Practice Essentials
Infection with the encapsulated yeast Cryptococcus neoformans can result in harmless colonization of the airways, but it can also lead to meningitis or disseminated disease, especially in persons with defective cell-mediated immunity. Cryptococcosis represents a major life-threatening fungal infection in patients with severe HIV infection and may also complicate organ transplantation, reticuloendothelial malignancy, corticosteroid treatment, or sarcoidosis.
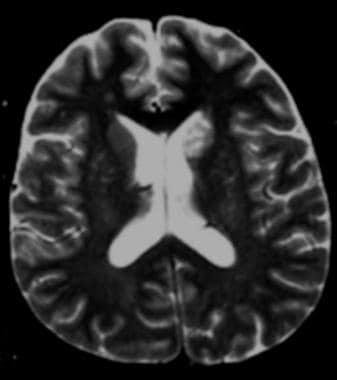 Axial T2-weighted magnetic resonance image shows clustered hyperintensities in the left caudate; these are consistent with enlarged Virchow-Robin spaces caused by small cryptococcomas.
Axial T2-weighted magnetic resonance image shows clustered hyperintensities in the left caudate; these are consistent with enlarged Virchow-Robin spaces caused by small cryptococcomas.
Signs and symptoms
The presentation in cryptococcosis varies with the site of infection and the patient’s immune status. Signs and symptoms of pulmonary cryptococcosis in immunocompetent patients are as follows:
-
Cough (54%)
-
Cough with the production of scant mucoid sputum (32%)
-
Pleuritic chest pain (46%)
-
Low-grade fever, dyspnea, weight loss, and malaise (less common)
HIV-infected patients with pulmonary cryptococcosis may present with the following:
-
Fever (84%)
-
Cough (63%)
-
Dyspnea (50%)
-
Headache (41%)
-
Weight loss (47%)
Other possible findings in pulmonary infection are as follows:
-
Pleuritic pain
-
Hemoptysis
-
Rales or pleural rub
-
Acute respiratory distress syndrome (ARDS)
Meningitis and meningoencephalitis, the most common manifestations of CNS cryptococcosis, are usually subacute or chronic in nature. HIV-infected patients may have minimal or nonspecific symptoms. Common symptoms are as follows:
-
Headache
-
Confusion
-
Lethargy
-
Obtundation
-
Coma
-
Normal or mildly elevated temperature
-
Nausea and vomiting (with increased intracranial pressure)
-
Fever and stiff neck (with an aggressive inflammatory response; less common)
-
Blurred vision, photophobia, and diplopia
-
Hearing defects, seizures, ataxia, aphasia, and choreoathetoid movements
After lung and CNS infection, the next most commonly involved organs in disseminated cryptococcosis include the skin, the prostate, and the medullary cavity of bones. Cutaneous manifestations (10-15% of cases) are as follows:
-
Papules, pustules, nodules, ulcers, or draining sinuses
-
Umbilicated papules in patients with AIDS
Other less common forms of cryptococcosis include the following:
-
Optic neuritis or endophthalmitis
-
Myocarditis
-
Chorioretinitis
-
Hepatitis
-
Peritonitis
-
Renal abscess
-
Myositis
-
Adrenal involvement
Diagnosis
The workup in patients with suspected cryptococcosis includes the following:
-
Cutaneous lesions: Biopsy with fungal stains and cultures
-
Blood: Fungal culture, cryptococcal serology, and cryptococcal antigen testing
-
Cerebrospinal fluid: India ink smear, fungal culture, and cryptococcal antigen testing
-
Urine and sputum cultures, even if renal or pulmonary disease is not clinically evident
-
In AIDS patients with cryptococcal pneumonia, culture of bronchoalveolar lavage washings
With possible CNS cryptococcosis, especially in patients who present with focal neurologic deficits or a history compatible with slowly progressive meningitis, consider obtaining a computed tomography or magnetic resonance imaging scan of the brain prior to performing a lumbar puncture. If a mass lesion is identified, do not perform a lumbar puncture to obtain spinal fluid; rather, consult a neurosurgeon for an alternative procedure.
