Overview
Cognitive disorder in the setting of human immunodeficiency virus (HIV) infection has long been recognized as an important and disabling aspect of the disease. It has been known by a variety of terms. The current terminology, HIV-associated neurocognitive disorder (HAND) and its subclassifications, were articulated at the Frascati conference in 2004. [1] In addition to its effects on the cellular immune system, HIV enters the central nervous system (CNS) early in the course of the infection and causes several important CNS conditions over the course of the disease, such as HIV encephalopathy and HAND. [2] As part of the acute HIV syndrome during seroconversion, patients may experience HIV encephalopathy. HIV-associated progressive encephalopathy (HPE) is a syndrome complex with cognitive, motor, and behavioral features seen in children. [3]
Prior to the advent of highly active antiretroviral therapy (HAART), dementia was a common source of morbidity and mortality in HIV-infected patients. It was usually observed in the late stages of acquired immunodeficiency syndrome (AIDS), when CD4+ lymphocyte counts fall below 200 cells/mL, and was seen in up to 50% of patients prior to their deaths. In 1986, the term HIV-associated dementia (HAD) was introduced to describe a unique constellation of neurobehavioral findings. [4, 5] As HIV treatment entered the HAART era, neurocognitive dysfunction has remained prevalent, with cross-sectional studies suggesting some degree of cognitive impairment in 44% of patients. [6] The nature and severity of the impairment changed with the advent of prevalent HAART therapy, however, leading to the new consensus definition of HIV-associated neurocognitive disorder in 2004. [1]
HAND encompasses a hierarchy of progressively more severe patterns of neurological involvement. It is defined as an acquired impairment in cognitive functioning involving at least 2 ability domains with a decline of daily functioning in severe cases. The spectrum ranges from asymptomatic neurocognitive impairment (ANI) to minor neurocognitive disorder (MND) to more severe HIV-associated dementia (HAD). [1]
While in the pre-HAART era, HAD developed predominantly in patients with high viral loads and CD4 counts < 200, whereas HAND develops in patients with normal CD4 counts. [6]
The overall psychosocial and emotional burden on the family and friends of patients with HAND remains tremendous. Patients with cognitive difficulties have problems with adherence to their medication regimens, follow-up visits, and health behavior. Because of their neuropsychiatric problems, such patients may be more prone to risk behavior (eg, unprotected intercourse), and they may pose a greater risk of transmission of the virus.
In addition to HIV itself, other causes of neurologic complications in HIV-infected individuals include opportunistic infections, tumors, autoimmune conditions, and antiretroviral drugs. In addition, patients are at risk for many other neurologic complications of HIV infection, including vacuolar myelopathy, peripheral neuropathies, and polymyositis, which can contribute to further disability.
For other discussions of HIV infection, see HIV Disease, Pediatric HIV Infection, and Antiretroviral Therapy for HIV Infection.
Pathophysiology
HIV is thought to enter the brain via HIV-infected macrophages and lymphocytes. Other proposed mechanisms include passage of cell-free virus into the brain and release of the virus from the infected endothelial cells. [7] The virus replicates in these cells and may infect other cells, such as microglia, oligodendrocytes, astrocytes, and neurons; macrophages and microglia are the most commonly infected cells. HIV infection in the CNS can be detected and monitored by cerebrospinal fluid (CSF) viral load measurements. A positive correlation has been established between CSF viral load and the extent of cognitive dysfunction.
Immunohistochemistry studies show that the virus is most densely located in the basal ganglia, subcortical regions, and frontal cortex. Pathologic changes at autopsy are also predominantly subcortical, involving the deep gray matter (ie, basal ganglia, thalamus) and white matter regions.
The mechanism by which HIV infection of the CNS leads to neurocognitive disorders is likely multifactorial and is the subject of intense research.
Cellular proteins
Widespread pathologic damage may occur via indirect cellular responses with the secretion of chemokines, proinflammatory cytokines, nitrous oxide, and other neurotoxic factors. These products are produced not only from the infected cells (eg, macrophages, astrocytes, microglia) but also from noninfected activated cells.
Much attention has been placed on chemokines, such as CCL4 and CXCL12, and their respective chemokine receptors, CCR5 and CXCR4. These may affect many cellular processes, including neuronal migration, apoptosis, and neurotransmitter regulation.
HIV proteins (virotoxins)
Studies in several transgenic mouse models indicate that expression of a single or multiple HIV genes leads to clinical and histologic abnormalities. [8] Damage to neurons may occur through the actions of specific HIV proteins, including gp120, gp41, Tat, Nef, Vpr, and Rev. These viral proteins may be directly toxic to neuronal cells or may cause damage by activating astrocytes, microglia and macrophages to release cytokines, chemokines, or neurotoxic substances. [9, 10, 11] By initiating feedback loops, virotoxins may amplify their toxicity and cause widespread damage.
The basal ganglia show the highest immunostaining for the HIV p24 antigen. Some studies show that gp41 expression in the basal ganglia and frontal lobes correlates significantly with dementia severity. However, the presence of macrophages and microglia correlate better with clinical dementia than with the density of HIV-infected cells in the brain, as determined by gp41-positive cells. [12] In vitro, neuronal death is caused by gp120 and is accompanied by the opening of calcium channels in the neuronal membrane.
