or metastases
Hepatic panel to check for liver metastases
Oral examination, neck examination, and fiberoptic laryngoscopy to check for new oral or throat lesions
Thyroid-stimulating hormone (TSH) levels once or twice per year if neck was radiated
-
Dental monitoring is important following radiation to the neck, due to xerostomia and increased risk of tooth decay. Careful attention to cleaning, scaling, periodontal health, and lifelong topical fluoride treatment can reduce the risk of tooth loss.
Complications
Radiotherapy and chemotherapy complications
Chemotherapy complications include infection due to myelosuppression, alopecia, nausea and vomiting, peripheral neuropathy (taxanes, platinum drugs), and increased skin and mucous membrane damage from radiation.
Several factors can influence the side effects of radiation, including the fractionation schedule, the use of conformal techniques such as intensity-modulated radiation therapy (IMRT), and the concurrent use of chemotherapy or biologic therapy. Adverse effects that occur during irradiation should be regarded separately from those that persist following completion of treatment. Careful patient counseling is an important aspect in the successful delivery of head and neck radiotherapy and cannot be overstated.
Acute toxicities during irradiation, a constellation of adverse effects, can occur, beginning with taste alteration that may develop as early as the first week of treatment. This side effect is important to recognize because it can have a detrimental effect on a patient's appetite and oral intake early in the course of treatment, and weight loss may result. Avoiding such weight loss helps to ensure that good head and neck immobilization is maintained during the course of treatment.
Radiation-induced injury to the mucosa that causes erythema and ulceration results in pain and difficulty in swallowing and can begin as soon as the second or third week of treatment, occurring even earlier with the use of concurrent chemotherapy. As such, pain management is an important aspect in the care of patients during a course of head and neck radiotherapy. This is especially important given the significant body of scientific evidence demonstrating that treatment interruptions can result in poor treatment outcomes. Proper counseling and close attention to pain management are hallmarks of successful head and neck radiotherapy.
The severity of the radiation mucositis increases with the concurrent administration of chemotherapy; the severity varies depending on which chemotherapy agents are used. Severity is also influenced by the dose of radiation delivered daily. Using standard 3-field radiotherapy fields, the use of hyperfractionation or accelerated radiotherapy increases the severity of the mucositis. Similarly, increased mucositis can develop if IMRT techniques are used and larger doses per treatment are simultaneously delivered to areas of the cancer (ie, dose painting).
With progressive accumulated doses of irradiation, the quality and amount of salivary secretions changes. Patients typically describe a thick, tenacious, yet copious, amount of secretion that is difficult to clear. To some extent, this may be minimized with antitussants and antihistamines. Despite the use of these agents, the reduction in secretions may be suboptimal in patients and poses an increased risk of aspiration pneumonia due to the difficulties in clearing the secretions within the upper airway. This is further compounded by the radiation mucositis in the laryngopharynx, which functions to coordinate swallowing function around the larynx. The risk of serious pneumonia is high in patients who receive concurrent chemotherapy and who may become neutropenic. Serious pneumonia is the single greatest risk of treatment-related death. Treatment-induced fatigue is also increasingly seen with the use of concurrent chemotherapy.
Radiation-induced mucosal edema can occur with radiotherapy and is increased with concurrent chemoradiotherapy. When the laryngopharynx is irradiated, as in the treatment of hypopharynx cancers, the increased edema can also exacerbate swallowing difficulties. For these reasons, the use of percutaneous gastrostomy tubes in patients receiving concurrent chemotherapy should be considered. Although beneficial in minimizing weight loss and adverse nutritional consequences, concurrent chemotherapy may exacerbate the risk of long-term swallowing difficulties by discouraging patients to continue attempting to swallow. A gastrostomy tube should be properly viewed as a mechanism for ensuring sufficient nutrition, and, when possible, patients should be encouraged to swallow.