With pulmonary cryptococcosis, radiographic findings in patients who are asymptomatic and immunocompetent may include the following:
-
Patchy pneumonitis
-
Granulomas ranging from 2-7 cm
-
Miliary disease similar to that in tuberculosis
Management
Pulmonary cryptococcosis resolves without specific therapy in most immunocompetent patients. Antifungal therapy is necessary for the following:
-
Pulmonary cryptococcosis in immunosuppressed hosts
-
CNS cryptococcosis
-
Disseminated nonpulmonary non-CNS cryptococcosis
Treatment for cryptococcal meningitis in patients with AIDS is as follows:
-
Amphotericin B deoxycholate, 0.7-1 mg/kg/day for 2 weeks, with or without
-
Flucytosine, 100 mg/kg/day in 4 divided doses for 2 weeks
-
Flucytosine speeds clearance of viable yeast from CSF but is potentially toxic, especially in patients with renal dysfunction
-
After 2 weeks, fluconazole at 400 mg/day for a minimum of 8-10 weeks
Alternative initial therapies include the following:
-
Liposomal amphotericin B 3-4 mg/kg/day for at least 2 weeks in patients at risk for renal dysfunction; in patients who have failed therapy or have a high fungal burden of disease, liposomal amphotericin B 6 mg/kg/day IV has been given safely
-
In patients intolerant of amphotericin B products, fluconazole 800-1200 mg/day plus flucytosine 100 mg/kg/day for at least 6 weeks can be used. Initial therapy should be considered successful only after CSF culture is negative for cryptococcal organisms and the patient has had significant clinical improvement.
Initial therapy should be considered successful only after CSF culture is negative for cryptococcal organisms and the patient has had significant clinical improvement.
Guidelines published in 2000 recommended maintenance therapy with fluconazole at 200 mg/day for life. [3] Guidelines published in 2002 supported discontinuation of suppressive therapy if CD4 counts remained greater than 200 cells/µL but reinstitution if the CD4 counts fall to fewer than 200 cells/µL. [4] Guidelines published in 2010 support discontinuation of suppressive therapy when the CD4 count exceeds 100 cells/µL and HIV viral load is undetectable or very low for more than 3 months. However, reinstitution of maintenance therapy should be considered if the CD4 cell count falls to less than 100 cells/µL. [5]
Control of CSF pressure is critical to the patient’s survival. An initial opening pressure of 250 mm H2O or greater must be reduced and kept around 200 H2O throughout therapy. In some patients, this may require daily spinal taps or a spinal fluid drain until pressures are controlled. In rare cases, control of elevated CSF pressures may require a ventriculoperitoneal shunt. Failure to control CSF pressure may result in blindness, permanent neurologic deficits, or death.
-
Monitor CSF pressure during the initial phase of therapy
-
If the opening pressure exceeds 250 mm H 2O, remove CSF to reduce the closing pressure to below 200 mm H 2O or at least 50% of the elevated opening pressure
-
Mannitol has no proven value in reducing pressure in cryptococcal meningitis. Acetazolamide or corticosteroids to control CSF pressure unassociated with immune reconstitution inflammatory syndrome (IRIS) should also be avoided.
-
In severe IRIS complicating therapy of HIV-associated cryptococcal meningitis, prednisone 0.5-1.0 mg/kg/day or dexamethasone can be used to control signs or symptoms of severe CNS disease.
IRIS may occur in patients with AIDS or other severe immunosuppressive conditions. In patients with AIDS who are not on antiretroviral therapy but who develop cryptococcal meningitis, initiation of antiretrovirals early in the administration of anticryptococcal therapy may result in a rapid worsening of the patient’s condition. This worsening is believed to result from sudden enhancement in the patient’s immune response to the infection, leading to worsening signs and symptoms or even death.
In patients without AIDS, treatment of cryptococcal meningitis is as follows:
-
Amphotericin B (0.7-1 mg/kg/day) alone for 6-10 weeks or in combination with flucytosine (100 mg/kg/day in 4 divided doses) for 2 weeks, followed by fluconazole for a minimum of 10 weeks
-
Base therapy duration on CSF examination results
-
Consider weekly CSF examination until culture conversion is documented and cultures remain negative for 4 weeks
-
CSF protein abnormalities may persist for years despite successful therapy; thus, an elevated CSF protein as the only residual abnormality should not dictate prolonging therapy
Pulmonary cryptococcosis can be treated with observation only, if the following criteria are met:
-
CSF chemistry parameters are normal
-
CSF culture, CSF cryptococcal antigen, India ink preparation, and serology results are negative
-
Urine culture results are negative
-
The pulmonary lesion is small and stable or shrinking
-
The patient has no predisposing conditions for disseminated disease
Antifungal treatment for cryptococcal pulmonary disease is as follows:
-
Mild-to-moderate disease: Fluconazole for 6-12 months, itraconazole for 6-12 months, or amphotericin B
-
Severe disease: Amphotericin B (0.7-1 mg/kg/day) plus flucytosine (100 mg/kg/day) for 6-10 weeks, or for 2 weeks followed by fluconazole at 400 mg/kg/day for at least 10 weeks, possibly followed by further consolidation therapy for 6-12 months
Background
Cryptococcus neoformans is an encapsulated yeast. In 1894, Busse, a pathologist, first described the yeast in a paper he presented to the Greifswald Medical Society. Busse isolated the yeast from the tibia of a 31-year-old woman, noted its resistance to sodium hydroxide, and published the case report that same year. [6] The following year, a surgeon named Buschke reported the same isolate from the same patient, thus establishing the early eponym of Busse-Buschke disease. [7] This single case served to identify a new yeast and to prove its pathogenic potential.