HIV p53 (tumor suppressor transcription factor) [13] appears to have multiple roles in the pathogenesis of the disease. HIV proteins Tat and gp120 cause microglia to release factors that promote neuronal p53 activation. All 3 cell types in the brain (microglia, astrocytes, and neurons) accumulate p53, causing cell cycle arrest; in neurons, this ultimately induces apoptosis and cell death by oxidative injury and DNA damage. [14]
Viral proteins Tat and gp120 have been shown to have synergistic neurotoxicity with cocaine and methamphetamine. Thus, users of these drugs may have a higher likelihood of developing AIDS dementia complex (ADC).
Autoimmune disease
CNS damage may occur by humoral immune mechanisms, as evidenced by the presence of anti-CNS antibodies in AIDS patients with dementia but not in those without dementia. [15] Autoantibodies against myelin oligodendrocyte glycoprotein may persist in a high percentage of patients despite viral clearance; this finding suggests ongoing neuroinflammation, which may prevent recovery from HIV-associated neurocognitive disorder. [16]
Risk factors
In the pre-HAART era, the identified risk factors for HAD were low weight, anemia, constitutional symptoms, low CD4+ count, and high plasma HIV-RNA load. In the post-HAART era, the most significant risk factor for HAND is CD4 nadir, but risk factors also include age, hypertension, and hyperlipidemia. This identification, along with the neuroimaging similarities between HAND and vascular cognitive impairment, has led some to postulate that premature aging at the neurovascular unit may be the primary target of HIV-related brain injury in the treated HIV population. [17]
The Multicenter AIDS Cohort Study reported that older age was associated with more rapid progression to dementia and death. [18] The prevalence of cognitive disorders in persons who are HIV positive and older than 50 years is greater than in younger patients. [19]
Epidemiology
The introduction of HAART had two major impacts on the epidemiology of HIV-associated neurocognitive disorder (HAND). Firstly, the prevalence of the most severe form, HIV-associated dementia, which had been estimated at 10–15%, became rare, measured at only 2% in the cross-sectional CHARTER study. Secondly, the overall prevalence of HAND, driven by its more mild forms, increased significantly to 44%. Curiously, the study found that the rate of cognitive impairment was higher in the population treated with HAART rather than the off-treatment group, which may reflect severity of disease and length of infection. [6]
A meta-analysis attempting to quantify the global prevalence of HAND estimated it to be 42.6% with 88% of cases representing mild disease. The proportion of patients with HAND decreased with level of income, CD4 count, and treatment with HAART. Findings suggest that early initiation of HAART and prevention of severe immunosuppression (and, thus, CD4 nadir) reduced both the prevalence and the severity of HAND. The prevalence in sub-Saharan Africa and Latin America may be higher than in the United States and Western Europe. [20]
Prognosis
The prognosis of HIV-associated neurocognitive disorder (HAND) is dependent on its severity. Little is known about the expected progression of asymptomatic neurocognitive impairment (ANI) and minor neurocognitive disorder (MND), but by extrapolating from the Multicenter AIDS Cohort Study, which found that patients with HIV infection had no more decline in neuropsychometric tests than age-matched controls, suggests that cognitive deterioration in HAND patients is not widespread. The CHARTER study, similarly, found that most patients (61%) remained stable over a 42-month period while 16% improved and 22% declined. Patients who experienced progression were more likely to have severe comorbidities such as drug use and hepatitis C as well as a higher rate of HAART treatment failure and lower CD4 count. [21, 2]
HIV-associated dementia (HAD) is associated with a much worse prognosis, and is typically associated with progressive impairment of attention and concentration, motor slowing, and behavioral change with death within 1 year of presentation. Patients who are severely impacted and meet criteria for HAD based on neuropsychological evaluation but do not show evidence of progression are suspected of having a better prognosis. [2]
Patient Education
Educate the patient at an early stage, and discuss future medicolegal implications of dementia. The patient should be strongly encouraged to prepare a living will and to assign power of attorney.
Educate patients and families about the persistent dangers of the transmission of HIV. The following Web sites can be referenced for further information:
-
National Institutes of Health -HIV Infection and AIDS: An Overview
-
Centers for Disease Control and Prevention – HIV/AIDS
-
UCSF Center for HIV Information -HIV Transmission and Prevention in Adolescents
Education of family members, friends, and caregivers of a patient with HIV-associated neurocognitive disorder (HAND) is of great importance. HIV dementia is a multifaceted problem, and caregivers should know about the complications, including psychiatric complications. Often, friends and family need counseling and support to deal with this chronic and difficult condition.
For patient education information, see the Dementia Center, Immune System Center, and Sexually Transmitted Diseases Center, as well as Dementia Due to HIV Infection, Dementia Overview, and HIV/AIDS.
Clinical Presentation
Currently, it is estimated that nearly half of all patients with HIV infection demonstrate lower than expected performance in various neuropsychological assessments compared with healthy individuals matched for age, race, education, and ethnicity. Neuropsychiatric symptoms such as apathy, depression, anxiety, and psychosis are commonly seen in these individuals. Significant memory impairment is also seen in these individuals. Personality changes, including social withdrawal and, in some extreme cases, vegetative state and mutism, are also seen.
Not all patients with HIV-associated neurocognitive disorder (HAND) progress to HIV-associated dementia (HAD). The onset of HAD is correlated with high viral loads, CD4 nadir, and the duration of the infection itself. With the use of HAART, milder forms of cognitive dysfunction, asymptomatic neurocognitive impairment (ANI) and minor neurocognitive disorder (MND), have become common.
