Practice Essentials
Polygenic hypercholesterolemia is the most common cause of elevated serum cholesterol concentrations. Low-density lipoprotein cholesterol (LDL-C) elevations are moderate (140-300 mg/dL) with serum triglyceride concentrations within the reference range. However, practically speaking, the material in this article is also relevant to patients with mixed dyslipidemias with triglyceride levels of less than 350 mg/dL.
Background
Polygenic hypercholesterolemia is caused by a susceptible genotype aggravated by one or more factors, including atherogenic diet (excessive intake of saturated fat, trans fat, and, to a lesser extent, cholesterol), obesity, and sedentary lifestyle. The involved genes have yet to be discovered. Polygenic hypercholesterolemia is associated with an increased risk for coronary heart disease (CHD), as displayed in the image below.
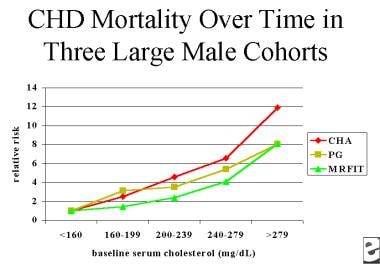 Relative risk of coronary heart disease (CHD) mortality versus baseline serum cholesterol over time in 3 large cohorts of young men. CHA is Chicago Heart Association Detection Project in Industry, PG is Chicago Peoples Gas Company, and MRFIT is Multiple Risk Factor Intervention Trial. Adapted from Stamler, 2000.
Relative risk of coronary heart disease (CHD) mortality versus baseline serum cholesterol over time in 3 large cohorts of young men. CHA is Chicago Heart Association Detection Project in Industry, PG is Chicago Peoples Gas Company, and MRFIT is Multiple Risk Factor Intervention Trial. Adapted from Stamler, 2000.
In the United States, the National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) guidelines are the most commonly used reference for determining therapeutic target LDL-C levels. The guidelines were first published in 1988 (ATP I), [1] with an update published in 2004. [2] The revisions and update have reflected the results of randomized placebo controlled clinical trials that have demonstrated reduced morbidity and mortality in subjects with moderate hypercholesterolemia treated with cholesterol-lowering agents, particularly (though not exclusively) statins. [3]
Pathophysiology
Low-density lipoprotein (LDL) particles are the major plasma carriers of cholesterol. Therefore, in patients with normal or minimally elevated triglyceride levels and average high-density cholesterol levels (HDL-C), the total serum cholesterol measurement can be used as a surrogate for the LDL-C level. Hypertriglyceridemia is caused by excessive numbers of very low-density lipoprotein (VLDL), intermediate-density lipoprotein (IDL), and/or chylomicron particles; and in this situation, the total cholesterol level is not a reflection of the LDL-C level. For a simplified diagram of cholesterol metabolism, see the image below.
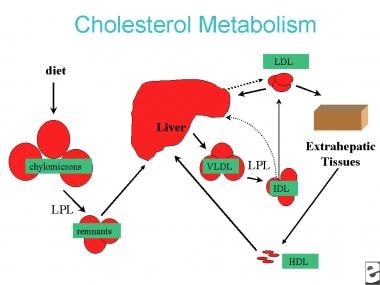 Simplified diagram of cholesterol metabolism. LDL is low-density lipoprotein, VLDL is very low-density lipoprotein, IDL is intermediate-density lipoprotein, HDL is high-density lipoprotein, and LPL is lipoprotein lipase.
Simplified diagram of cholesterol metabolism. LDL is low-density lipoprotein, VLDL is very low-density lipoprotein, IDL is intermediate-density lipoprotein, HDL is high-density lipoprotein, and LPL is lipoprotein lipase.
Elevated LDL-C concentrations may be the consequence of elevated LDL production or decreased LDL hepatic uptake. The liver is responsible for high LDL-C levels, as follows:
-
Overproduction of VLDL particles, which are converted to VLDL remnants or IDL particles by lipoprotein lipase and then to LDL particles by hepatic lipase (which occurs with diet high in triglycerides), or
Familial hypercholesterolemia (FH) is sometimes clinically difficult to distinguish from polygenic hypercholesterolemia unless genetic testing is performed. The presence of mutations in the following genes has most often been studied in the spectrum of familial hypercholesterolemia [8, 9] :
-
Gene encoding the receptor for removal of LDL-C (LDL-R), 93%
-
APOB gene encoding for apolipoprotein B, 5%
-
PCSK9 gene (proprotein convertase subtilisin kexin 9), which codes for protein responsible for degradation of LDL receptor, 2%
A case-controlled study was done in the UK to determine if LDL cholesterol gene score can help differentiate patients with polygenic and monogenic familial hypercholesterolemia. It comprised more than 600 patients with clinical FH and 3,020 control subjects. The study attempted to distinguish patients with polygenic and monogenic FH by genotyping for the 3 known genetic causes above and 12 common LDL-C raising single-nucleotide polymorphisms (SNPs). Only about 50% of patients with clinical FH had monogenic FH, although many were found to have multiple SNPs. Multiple genetic mutations were often found in those labeled as having a polygenic cause. [10]
Some patients with mixed dyslipidemias (elevations of both LDL-C and triglycerides) may have polygenic hypercholesterolemia along with some other condition such as insulin resistance or obesity that causes high triglyceride values.