Since the initial reports, researchers have identified the diverse spectrum of host responses to cryptococcal infection. The responses range from a harmless colonization of the airways and asymptomatic infection in laboratory workers (resulting in only a positive skin test finding) to meningitis or disseminated disease. Although virulence in animals and, possibly, humans varies among strains of cryptococci, virulence probably plays a relatively small role in the outcome of an infection. The crucial factor is the immune status of the host.
The most serious infections usually develop in patients with defective cell-mediated immunity. For example, patients with AIDS, patients undergoing organ transplantation, patients with reticuloendothelial malignancy, patients undergoing corticosteroid treatment (but not those with neutropenia or immunoglobulin deficiency), and patients with sarcoidosis develop the most serious cryptococcal infections.
With the global emergence of AIDS, the incidence of cryptococcosis is increasing and now represents a major life-threatening fungal infection in these patients.
Mycology
Although the genus Cryptococcus contains more than 50 species, only C neoformans and Cryptococcus gattii are considered principal pathogens in humans. Previously, C neoformans was defined as having two varieties—var neoformans and var gattii. However, based on the elucidation of the genomic sequences, C neoformans and C gattii are now considered two distinct species. These two species have 5 serotypes based on antigenic specificity of the capsular polysaccharide; these include serotypes A, D, and AD (C neoformans) and serotypes B and C (C gattii).
C neoformans is the most common species in the United States and other temperate climates throughout the world and is found in aged pigeon droppings. Until recently, C gattii was found principally in tropical and subtropical climates. C gattii is not associated with birds but grows in the litter around certain species of eucalyptus trees (ie, Eucalyptus camaldulensis, Eucalyptus tereticornis). A 2016 epidemiological study performed in Bogota, Columbia, showed that Cneoformans also has a predilection for eucalyptus tree species, similar to Cgattii. [8]
Worldwide, C neoformans serotype A causes most cryptococcal infections in immunocompromised patients, including patients infected with HIV. For unknown reasons, Cgattii rarely infects persons with HIV infection and other immunosuppressed patients. Patients infected with C gattii are usually immunocompetent, respond slowly to treatment, and are at risk for developing intracerebral mass lesions (eg, cryptococcomas). A 2016 epidemiological study revealed that Cryptococcus tetragattii (AFLP7/VGIV), one of the five recognized genotypes of Cgattii sensu lato, is associated with a higher prevalence of cryptococcal meningitis among HIV-infected patients in Zimbabwe. [9]
C neoformans reproduces by budding and forms round yeastlike cells that are 3-6 µm in diameter. Within the host and in certain culture media, a large polysaccharide capsule surrounds each cell. C neoformans forms smooth, convex, yellow or tan colonies on solid media at 20-37°C (68-98.6°F). This fungus is identified based on its microscopic appearance, biochemical test results, and ability to grow at 37°C (98.6°F); most nonpathogenic Cryptococcus strains do not grow at this temperature. In addition, C neoformans does not assimilate lactose and nitrates or produce pseudomycelia on cornmeal or rice-Tween agar.
Most strains of C neoformans can use creatinine as a nitrogen source, which may partially explain the growth of the organism in creatinine-rich avian feces. Another useful biochemical characteristic of C neoformans, which distinguishes it from nonpathogenic strains, is its ability to produce melanin. The fungal enzyme phenol oxidase acts on certain substrates (eg, dihydroxyphenylalanine, caffeic acid) to produce melanin.
C gattii contains genotypes VGI and the more commonly identified VGIIa and VDIIb. Cryptococcus species can reproduce via same-sex mating, and VGIIa may have arisen from the same-sex mating of VGIIb and another strain that has yet to be identified.
In 1976, Kwon-Chung described the perfect (ie, sexual, teleomorphic) form of C neoformans, which was named Filobasidiella neoformans. Prior to the identification of F neoformans, which is mycelial, C neoformans was considered a monomorphic yeast. F neoformans results from the mating of suitable strains of serotypes A and D. The perfect state of C gattii is Filobasidiella bacillispora and results from the mating of serotypes B and C. Some strains of A and D can mate with strains of B and C.
Epidemiology
C neoformans is distributed worldwide. Most cases of cryptococcosis involve serotypes A and D. Serotypes B and C, C gattii, are most common in tropical and subtropical areas and can be isolated from certain species of eucalyptus trees and the air beneath them. C neoformans, which is recovered from aged pigeon feces, bird nests, and guano, is invariably serotype A or D. Although serotypes A and D exist in high concentrations in the pigeon feces, the fungus does not infect the birds. In moist or desiccated pigeon excreta, C neoformans may remain viable for 2 years or longer. The pigeon fanciers are known to have higher anti–C. neoformans antibodies titers than normal population. [10] In saprobic environments, C neoformans grows unencapsulated; however, unencapsulated strains regain their virulence following reacquisition of their polysaccharide capsule. C gattii usually causes disease in patients with intact cell-mediated immunity.