Cognitive assessment in patients with HAD demonstrates deficits in memory, abstraction, verbal fluency, decision-making, and attention.
Rare features include sleep disturbances, psychosis (with mania), and seizures. Motor problems include imbalance, clumsiness, and weakness.
Early signs and symptoms are subtle and may be overlooked. Consequently, cognitive screening tests should be part of the routine care of HIV-infected patients, especially those at high risk, as indicated by older age, high plasma HIV ribonucleic acid (RNA) levels, low CD4+ cell counts, hepatitis C, and poor baseline cognitive status.
In ANI and MND, activities of daily living are only mildly impaired. This contrasts with the significant impairment seen in HAD.
In infants with HIV-associated progressive encephalopathy (HPE), characteristic features include decline in intellectual and motor milestones. In young children, the rate of acquisition of new skills decreases, and fine motor ability and dexterity may become impaired. Feeding difficulties may develop. In older children and adolescents, the presentation is similar to that of AIDS dementa complex (ADC) in adults.
Physical Examination
The examination for AIDS dementa complex (ADC) includes a full Mental Status Examination (MSE), a general neurologic examination, and a general physical examination. The patient should then be referred for complete neuropsychological testing addressing specific domains.
Some patients with HIV can become depressed, suicidal, and homicidal. Therefore, a thorough psychiatric assessment should also be performed at each visit.
In the early stage, findings from the MSE and the general neurologic examination are normal. MSE findings are abnormal if the patient exhibits inattention, impaired concentration (eg, digit span, serial 7's), memory loss (eg, recalling 3 objects at 5 min), slowed verbal responses, and a blunted affect.
Early on, the neurologic examination may be normal or reveal subtle impairment of rapid limb and eye movements. In more severe cases, the neurologic examination shows frontal release signs, slowed rapid movements, antisaccadic eye movements, incoordination, abnormal gait, hyperreflexia, hypertonia, extensor-plantar response weakness, and peripheral neuropathy. [22] Cortical signs, including apraxia, aphasia, and agnosia, typically are absent.
The terminal stage of HIV-associated dementia (HAD), after progression over several months, includes severe psychomotor retardation and dementia, apraxia, paraparesis, and akinetic mutism. Death ensues within a few months of reaching this stage.
Seizures are rare and warrant consideration of other conditions.
Diagnostic Criteria
AIDS dementia complex (ADC) encompasses cognitive deficits, behavioral changes, and motor involvement. Affected persons may manifest deficits in each of the 3 aspects at varying severity; thus, some patients may present primarily with cognitive changes, such as slowed processing of information, captured by neuropsychological testing; others may present with behavioral problems; and still others may be have a chief complaint of motor symptoms, such as unsteady gait, tremor, or weakness.
In 1991, the American Academy of Neurology defined neurocognitive deficits seen with HIV as HIV-associated dementia (HAD) and minor cognitive motor disorder (MCMD). Criteria for the diagnosis of HAD included cognitive deficits in 2 or more cognitive domains that cause impairment in activities of daily living (ADL) and an abnormality in either motor or neurobehavioral function. Patients with MCMD were defined as having decreased function in 2 cognitive or behavioral domains but without severe enough impairment to meet criteria for HAD.
In 2007, Antinori et al proposed more refined criteria for diagnosing cognitive impairment associated with HIV. They proposed 3 entities: asymptomatic neurocognitive impairment (ANI), HIV-associated mild neurocognitive disorder (MND), and HIV-associated dementia (HAD).
Standardized neuropsychological testing was required to assess the following domains of cognition: language, attention, executive function, memory, speed of information processing, and perceptual and motor skills. In order to meet diagnostic criteria for ANI, MND, or HAD, patients must have no other etiology of dementia and must not have the confounding effect of substance use or psychiatric illness. [1]
ANI was proposed on the basis of experience with patients who had declines in their performance on formal neuropsychological testing but had no functional impairment in ADL. One standard deviation (SD) below the mean for age and education appropriate norms in at least 2 of at least 5 tested domains in formal testing is diagnostic of ANI.
Patients with MND meet the criteria for ANI, except that they also have impairment with ADL as reported by patient or by a corroborator. HAD can be diagnosed if patients score 2 SDs below the mean in at least 2 cognitive domains and have marked impairment in ADL as a result of cognitive decline.
Staging of AIDS Dementia Complex
Price and Brew in 1988 outlined a clinical staging of AIDS dementia complex (ADC), the Memorial Sloan-Kettering rating scale. [23] Currently, it is used mostly as a research instrument.
Stage 0
In stage 0 (normal), mental and motor functions are normal. In stage 0.5 (equivocal/subclinical), symptoms may be absent, minimal, or equivocal, with no impairment of work or performance of ADL. Mild signs (snout response, slowed ocular or extremity movements) may be present, but gait and strength are normal.
Stage 1
In stage 1 (mild), the patient is able to perform all but the more demanding aspects of work or activities of daily living (ADL) but has unequivocal evidence of functional, intellectual, or motor impairment. Signs or symptoms may include diminished performance on neuropsychological testing. Patient can walk without assistance.
Stage 2
In stage 2 (moderate), the patient is able to perform basic activities of self-care but cannot work or maintain the more demanding aspects of daily life. The patient is ambulatory but may require a single prop.