Following completion of head and neck radiotherapy, the vast majority of these side effects gradually resolve during the following 1-2 months, with the radiation-mucositis quickly improving if no concurrent chemotherapy is delivered. Concurrent chemotherapy may require additional time for recovery. With concurrent Erbitux administration, the mucositis recovery rate in patients receiving chemotherapy is similar to that in patients receiving radiotherapy alone. This is consistent with the selective targeting of cancer cells associated with this agent.
Despite the use of conformal techniques such as IMRT, patients continue to describe a sense of xerostomia within the first several months of completing head and neck radiotherapy. Patients treated with parotid-sparing techniques have greater amounts of salivary flow, which is also inducible, compared with patients treated with the traditional 3-field arrangement. The use of parotid-sparing techniques also increases the probability of further recovery of parotid function, which may require a period of 6-12 months following completion of the radiotherapy. Similarly, taste alteration typically resolves months after the completion of radiotherapy, with recovery variable.
Late toxicities
Late toxicities may include radiation-induced hypothyroidism, which is easily managed with thyroid-replacement therapy. This can often be identified using routine blood analysis, and replacement therapy can be initiated prior to the development of symptoms.
The addition of concurrent chemotherapy poses the potential for an increased risk of persistent laryngopharyngeal edema. This can result in an increased risk of ongoing swallowing difficulties, necessitating a permanent gastrostomy tube. However, in a large randomized trial of larynx cancers conducted by the Radiation Therapy Oncology Group (RTOG 9111), the risk of swallowing difficulties was 15%, the same as in the group receiving radiotherapy alone (14%). This study did not include hypopharyngeal cancer but did expose an almost identical region for irradiation. The probability of complete inability to swallow was less than 5%, the same as in patients treated with radiotherapy alone.
Similarly, in the large randomized trial of altered fractionation (RTOG 9003), the magnitude of late swallowing difficulties between conventional once-daily fractionation and hyperfractionation or accelerated fractionation with the concomitant boost technique also appeared to be similar. Severe swallowing difficulties were also reported to be less than 5% in all groups, despite the fractionation. The use of concurrent chemotherapy and altered fractionation likely increases the risk of swallowing difficulties and severe complications, requiring a permanent gastrostomy tube. The significance of the difference in these large randomized trials is limited by the small number of patients who developed serious swallowing difficulties. Patients need to be appropriately counseled that this complication is possible.
With the advent of parotid-sparing radiotherapy, such as IMRT, the incidence of late swallowing difficulties is likely reduced because of the preservation of parotid function. With salivary flow, the food bolus is lubricated. In addition, the use of the IMRT technique allows for careful limits to be placed on critical anatomic structures involved in the swallowing mechanism. Ongoing studies are examining whether the risk of late swallowing dysfunction can be reduced.
Other rare late, but potentially serious, consequences of radiation injury may include laryngeal chondronecrosis, laryngeal strictures, brachial plexus injury, and the possibility of spinal cord injury.
See related CME at Treatment Options for Esophageal Strictures.
Surgical complications
Certain factors, such as prior radiation therapy, poor general health, chronic malnutrition, alcoholism, diabetes mellitus, advanced age, and systemic illness, all increase the chance of surgical complications.
Intraoperative complications may include hemorrhage, carotid sinus reflux, and damage to cranial nerves. Unilateral resection of the hypoglossal nerve is usually well tolerated without serious sequelae; however, bilateral hypoglossal nerve resection causes severe disability with serious difficulties in feeding, swallowing, and speaking. Resection of the vagus nerve, which carries motor and sensory branches to the larynx and pharynx, causes vocal cord paralysis.
Damage to the accessory nerve causes denervation of the trapezius muscle, which is one of the most important shoulder abductors. Damage to the accessory nerve also causes destabilization of the scapula, with progressive flaring of this bone at the vertebral border. Injury to the brachial plexus and phrenic nerve are complications that should be avoided with proper identification of anatomic planes.
