Practice Essentials
Entrapment neuropathies are disorders of the peripheral nerves that are characterized by pain and/or loss of function (motor and/or sensory) of the nerves as a result of chronic compression. The brain and the spinal cord receive and send information through muscles and sensory receptors, and information sent to organs of the body is transmitted through the nerves. These nerves travel to the upper and lower extremities and traverse various joints along their paths. Unfortunately, these nerves can become compressed or entrapped at various regions of the extremities, especially at "tunnel" regions, where they may be predisposed or vulnerable to compression.
Neurosurgeons, among other surgical specialists (eg, orthopedists, plastic surgeones), treat these entrapment neuropathies, which can account for 10-20% of cases in a practice. The first operations or decompressions for different nerve entrapments were performed more than a century ago, but the disorders were described even earlier by such pioneering physicians as Sir Astley Cooper (1820s) and Sir James Paget (1850s).
Repetitive injury and trauma to a nerve may result in microvascular (ischemic) changes, edema, injury to outside layers of the nerve (myelin sheath) that aid in transmission of the nerve’s messages, and structural alterations in membranes at the organelle levels in both the myelin sheath and the nerve axon. Focal segmental demyelination at the area of compression is a common feature of compression syndromes. Complete recovery of function after surgical decompression reflects remyelination of the injured nerve. Incomplete recovery in more chronic and severe cases of entrapment is due to Wallerian degeneration of the axons and to permanent fibrotic changes in the neuromuscular junction that may prevent full reinnervation and restoration of function.
Nerve entrapment syndromes result from chronic injury to a nerve as it travels through an osseoligamentous tunnel; compression is typically evident between the ligamentous canal and bony surfaces. Other anatomic sites with potential for entrapment include the muscular arcade of the supinator (also known as the arcade of Frohse), the posterior interosseous nerve (PIN), and the thoracic outlet for the lower trunk of the brachial plexus. [1]
In cases of nerve entrapment, at least 1 portion of the compressive surface is mobile. This results in a repetitive "slapping" insult or "rubbing/sliding" compression against sharp, tight edges with motion at the adjacent joint, resulting in a chronic injury. Immobilization of the nerve by means of a splint or lifestyle adjustments may resolve the symptoms. Entrapment neuropathies can also be caused by systemic disorders such as rheumatoid arthritis, pregnancy, acromegaly, or hypothyroidism.
Suprascapular nerve entrapment may cause 2% of all cases of chronic shoulder pain. Of the many reported causes of suprascapular nerve entrapment, the most common are para-labral cysts, usually found in the spinoglenoid notch, and microtrauma among elite athletes. [2]
Carpal tunnel syndrome (CTS), defined as compression of the median nerve at the wrist, is the most common entrapment neuropathy. [3] Cubital tunnel syndrome, the second most common, is caused by compression at the elbow. [4] Other rare nerve entrapment syndromes involve the suprascapular nerve and account for approximately 0.4% of upper girdle pain symptoms; meralgia paresthetica is compression of the lateral femoral cutaneous nerve (LFCN) within the groin. [5]
(An ulnar nerve transposed at the elbow is shown in the image below.)
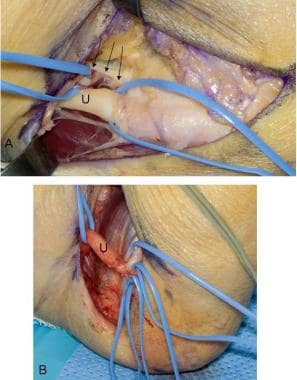 Ulnar nerve (U) transposition at the elbow. A: The medial intermuscular septum (arrows) is resected to prevent compression of the transposed nerve. Vasoloops are around the ulnar nerve and a vascular pedicle between the nerve and the septum that has been preserved. B: After subcutaneous transposition, the ulnar nerve is observed lax in elbow flexion. The ulnar nerve and its distal branches are surrounded by vasoloops.
Ulnar nerve (U) transposition at the elbow. A: The medial intermuscular septum (arrows) is resected to prevent compression of the transposed nerve. Vasoloops are around the ulnar nerve and a vascular pedicle between the nerve and the septum that has been preserved. B: After subcutaneous transposition, the ulnar nerve is observed lax in elbow flexion. The ulnar nerve and its distal branches are surrounded by vasoloops.
Anterior cutaneous nerve entrapment syndrome is a frequent cause of abdominal wall pain due to trapped thoracic intercostal nerves between abdominal muscles. History and bedside Carnett's sign can elicit the diagnosis. Injection of local anesthetics with steroids in the junction between rectus sheath and abdominal muscle under ultrasound guidance can provide sustained pain relief. [6]
Cauda equina syndrome (CES) involves compression of some or all of the lumbar and sacral peripheral nerve roots.The literature reveals timing to surgical decompression, severity of symptoms at the time of onset, and involvement of bladder dysfunction as prognostic indicators of CES. [7]
The American College of Radiology (ACR) has published the following guidelines for thoracic outlet syndrome [8] :
-
Radiography of the chest and either MRI without and with IV contrast of the chest or MRI without IV contrast of the chest are usually appropriate for the initial and follow-up imaging after surgery or intervention for patients with neurogenic thoracic outlet syndrome (nTOS). MRI without IV contrast is an acceptable alternative to MRI without and with IV contrast (ie, only one procedure will be ordered to provide the clinical information to effectively manage the patient’s care).
-
Radiography of the chest and US duplex Doppler of the subclavian artery and vein, CT with IV contrast of the chest, or catheter venography of the upper extremity are usually appropriate for the initial and follow-up imaging after surgery or intervention for patients with venous thoracic outlet syndrome (vTOS). US duplex Doppler, CT with IV contrast, and catheter venography are equivalent alternatives (ie, only one procedure will be ordered to provide the clinical information to effectively manage the patient’s care).
-
Radiography of the chest and CTA with IV contrast of the chest, MRA without and with IV contrast of the chest, US duplex Doppler of the subclavian artery and vein, or arteriography of the upper extremity are usually appropriate for the initial and follow-up imaging after surgery or intervention for patients with arterial thoracic outlet syndrome (aTOS). CTA with IV contrast, MRA without and with IV contrast, US duplex Doppler, and arteriography of the upper extremity are equivalent alternatives (ie, only one procedure will be ordered to provide the clinical information to effectively manage the patient’s care).
-
Chest PA radiograph showing a right cervical rib (arrows), a possible cause of thoracic outlet syndrome.
-
Ulnar nerve (U) transposition at the elbow. A: The medial intermuscular septum (arrows) is resected to prevent compression of the transposed nerve. Vasoloops are around the ulnar nerve and a vascular pedicle between the nerve and the septum that has been preserved. B: After subcutaneous transposition, the ulnar nerve is observed lax in elbow flexion. The ulnar nerve and its distal branches are surrounded by vasoloops.
-
Common peroneal nerve decompression at the fibular neck. A: The common peroneal nerve (P) has been identified and mobilized proximal to the fibular tunnel region, fascia (F) covering peroneus longus. B: The common peroneal nerve has been traced through the fibular tunnel. The fascia overlying the peroneus longus muscle has been divided and the muscle (M) has been retracted. The fascial band overlying the nerve is released.
-
Median nerve (M) after decompression at the wrist; note the congestion from the longstanding compression. The transverse carpal ligament (arrows) has been transected. Fat is observed distally.