Stage 3
In stage 3 (severe), the patient has major intellectual incapacity (cannot follow news or personal events, cannot sustain complex conversation, shows considerable slowing of all outputs). Motor disability precludes walking unassisted (ie, without walker or personal support); walking is usually slowed and accompanied by clumsiness of arms.
Stage 4
In stage 4 (end stage), the patient is in a nearly vegetative state. Intellectual and social comprehension and output are at a rudimentary level. The patient is nearly or absolutely mute. The patient is paraparetic or paraplegic, with urinary and fecal incontinence.
Neurologic Examination in Pediatric Patients
In neonates, the physical examination findings are often normal. Although the age of onset is usually in the first year of life, manifestations may not be noticeable until age 2–3 years. At this time, children may present with cognitive impairment, masklike facies, acquired microcephaly, and pseudobulbar and corticospinal tract signs.
Common findings in older children and adolescents are impaired attention, decreased linguistic and scholastic performance, psychomotor slowing, emotional lability, and social withdrawal. Examination findings are similar to those in adults with AIDS dementia complex (ADC).
Criteria for HIV-associated progressive encephalopathy
The American Academy of Neurology defines HIV-associated progressive encephalopathy (HPE) as the presence, for at least 2 months, of at least one of the following progressive findings in a pediatric patient with no concurrent illness, other than HIV infection, that could explain the findings: [24]
-
Failure to attain, or loss of, developmental milestones or loss of intellectual ability verified by standard developmental or neuropsychological tests
-
Acquired microcephaly as demonstrated by head circumference measurement or brain atrophy on serial computed tomography (CT) or magnetic resonance imaging (MRI) imaging in children younger than 2 years of age
-
Acquired symmetrical motor deficits manifested by 2 or more of the following: paresis, pathological reflexes, ataxia or gait disturbance
Differential Diagnosis
Dementia due to HIV disease is a diagnosis of exclusion. The differential diagnosis includes the following:
Other problems to be considered in the differential diagnosis include the following:
-
Cerebral lymphoma
-
CNS infections (eg, tuberculosis, toxoplasmosis, cryptococcal meningitis, neurosyphilis)
-
Metabolic encephalopathies
-
Depression
-
Psychoactive drugs
-
Attention deficit hyperactivity disorder
-
Toxic-metabolic states (eg, alcoholism, vitamin B-12 deficiency, thyroid disorders, adverse medication effects, drug interaction, recreational drug use)
Antiretroviral medications may have neurocognitive side effects (eg, efavirenz therapy can result in depression, insomnia, and decreased neuropsychological testing). [25]
Immune reconstitution inflammatory syndrome (IRIS)
Clinical worsening may be observed in patients with HIV soon after initiation of HAART therapy, due to mounting of a significant inflammatory response. This is seen even while a patient’s CD4+ count improves and viral load dramatically decreases. Immune reconstitution inflammatory syndrome (IRIS) may actually worsen AIDS dementia complex (ADC) and progressive multifocal leukoencephalopathy. [26]
ADC can be distinguished from IRIS by the speed of onset. ADC is subacute to chronic, whereas IRIS can be more acute to subacute. ADC occurs in the setting of untreated, progressive AIDS, whereas IRIS begins with the start of treatment. Distinguishing between the 2 is important, because the treatment is different. ADC requires HAART with high penetration into the CNS. IRIS should be treated with steroids, depending on its severity.
An entity termed encephalitis with CD8 cell infiltration has been identified in patients with latent or inactive HIV infection of the brain due to restoration of T-cell function with HAART, leading to an intense inflammatory reaction with an influx of CD8+ lymphocytes. The influx of the CD8 cells may cause macrophage activation and control of infection but can also present with a subacute or acute encephalopathy. The imbalance between CD8+/CD4+ cells may cause worsening of the HIV encephalopathy and can also produce an acute demyelinating process similar to multiple sclerosis or acute demyelinating encephalomyelitis.
These cases may represent a specific clinicopathological entity, of which a few comparable cases have been already described. They can be included in the wide framework of immune reconstitution disease. Such syndromes have been described with opportunistic infections, but only rarely with HIV infection of the CNS. [27] In a report of 14 patients treated with glucocorticosteroids, therapeutic response varied from excellent, with no sequelae (n=5), to moderate, with cognitive disorders (n=4). The mean survival time was 8 years; however, 5 patients died within 13 months of the initiation of treatment.
Overview of Workup
The workup includes lumbar puncture with cerebrospinal fluid (CSF) analysis, neuroimaging, and neuropsychological testing. MRI is the first-choice neuroimaging modality. Electroencephalography (EEG) reveals generalized slowing in the later stages; this is a nonspecific finding. Brain biopsy is not recommended for corroboration, but biopsy material obtained for other reasons may confirm this diagnosis.
Draw peripheral blood for syphilis serology testing, thyroid studies, routine electrolyte levels, blood urea nitrogen (BUN)/creatinine determination, and a drug screen to effectively exclude other metabolic and infectious etiologies.
Vitamin B-12 and folic acid levels should be determined and, if necessary, corrected (see Vitamin B-12 Associated Neurological Diseases). In cases of borderline low B-12 levels, homocysteine and methylmalonic acid levels are better indicators of a deficiency. An assay for anti-parietal cell or anti-intrinsic factor antibodies and a Schilling test may be indicated.
Cerebrospinal Fluid Analysis
CSF markers are helpful in early dementia, when the diagnosis may be confusing. These markers, including neopterin, quinolinic acid, certain cytokines (eg, tumor necrosis factor–alpha, interleukin 1, interleukin 6), and antibodies to gp120 (eg, HIV viral envelope protein), correlate with the severity of dementia, but they are only research tools and therefore are not widely available.