Postoperative complications are not uncommon after extensive head and neck surgery. In the immediate postoperative period, the patient is at greatest risk for pulmonary embolism, gastric ulceration, hemorrhage, and aspiration pneumonia. Other more specific early complications include infection, fistula formation, and subsequent mediastinitis. The most common complication of surgery is pharyngocutaneous fistula after pharyngectomy. The incidence of fistula varies based on the type of reconstruction and the extent of the primary lesion. Other complications can include carotid rupture (< 1% without prior radiotherapy) or pharyngeal stenosis (3-15% following a jejunal free flap reconstruction of a total laryngopharyngectomy). The surgical mortality rate varies from 1-2%. The fistula rate remains the same with preoperative radiation; however, the time required to heal a fistula is significantly greater for the irradiated hypopharynx. The need for operative intervention with complex flaps also increases.
When a fistula or infection in the neck is detected, the wound should be opened widely and packed. The tract should be diverted away from the carotids and microvascular pedicle.
Later complications include pharyngoesophageal stenosis and stricture. A stricture that causes dysphagia may develop some weeks or months after surgery or after radiotherapy is complete. Other late complications include chronic pharyngocutaneous fistula and functional deficits in swallowing.
Outcome and Prognosis
Hypopharyngeal cancers generally have a poorer prognosis than do other head and neck subsites, partly related to frequent late-stage presentation. In general, the overall 5-year survival is reportedly 20-47%. Patients in whom lesions are detected early and who have negative nodes have 5-year survival rates higher than 70%. [39] Most cases are, however, advanced, and the overall survival rate rarely exceeds 25% in any series. Postcricoid carcinomas and pyriform apex lesions fare more poorly than superiorly based pyriform sinus lesions. General local control rates have been reported to be around 80%. Hoffman et al performed a survey to identify demographics and standards of care for the treatment of hypopharyngeal squamous cell carcinoma in the United States. Of 2939 cases analyzed, they found that the overall 5-year disease-specific survival was 33.4%. The disease-specific survival based on stage was 63.1% for stage I disease, 57.5% for stage II, 41.8% for stage III, and 22% for stage IV. [40]
The aforementioned study by Jakobsen et al reported that the overall 5-year survival rate in Denmark for patients with hypopharyngeal cancer was 13.4% between 1980 and 1985, rising to 26.9% for the period from 2010 to 2014. [7]
Distant metastatic disease develops in approximately 25% of patients. The lungs, liver, and bones are the principle organs affected. The principle cause of death is local tumor recurrence. Distant metastases, second primary cancers, and comorbid diseases are secondary causes.
Postoperative irradiation improves the results of surgery. Despite a good local control rate, the 5-year survival rate does not exceed 35%; most patients succumb to distant metastases, intercurrent diseases, or second primaries.
In the past, chemotherapy was used for palliative purposes because of poor outcomes in the treatment of cancer of the head and neck. With the introduction of platinum-based chemotherapeutics, either as a single agent or in combination with other drugs, partial response rates and complete response rates have improved. Of late, concomitant chemoradiotherapy has been show to result in a significant increase in survival.
Altered fractionation radiation has been explored in advanced head and neck cancers. The largest randomized trial was a 4-arm trial carried out by the Radiation Therapy Oncology Group (RTOG 90-03) evaluated the effectiveness of conventional irradiation, a split course accelerated fractionation, delayed concomitant boost and hyperfractionated irradiation.
In this study, only 13% of patients had hypopharyngeal cancers. Both hyperfractionated irradiation and concomitant boost showed significantly better locoregional control, disease-free survival, disease-specific survival, and overall survival.
Importantly, these trials and studies do not specifically address hypopharynx cancers. Thus, this site is rarely studied separately; in case of mixed sites, the hypopharynx represents just a few cases. Little is known about the selection of patients with cancer of the hypopharynx (detailed locoregional extension, performance status), and no information is provided about the possibilities of surgical salvage.