Epidemiology
United States statistics
The guidelines of the American Heart Association and the NCEP Adult Treatment Panel III (ATP III) define hypercholesterolemia as a blood cholesterol concentration of 240 mg/dL or more. Desirable cholesterol concentrations are less than 200 mg/dL.
Based on data from the 2009-2012 National Health and Nutrition Examination Survey (NHANES), an estimated 73.5 million (31.7%) US adults aged 20 years or older has high LDL-C 130 mg/dL, but only 48.1% are treated and 29.5 % have their LDL-C controlled. A person with high LDL-C is defined as either a person whose LDL-C levels were above the LDL-C goal levels or a person who reported currently taking cholesterol-lowering medication. The proportion of adults with high LDL-C who are treated increased from 28.4% to 48.1% between the 1999-2002 and 2005-2008 study periods. Among adults with high LDL-C, the prevalence of LDL-C control increased from 14.6% to 33.2% between the periods. [11]
International statistics
Serum cholesterol concentrations vary widely throughout the world. Generally, countries associated with low serum cholesterol concentrations (eg, Japan) have lower CHD event rates, while countries associated with very high serum cholesterol concentrations (eg, Finland) have very high CHD event rates. However, some populations with similar total cholesterol levels have very different CHD event rates, as would be expected given that other risk factors (eg, prevalence of smoking or diabetes mellitus) also influence CHD risk. The cholesterol levels in developing countries tend to increase as western dietary habits (McDonald's syndrome) replace traditional diets.
Race, sex-, and age-related demographics
Among adults, National Health and Nutrition Examination Survey data (2011-2012) showed higher LDL cholesterol level among Hispanic males (38.8%), than non-Hispanic black males (30.7%) and than non-Hispanic white males (29.4%)
Elevated LDL-C is more common in females (32%) than in males (31%), based on National Health and Nutrition Examination Survey data (2011-2012).
In adults, hypercholesterolemia increases with advancing age, as shown in the image below.
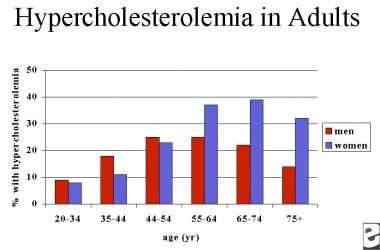 National Health and Nutrition Examination Survey data for hypercholesterolemia among American adults.
National Health and Nutrition Examination Survey data for hypercholesterolemia among American adults.
Prognosis
Statins have revolutionized the treatment of hypercholesterolemia. Coupled with the treatment of hypertension and the use of beta-blockers, angiotensin-converting enzyme inhibitors, and aspirin, the potential for reduction of CHD events in patients with known atherosclerosis is significant.
Cholesterol reduction is certainly useful as a CHD risk-reduction strategy and for primary prevention in individuals who are at high risk for CHD and atherosclerosis.
Morbidity/mortality
The primary consequence of hypercholesterolemia is increased CHD risk. [12] Data from epidemiological studies (eg, the Multiple Risk Factor Intervention Trial and the Framingham Heart Study) show a relationship between elevated LDL-C concentrations and CHD events and CHD mortality rates. In the prestatin era, randomized clinical trials showed a clear correlation between CHD morbidity and mortality but not total mortality. The advent of the statins, medications that are more easily tolerated and substantially more powerful than older cholesterol-lowering medications, increased the likelihood of substantial LDL-C lowering (increased power). Thus, the statins showed benefits that drugs used in previous studies had not. [13]
Placebo-controlled statin trials have demonstrated not only reduced coronary morbidity and mortality in primary and secondary prevention populations, but also decreased total mortality.
The causative relationship between LDL-C levels and ischemic stroke and transient ischemic attack (TIA) was suggested by decreased cerebrovascular events in several major statin trials in which stroke was a secondary endpoint. The SPARCL (Stroke Prevention by Aggressive Reduction in Cholesterol Levels) study definitively showed that in patients who had suffered a recent stroke or TIA but who had no CHD, high-dose statin reduced the overall incidence of stroke and cardiovascular events despite a small, but statistically significant, increase in the incidence of hemorrhagic stroke. [14, 15]
Patient Education
Dietary education about a low-fat (especially saturated fat and trans fat), low-cholesterol diet is of paramount importance.
For patient education resources, see the Cholesterol Center, as well as High Cholesterol, Cholesterol Charts, Lifestyle Cholesterol Management, Cholesterol Lowering Medications, and Statins for Cholesterol.
-
Relative risk of coronary heart disease (CHD) mortality versus baseline serum cholesterol over time in 3 large cohorts of young men. CHA is Chicago Heart Association Detection Project in Industry, PG is Chicago Peoples Gas Company, and MRFIT is Multiple Risk Factor Intervention Trial. Adapted from Stamler, 2000.
-
Simplified diagram of cholesterol metabolism. LDL is low-density lipoprotein, VLDL is very low-density lipoprotein, IDL is intermediate-density lipoprotein, HDL is high-density lipoprotein, and LPL is lipoprotein lipase.
-
National Health and Nutrition Examination Survey data for hypercholesterolemia among American adults.
-
Angiographic and clinical endpoint trials with statins.
-
Major coronary heart disease (CHD) clinical endpoint studies of primary prevention and stable CHD with statins versus placebo. *not statistically significant. + atorvastatin 10 mg is the comparator rather than placebo. ++ LDL-C in the atorvastatin 80 mg group/LDL-C in the atorvastatin 10 mg group.