The axonal neurofilament light chain protein and neuronal protein Tau are frequently elevated in the CSF of patients with HIV-associated dementia (HAD). These proteins sometimes can be seen even before HAD develops and normalize with treatment. Neopterin, MCP-1, and CSF viral load can be used to assess the effect of treatment on viral replication.
CSF beta-2 microglobulin, an immune activation marker, is a more specific CSF marker and has a positive predictive value of 88% if levels are higher than 3.8 mg/dL. CSF beta-2 microglobulin levels were found to be twice as high in patients who cognitively improved with HAART than in those who did not, indicating that CNS inflammation plays a major role in reversible neurocognitive deficits. Patients with HIV dementia have elevated levels of certain matrix metalloproteins in the CSF, but the clinical significance of these proteins is unclear.
Beta-amyloid(1-42) measurements in CSF of patients with HIV who are cognitively impaired are similar to patients with mild dementia of the Alzheimer type (DAT). Normal or slightly depressed CSF tau and p-tau181 measurements distinguish patients with HIV-associated cognitive impairment from patients with DAT. [28]
Other CSF findings are as follows:
-
Elevated protein (60%) and immunoglobulin G (80%)
-
Oligoclonal bands are sometimes present
-
CSF is usually acellular, but a mononuclear pleocytosis is found in 25%
-
HIV antibodies are present
HIV frequently is cultured from CSF or detected by means of polymerase chain reaction (PCR). However, HIV-1 is present in CSF in the absence of neurologic abnormalities. CSF HIV RNA levels do not correlate with neuropsychological impairment; rather, plasma levels are a better correlation.
CSF studies to help exclude CNS infection include the following:
-
Cryptococcal antigen
-
Venereal Disease Research Laboratory (VDRL) test
-
Fluorescent treponemal antibody-absorption test (FTA-abs)
-
Cytomegalovirus polymerase chain reaction (PCR) test
Depending on the clinical picture, PCR studies may also be obtained for herpes simplex and varicella zoster viruses and JC virus (the causative agent of progressive multifocal leukoencephalopathy).
Neuroimaging
CT and MRI of the brain can support a diagnosis of HIV-associated neurocognitive disorder (HAND) and rule out other neurologic opportunistic infections or neoplasms. CT can reveal diffuse cortical atrophy, ventricular enlargement, and increased white matter signal in later stages (see the image below). Basal ganglia calcifications are seen in adults but are more common in children. Neuroimaging results may be normal in minor cognitive motor disorder (MCMD).
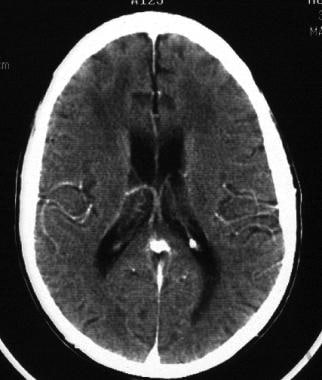 HIV-1 encephalopathy and AIDS dementia complex. CT scan of the brain of a patient with HIV associated neurocognitive disorder (HAND) shows diffuse atrophy and ventricular enlargement and attenuation of periventricular white matter.
HIV-1 encephalopathy and AIDS dementia complex. CT scan of the brain of a patient with HIV associated neurocognitive disorder (HAND) shows diffuse atrophy and ventricular enlargement and attenuation of periventricular white matter.
Primary infection of the CNS may lead to focal white spots in the white matter on MRI. These resemble white matter abnormalities seen in various other settings such as advanced age, diabetes, and hypertension and should be interpreted with caution. Some degree of atrophy occurs during the latent stage, and, with ongoing disease activity, evidence of interstitial fluid accumulation can be seen that is more pronounced around the ventricles, in the form of hyperintense signals on T2-weighted images (see the image below).
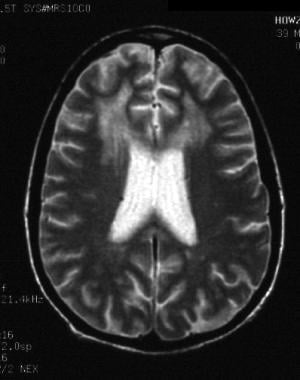 HIV-1 encephalopathy and HIV associated neurocognitive disorder (HAND). T2-weighted MRI shows ventricular enlargement and large areas of hyperintense signal in the subcortical white matter of both frontal lobes.
HIV-1 encephalopathy and HIV associated neurocognitive disorder (HAND). T2-weighted MRI shows ventricular enlargement and large areas of hyperintense signal in the subcortical white matter of both frontal lobes.
Differential diagnosis includes multiple sclerosis (MS) and small-vessel disease.
Functional MRI
Functional MRI studies are not yet widely available, but they may demonstrate abnormalities in regional brain activation during working memory tasks before mild dementia can be detected by clinical or neuropsychological evaluation. [29]
Proton magnetic resonance spectroscopy (MRS) is a functional imaging technique that measures brain metabolites. Neuronal injury is confirmed by finding lower N-acetyl aspartate (NA) levels (a marker of neuronal metabolism) in the frontal white matter. [30]
In the basal ganglia and white matter, where gliosis and inflammatory changes are noted, the level of choline-containing metabolites, which is a marker of glial metabolism, is increased.