A study by Park et al indicated that up-front surgery can be more beneficial than chemoradiotherapy in discouraging recurrence, but not in improving the overall survival rate, in patients with advanced-stage hypopharyngeal SCC. In a cohort of individuals with stage IVa SCC of the oral cavity, oropharynx, larynx, or hypopharynx, 5-year overall and disease-free survival rates were 64.4% and 62.0%, respectively, for the patients who underwent up-front surgery, and 49.5% and 45.4%, respectively, for those treated with chemoradiation. While, more specifically, surgery did not improve overall survival for the patients with hypopharyngeal SCC, it led to a 49% reduction in the odds of recurrence. [41]
Prognostic factors
See the list below:
-
Age: The survival rate usually declines as the age increases. However, 50% or more of the patients who present when younger than 40 years (1-3%) have stage IV disease.
-
Sex: Women usually present with earlier-stage disease and have a higher survival rate after therapy.
-
Race: African Americans have a higher incidence of hypopharyngeal cancers and a 26% lower survival rate.
-
Karnofsky performance score: Patients with a poor Karnofsky performance score (KPS) usually have poorer outcome due to weight loss, cachexia, malnutrition, and anemia.
-
Tumor-related factors that influence prognosis include the following:
Stage: Increasing T and N stages indicate poor prognosis.
Histology: Pathologic factors such as positive surgical margins or tumor persistence in a radiation field after definitive treatment adversely affect survival.
Location: Aryepiglottic fold and pyriform fossa tumors on the medial wall are usually smaller and more localized and have higher cure rates.
Cross-sectional tumor volume: Several studies have demonstrated an inverse relationship between the primary tumor volume, as assessed with cross-sectional imaging (eg, CT scanning), and local control rates. In several independent studies, this has been more consistently reported in patients treated with radiotherapy but has also been reported in patients who underwent surgery at the primary site.
Future Directions
The future direction of the treatment of hypopharyngeal cancers parallels the development in advances for treating all late-stage head and neck cancers. This is largely due to the difficulties of conducting large clinical trials in patients with cancers of only a single head and neck site. The future is exciting, and many of the future directions previously discussed in this section have been realized.
The introduction of the monoclonal antibody Erbitux has demonstrated that selective drugs can be delivered to head and neck carcinomas without increasing the risk of injuring the mucosa. This offers the possibility of reduced swallowing difficulties. Despite this excitement, understanding how Erbitux administration combined with radiotherapy compares with traditional chemoradiotherapy regimens, especially in combination with high-dose cisplatin delivered every 3 weeks, is important. Clinical trials have demonstrated that traditional chemoradiotherapy regimens affect the risk of late distant recurrences, which is a particularly important pattern of failure in hypopharyngeal cancers.
Bonner and colleagues recently reported the improved survival rates seen with Erbitux administration but did not report any difference in the rate of distant cancer recurrences. [42] Future studies with such EGFR-directed agents will likely seek to answer these questions and to study the combination of Erbitux administration with conventional chemoradiotherapy regimens that incorporate intensity-modulated radiation therapy (IMRT) radiotherapy techniques.
Because the risk of distant cancer relapse is a pattern that is particularly great in patients with hypopharyngeal cancer, future directions, including the incorporation of induction systemic chemotherapy and the incorporation of antiangiogenesis agents (eg, bevacizumab [Avistan]), offer the promise of affecting this pattern of cancer failure.
Continued improvements in conservative surgical techniques using robotic assistance allow for the potential for further surgical resection to be performed with less swallowing morbidity. This technique holds the promise of further resections without the swallowing difficulties that result from gaining access to the cancer.
In the coming years, further studies with proton radiation, including intensity-modulated proton radiotherapy (IMPT) techniques, are expected to be extended to various head and neck cancers, including the hypopharyngeal cancer. To date, this technology has not been extensively evaluated for use in cancers of the head and neck, other than at the base of skull or in the orbit, because few centers have this technology available for clinical use in the United States. The advantage of this technology is that the exit dose of a particular radiation beam can be dramatically reduced, limiting side effects. The dose delivered to the parotid glands will likely be dramatically reduced, even with current IMRT techniques.