Chang et al showed that even in the asymptomatic stage of ADC, MRS demonstrates metabolite changes in the basal ganglia and frontal white matter. In the absence of clinically recognizable symptoms, elevated glial marker, myoinositol-to-creatinine ratio (MI/Cr), is seen in the white matter, indicating early HIV brain disease. [31, 32]
Patients with ADC have elevated MI/Cr and choline-to-creatinine ratio (Cho/Cr) in the basal ganglia and white matter, relative to the asymptomatic group. However, compared with controls, patients with ADC have decreased NA/Cr ratio, which is a neuronal marker. The decreased NA/Cr ratio in HAND is more profound in younger persons. This indicates that in older individuals, the metabolic changes seen may be a combination of age and HIV infection. [31, 32]
Research imaging tools
Position emission tomography (PET) may reveal abnormalities in cortical metabolism. This method is not widely available and is most useful as a research tool. PET scanning may also be useful in very difficult cases to help exclude CNS lymphoma, which shows increased uptake, whereas the lesions of AIDS dementia do not.
Single-photon emission computed tomography (SPECT) may reveal abnormalities in cerebral blood flow. This method is most useful for research rather than as a routine diagnostic tool.
Electroencephalography
Patients with subclinical seizures may present with symptoms that mimic dementia. Consider performing an EEG to help exclude this type of pseudodementia.
EEG findings may be normal in early dementia or may demonstrate diffuse slowing. However, this finding is nonspecific and is present in persons with dementia from any cause (even a metabolic one); therefore, it does not help in making an etiologic diagnosis.
Neuropsychological Testing
Neuropsychological testing can be used for early screening of asymptomatic, high-risk patients (eg, those with high viral load and low CD4 count [33] ) and for follow-up evaluations. Formal neuropsychological testing results may be normal in minor cognitive motor disorder (MCMD).
Early in the course, impairment of working memory is noted in bedside testing such as digit and word reversals and serial sevens.
In the early stages of the disease, mental status examination findings may be entirely normal. In such cases, neuropsychological testing is especially useful and can help to detect mild, early cognitive abnormalities. This testing can help to quantify and determine the specific pattern of the cognitive abnormality.
Several neuropsychologic screening tests have been proposed; the most widely accepted is the modified HIV dementia scale, although this scale has been found to be sensitive only for the most severe forms of impairment. The scale consists of 4 subsets that target memory (eg, recall, registration), psychomotor speed, constructional ability, and concentration. A total of 12 points can be earned, and a score lower than 6 points is considered abnormal. The test takes 10 minutes to administer and can be given by a nonneurologist. These tests are useful diagnostic adjuncts, but the results cannot solely determine the presence of HAND. Because false-negatives can occur with screening tests, a patient with a negative screening test may require more in-depth neuropsychological testing. [34]
In advancing disease, tests that explore the following abilities may be helpful:
-
Motor ability (ie, Finger Tapping Test, Grooved Pegboard Test)
-
Concentration (ie, Continuous Performance Test, Trail Making Test A and B)
-
Processing (ie, Trail Making Test A and B, Choice Reaction Time)
-
Memory/learning (ie, Weschler Memory Scale, California Verbal Learning Test)
-
Abstraction (ie, Wisconsin Card-Sorting Test)
-
Speech/language (ie, Boston Naming Test, Verbal Fluency Test)
Histologic Findings
The hallmark is HIV encephalitis in the white and subcortical gray matter. These changes are noted in 20-90% of patients. Some patients show only minimal changes. Atrophy is typically in a frontotemporal distribution. Diffuse myelin pallor may be present but is more commonly due to changes in the blood-brain barrier than to demyelination. Vacuolation may be observed.
Cortical neuronal loss is noted in 18-50% of patients. Subcortical neuronal loss (substantia nigra) is noted in 25%. Reduced synaptic density and dendritic arborization may be observed. Some neurons and astrocytes appear to die by apoptosis.
Brain tissue may be infiltrated by microglia, macrophages, lymphocytes, and multinucleated giant cells (see the images below). Activated glial cells are twice as numerous in brains of patients with AIDS as in brains of controls. Microgliosis may be diffuse or form clumps or nodules, often in a perivascular pattern in the white and subcortical gray matter.
Infected cells are associated consistently with macrophages/microglia and endothelial cells. Less commonly observed are astrocytes and neurons with restricted expression of HIV genes.
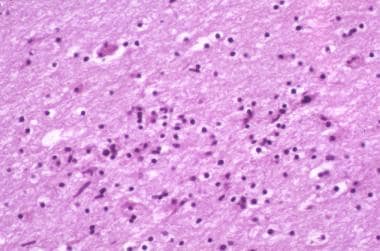 HIV-1 encephalopathy and HIV associated neurocognitive disorder (HAND). Photomicrograph shows perivascular and parenchymal infiltrates of lymphocytes and macrophages. These often form microglial nodules. Image contributed by Dr Beth Levy, Saint Louis University School of Medicine, St Louis, Missouri.
HIV-1 encephalopathy and HIV associated neurocognitive disorder (HAND). Photomicrograph shows perivascular and parenchymal infiltrates of lymphocytes and macrophages. These often form microglial nodules. Image contributed by Dr Beth Levy, Saint Louis University School of Medicine, St Louis, Missouri.