However, improvements in more conformal radiation techniques will continue to be limited by the need to define the extent of cancer spread. Traditional techniques have relied on alterations in the shape, size, and appearance of normal tissues. The increasing use of FDG-PET scans now permits smaller volumes of cancer spread, such as is found in normal-sized cervical lymph nodes, to be identified. This is particularly important for more conformal radiation techniques, in which underdosing areas of the neck that appear otherwise normal is possible. Future developments in additional imaging agents that allow for more specific aspects of cancer to be detected offer the promise of smaller volumes of cancer spread to be detected and greater confidence in the use of conformal irradiation.
Even more exciting is the promise of newer imaging agents and techniques that can be used noninvasively to determine various biologic aspects of the cancer. Examples include the ongoing studies of various agents that bind to areas of tumor hypoxia, which has been shown to increase radiation resistance in head and neck cancers. The ability to tag such agents with radioactive markers allows them to be used as imaging agents, such as has been achieved using the hypoxia marker EF5, which has been shown to be of prognostic significance in head and neck cancers.
Medicolegal Pitfalls
See the list below:
-
In a patient with throat symptoms, inadequate examination (flashlight and tongue blade or mirror examination) may provide false reassurance.
-
Protracted empiric antibiotic therapy for nonresponding earaches, sore throat, or cervical lymphadenopathy can delay diagnosis.
-
Negative office biopsy of suspicious mucosal lesions or fine-needle aspiration of cervical lymph nodes does not rule out malignancy.
Necrotic debris can interfere with pathologic interpretation.
If clinical setting is suspicious, obtain further biopsies.
Guidelines
Head and neck cancer guidelines published in November 2017 by the Spanish Society of Medical Oncology include the following options for hypopharyngeal cancer [43, 44] :
-
Total pharyngo-laryngectomy plus neck dissection, with subsequent radiotherapy or chemoradiotherapy if a high risk exists for pathologic factor recurrence, particularly T4a (ie, tumor invasion of the thyroid/cricoid cartilage, hyoid bone, thyroid gland, oesophagus, and/or central compartmental soft tissue)
-
If the patient refuses surgery, then concurrent chemoradiotherapy with thrice-weekly cisplatin; the use of cetuximab concurrent to radiotherapy is recommended if cisplatin cannot be administered
-
Induction chemotherapy with TPF (docetaxel/cisplatin/fluorouracil) schedule
With the induction chemotherapy option, the guidelines recommend the following:
-
If complete response - Radiotherapy (based on initial stage) ± cisplatin/cetuximab (based on induction chemotherapy toxicity)
-
If partial response - Surgery followed by radiotherapy or chemoradiotherapy; if the main objective is organ preservation, consider concomitant radiotherapy (with cisplatin or cetuximab)
-
If stable disease or progression - Surgery (including neck dissection) followed by radiotherapy or chemoradiotherapy
-
The hypopharynx is the longest of the 3 segments of the pharynx. It is wide superiorly and progressively narrows toward the level of the cricopharyngeal muscle. It is bounded anteriorly by the posterior face of the cricoid cartilage. The parts of the hypopharynx that lie partly to each side of the larynx form the pyriform sinuses or fossae.
-
Hypopharyngeal anatomy.
-
Staging of cancer of the hypopharynx.
-
Patient presenting with hoarseness and dysphagia. CT scan demonstrated bulky right pyriform sinus tumor eroding through thyroid cartilage, with displacement of supraglottic airway. Total laryngectomy would have been required, because the patient placed a high value on retaining the ability to talk, chemoradiotherapy was chosen. Following chemoradiotherapy, note persistent fullness in tumor bed. Endoscopy revealed edema and scarring, but the biopsy was negative for tumor. Continued vigilance is needed in this situation.
-
Patient presenting with hoarseness and dysphagia. CT scan demonstrates bulky right pyriform sinus tumor (white arrows) eroding through thyroid cartilage, with displacement of supraglottic airway. A total laryngectomy would have been required, because the patient placed a high value on retaining the ability to talk, chemoradiotherapy was chosen.
-
Patient presented with hoarseness and otalgia. On MRI, there was a bulky left pyriform sinus tumor with an area of gadolinium enhancement extending to the carotid sheath. This T4 tumor was unresectable, and the patient was treated with chemoradiation. Despite a good response to chemoradiotherapy, the evaluation for progressive neck pain 4 months later revealed a bulky recurrence in the left neck. Note tumor (white arrows) surrounding the carotid artery (black arrow).