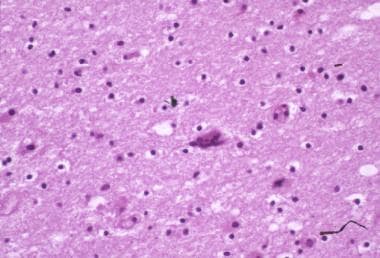
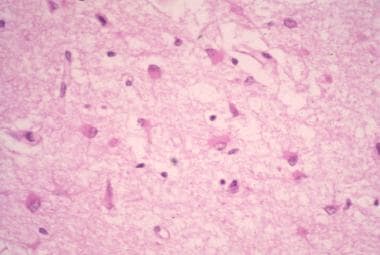 HIV-1 encephalopathy and HIV associated neurocognitive disorder (HAND). Photomicrograph illustrates the intense astrogliosis that is characteristic of HIV encephalitis. Image contributed by Dr Beth Levy, Saint Louis University School of Medicine, St Louis, Missouri.
HIV-1 encephalopathy and HIV associated neurocognitive disorder (HAND). Photomicrograph illustrates the intense astrogliosis that is characteristic of HIV encephalitis. Image contributed by Dr Beth Levy, Saint Louis University School of Medicine, St Louis, Missouri.
 HIV-1 encephalopathy and AIDS dementia complex. Multinucleated giant cells, as shown here, are a hallmark of HIV encephalitis and harbor the virus. Image contributed by Dr Beth Levy, Saint Louis University School of Medicine, St Louis, Missouri.
HIV-1 encephalopathy and AIDS dementia complex. Multinucleated giant cells, as shown here, are a hallmark of HIV encephalitis and harbor the virus. Image contributed by Dr Beth Levy, Saint Louis University School of Medicine, St Louis, Missouri.
Antiretroviral and Other Therapies
Currently, highly active antiretroviral therapy (HAART) is the cornerstone of treatment for HIV-related cognitive disorders. Aggressive early treatment of patients with HIV disease with antiviral medications and early suppression of viral replication prevents most of the devastating consequences of HIV dementia. [35]
Several studies have shown that early and aggressive treatment of HIV infection decreases the rate of dementia from greater than 50% to 10%. Patients on HAART show partial reversals of neuropsychological deficits and significant improvement, which is sustained, whereas patients not on HAART steadily decline. [36]
HAART protects against and induces remission and decreases the incidence of HIV-associated neurocognitive disorder (HAND) and HIV-associated progressive encephalopathy (HPE). Early and continuous viral suppression with HAART is associated with improved performance on neuropsychological testing.
However, some patients progress despite adequate control of the disease. One theory proposes poor CNS penetration of the antiretroviral drugs as the reason. The Cerebral Penetration Effective Index (CPE) has been proposed for estimating the effectiveness of antiretroviral drugs in the CNS. Progression may also be linked to comorbid conditions, such as drug use and head trauma, as well as social determinants of health.
Many antiretroviral medications have poor cerebrospinal fluid-to-plasma drug ratios, indicating poor CNS penetration. Exceptions include stavudine, abacavir, nevirapine, and zidovudine (ZDV). However, whether this translates into poor drug levels in CNS tissue and whether drug penetrance is clinically important remain unclear. [37] In the absence of more data, no general recommendation exists to change a patient’s HAART regimen to agents with higher CSF penetrance based on cognitive status. [38]
A broad range of nano medicines is being developed to improve drug delivery to the CNS. These nano technology–based methods include disruption of blood brain barrier (BBB), development of nano particles with improved BBB permeability, uptake by brain microvascular endothelial cells via adsorptive mediated transcytosis, and cell-mediated delivery.
HAART-related reversal of some of the neurologic deficits of ADC, with patients showing improvements in motor and psychomotor speed, has been seen to be independent of CNS penetration of specific antiretroviral drugs.
When treatment fails and virologic rebound occurs, cognitive function deteriorates. Optimal doses in the presence of ADC remain unclear. If ADC develops during treatment with antiretroviral agents, additional or alternative agents should be tried.
Clinical trials have used various agents with different mechanisms of action, eg MAO-B inhibitors, antioxidants, anticonvulsants (valproic acid), NMDA receptor antagonists (memantine), and other peptides; none showed benefit superior to HAART alone. Minocycline, shown to have neuroprotective and antiinflammatory action, was able to inhibit protein kinases in apoptotic pathways. It inhibits microglial activation, release of reactive oxygen species, and production of proinflammatory cytokines.
Sometimes, depression and behavioral disturbances such as hallucinations or delusions require pharmacotherapy. However, caution is required with psychoactive drugs because of enhanced susceptibility to sedative properties and possible paradoxical reactions. Such symptoms should be treated cooperatively by specialists in internal medicine, neurology, and psychiatry. Furthermore, many drugs can upregulate the metabolism of HAART drugs, thus reducing its bioavailability.
Metabolic causes of cognitive decline, such as other infections, vitamin deficiencies, thyroid dysfunction, and liver and renal dysfunction, should be corrected in consultation with internal medicine specialists.
Case reports and small experimental studies have shown that stimulants and L-deprenyl may be helpful for attention and memory deficits.
Nutritional therapies may be considered as potential interventions in the follow-up care for patients with cognitive motor symptoms associated with HIV infection. Oxidative free-radical scavengers, such as vitamin E, the experimental antioxidant OPC-4117, and the trace mineral and antioxidant selenium, may prove therapeutically useful.
Future trials might include monoclonal antibodies against interleukins 1 and 6 and tumor necrosis factor-alpha.
Follow-up
Patients need close follow-up because of progressive dementia, unavoidable polypharmacy with possibly toxic drug levels (in particular, free drug levels), and possible development of seizures and psychosis. Patients may become incapable of self-care and require hospice care.
HIV RNA levels and CD4+ T-cell counts should be evaluated periodically to monitor clinical response and treatment resistance. HIV RNA serum levels generally reflect CSF levels until late in disease when different HIV strains may be present. [39]
Neuropsychological testing should be performed at regular intervals to monitor for improvement and responses to therapy.
Serial MRI may show decreased brain atrophy and improvement in white matter changes when patients respond to HAART.
HAART should be continued indefinitely in essentially all cases.
Depending on the severity and manifestations, patients may require nursing home placement and hospice care. Severely demented and emaciated patients are at risk for pressure injuries.
Psychotic features may require psychiatric consultation. While seizures are rare, their management is difficult, because several antiseizure drugs affect blood levels of antiretroviral drugs.
Patient Competence and Decision Making
Patients should be encouraged to prepare a living will or assign power of attorney early in their disease process. Issues of competence to make medical decisions must be addressed.
Patients may reject proposed treatments. A person’s right to autonomy cannot be challenged, provided that they have the competence to understand the risks and benefits of the treatment offered.
Competence to consent to medical treatment is defined as the “mental capacity necessary to comprehend the risks and benefits of a proposed medical treatment and its alternatives.” The only exception to this situation would be a medical emergency in which the hospital or physician may obtain consent from a surrogate, a close family member, or a spouse. Bioethics consultations may be helpful.
Only a mental health professional psychiatric crisis team, state-designated mental health professional, or peace officer can authorize involuntary hospitalization. Within 72 hours, the patient must be evaluated for mental capacity and grave disability. Grave disability is determined by the ability of the person to provide basic food, clothing, and shelter for himself or herself. If the patient is determined to be gravely disabled, the hold can be extended for 14 days, and the superior court can be petitioned for appointment of a conservator.
HIV-associated dementia may jeopardize the patient’s ability to safely operate a motor vehicle. In such cases, the clinician has a duty to advise both the patient and the Department of Motor Vehicles that it is unsafe for the patient to drive. Some patients may have severe sensory loss related to HIV-associated peripheral neuropathy and thus may be unsafe to drive on that basis. [22]
Consultations
The care of patients with AIDS dementia complex (ADC) is best accomplished with a team approach, drawing upon the expertise of specialists in various fields. A specialist with expertise in HIV (an infectious diseases or general practice physician) should oversee the antiretroviral regimen. Like all patients with HIV disease, patients with HAND require a HAART regimen that is clinically, virologically, and immunologically effective.
Psychiatric and/or psychological consultations are often indicated, as patients with ADC commonly exhibit agitation, anxiety, fatigue, depression, and other psychiatric manifestations. Psychotherapy may be helpful for patients with mild-to-moderate dementia to help them understand, mourn, and adapt to this new impairment in functioning.
As the population of patients with HIV ages, dementia is a risk, because it occurs late in life; older patients with HIV may develop Parkinson disease, frontotemporal dementia, Lewy body dementia, or Alzheimer disease unrelated to HIV. A neurologic workup by a neurologist specializing in neurobehavioral disorders may help to sort out the etiology of cognitive impairment.
The physical therapist and occupational therapist each plays a vital role in trying to maximize the functional capacity of the patient.
-
HIV-1 encephalopathy and AIDS dementia complex. CT scan of the brain of a patient with HIV associated neurocognitive disorder (HAND) shows diffuse atrophy and ventricular enlargement and attenuation of periventricular white matter.
-
HIV-1 encephalopathy and HIV associated neurocognitive disorder (HAND). T2-weighted MRI shows ventricular enlargement and large areas of hyperintense signal in the subcortical white matter of both frontal lobes.
-
HIV-1 encephalopathy and HIV associated neurocognitive disorder (HAND). Photomicrograph shows perivascular and parenchymal infiltrates of lymphocytes and macrophages. These often form microglial nodules. Image contributed by Dr Beth Levy, Saint Louis University School of Medicine, St Louis, Missouri.
-
HIV-1 encephalopathy and HIV associated neurocognitive disorder (HAND). Photomicrograph illustrates the intense astrogliosis that is characteristic of HIV encephalitis. Image contributed by Dr Beth Levy, Saint Louis University School of Medicine, St Louis, Missouri.
-
HIV-1 encephalopathy and AIDS dementia complex. Multinucleated giant cells, as shown here, are a hallmark of HIV encephalitis and harbor the virus. Image contributed by Dr Beth Levy, Saint Louis University School of Medicine, St Louis, Missouri.
Tables

What would you like to print?
- Overview
- Pathophysiology
- Epidemiology
- Prognosis
- Patient Education
- Presentation
- Physical Examination
- Diagnostic Criteria
- Staging of AIDS Dementia Complex
- Neurologic Examination in Pediatric Patients
- Differential Diagnosis
- Overview of Workup
- Cerebrospinal Fluid Analysis
- Neuroimaging
- Electroencephalography
- Neuropsychological Testing
- Histologic Findings
- Antiretroviral and Other Therapies
- Follow-up
- Patient Competence and Decision Making
- Consultations
- Show All
- Media Gallery
- References