-
Right pyriform sinus cancer following laryngeal conservation surgery. Postoperative chemoradiation was indicated for positive neck metastasis and a positive deep margin.
-
Lateral view of tumor cuts for laryngopharyngectomy.
-
The tendency for submucosal spread of advanced hypopharyngeal tumors mandates wide margins, and primary closure is often not possible. These procedures often require free tissue transfer for closure.
-
This figure demonstrates a traditional nonconformal arrangement of 3 fields used to bilaterally treat the hypopharynx and cervical neck nodes.
-
Right pyriform sinus cancer following laryngeal conservation surgery. This figure demonstrates the remaining left cricoarytenoid joint and the importance of minimizing radiation injury in minimizing the risk of swallowing dysfunction and protection of the airway.
-
Axial CT slice demonstrating the conformal distribution of radiation in color wash around the left cricoarytenoid joint, which is receiving 3800 cGy. In contrast, the right resected pyriform sinus with a positive surgical margin is receiving 6600 cGy.
-
This figure demonstrates the residual laryngopharynx after conservative surgery and one month following completion of postoperative chemoradiotherapy. The left cricoarytenoid joint is mobile with minimal treatment edema.
-
This figure demonstrates a patent left pyriform sinus apex one month following postoperative chemoradiotherapy delivered with a conformal intensity-modulated radiation therapy (IMRT) treatment plan. The patient continues to swallow without any symptoms of dysphagia.
-
Patient with left-sided sore throat and neck mass. CT scan demonstrates left pyriform sinus mass (white arrows) and large neck node (black arrow).
-
Patient with left-sided sore throat and neck mass. CT scan demonstrated left pyriform sinus mass and large neck node. Two years after chemoradiotherapy, no evidence of tumor exists.
-
Patient presented with hoarseness and otalgia. Note the bulky left pyriform sinus tumor (black arrow) with an area of gadolinium enhancement extending to the carotid sheath (white arrows). This T4 tumor was unresectable, and the patient was treated with chemoradiation.
Tables
Stage |
Grouping |
||
Stage 0 |
TIS |
N0 |
M0 |
Stage I |
T1 |
N0 |
M0 |
Stage II |
T2 |
N0 |
M0 |
Stage III |
T3 |
N0 |
M0 |
T1 |
N1 |
M0 |
|
T2 |
N1 |
M0 |
|
T3 |
N1 |
M0 |
|
Stage IVA |
T4 |
N0 |
M0 |
T4 |
N1 |
M0 |
|
Any T |
N2 |
M0 |
|
Stage IVB |
Any T |
N3 |
M0 |
Stage IVC |
Any T |
Any N |
M1 |
Site |
Submaxillary (Level I), % |
Upper Jugular (Level II), % |
Mid Jugular (Level III), % |
Lower Jugular (Level IV), % |
Pharyngeal wall |
20 |
80 |
40 |
40 |
Pyriform sinus |
0 |
67 |
33 |
7 |
*As found after elective modified neck dissection by Byers et al [13] |
||||
Result |
Standard, %
|
Hyperfractionation, %
|
Accelerated Fractionation With Split, % |
Accelerated Fractionation With Boost, %
|
Local control |
46 |
54.4 |
47.5 |
54.5 |
Disease-free survival |
31.7 |
37.6 |
33.2 |
39.3 |
Overall survival |
46.1 |
54.5 |
46.2 |
50.9 |

What would you like to print?
- Practice Essentials
- Epidemiology
- Presentation
- Etiology and Risk Factors
- Workup
- Anatomy
- Medical Treatment
- Medications Used to Treat Hypopharyngeal Cancer
- Surgical Treatment
- Follow-up and Complications
- Outcome and Prognosis
- Future Directions
- Medicolegal Pitfalls
- Guidelines
- Show All
- Media Gallery
- Tables
- References