Naturally occurring cryptococcosis occurs in both animals and humans, but neither animal-to-human transmission nor person-to-person respiratory transmission via the respiratory route has been documented. Transmission via organ transplantation has been reported when infected donor organs were used. C neoformans causes the vast majority of cryptococcal infections in immunosuppressed hosts, including patients with AIDS, whereas C gattii causes 70%-80% of cryptococcal infections among immunocompetent hosts. AIDS, decompensated liver cirrhosis, cellular mediated immunity suppressive regimens, and autoimmune disorders have been established as possible risk factors in the causation of invasive C neoformans disease. [11]
Although C neoformans is found worldwide, C gattii is usually identified in subtropical areas such as Australia, South America, Southeast Asia, and Central and sub-Saharan Africa. In the United States, C gattii is found in Southern California and more recently in the states of Washington and Oregon.
As noted above, C gattii may be found in association with several different trees, such as river red gum trees (E camaldulensis) and forest red gum trees (E tereticornis). Infection is acquired by inhalation of air-borne propagules that infect the lungs and may result in fungemia, leading to CNS involvement.
In 1999, C gattii emerged on Vancouver Island, British Columbia, Canada. Infections were reported among residents and visitors to the island, as well as among domesticated and wild animals. Disease has been most often identified in cats, dogs and ferrets. Marine mammals have also been infected. Vectors can disperse the spores from an endemic area to a previously unaffected area. This may have been the route of spread in the case of Vancouver Island. Since 2003, cryptococcal disease has become a provincially notifiable infection in British Columbia. Isolates have been identified in coastal Douglas fir and coastal western hemlock bioclimatic zones. C gattii has been identified subsequently in the states of Washington and Oregon.
The incidence of infection related to age, race, or occupation does not significantly differ. Cryptococcal antibodies acquisition begins at as early as one year of age. At the age of 5 years, 70% of children react with C. neoformans antigen. [12] Healthy persons with a history of exposure to pigeons or bird feces and laboratory workers exposed to an aerosol of the organism have a higher rate of positive delayed hypersensitivity skin reactions to cryptococcal antigen or cryptococci. Occasionally, laboratory accidents result in transmission of C neoformans, but pulmonary and disseminated disease is rare in this setting. Accidental cutaneous inoculation with C neoformans causes localized cutaneous disease.
A report from British Columbia, Canada indicates that risk factors for infection by C gattii include steroid use and underlying pulmonary disease. [13] The authors also report a predilection for individuals older than 50 years, current smokers, and those with immunosuppression due to HIV or invasive malignancy.
The advent and increased use of anti-TNF and anti-CD 54 has posed an increased risk of contracting cryptococcosis, along with an increased risk of delayed diagnosis. [14, 15]
Pathophysiology
Of the more than 50 species that comprise the genus Cryptococcus, human disease is primarily associated with C neoformans and C gattii. Animal models provide much of the understanding of the pathogenesis and the host defense mechanisms involved in cryptococcal infections. Cryptococcosis is acquired in two routes; after exposure to C. neoformans in immunocompromised, causing rapidly progressive cryptococcosis; the second is with a phase of latency followed by reactivation and dissemination. The concept of latency has been validated in C. neoformans. [16] The organism is primarily transmitted via the respiratory route, but not directly from human to human.
Following inhalation, the yeast spores are deposited into the pulmonary alveoli, where they must survive the neutral-to-alkaline pH and physiologic concentrations of carbon dioxide before they are phagocytized by alveolar macrophages. Glucosylceramide synthase (GCS) has been identified as an essential factor in the survival of C neoformans in this extracellular environment. [17] Although GCS is a critical factor in extracellular survival of the yeast, the yeast no longer requires GCS to survive the intracellular, more acidic, environment within the macrophage once it is phagocytized by alveolar macrophages.
Unencapsulated yeast are readily phagocytosed and destroyed, whereas encapsulated organisms are more resistant to phagocytosis. The cryptococcal polysaccharide capsule has antiphagocytic properties and may be immunosuppressive. The antiphagocytic properties of the capsule block recognition of the yeast by phagocytes and inhibit leukocyte migration into the area of fungal replication.
The host response to cryptococcal infection includes both cellular and humoral components. Animal models demonstrate that natural killer cells participate in the early killing of cryptococci and, possibly, antibody-dependent cell-mediated killing. In vitro monocyte-derived macrophages, natural killer cells, and T lymphocytes can inhibit or kill cryptococci. A successful host response includes an increase in helper T-cell activity, skin test conversion, and a reduction in the number of viable organisms in the tissues. In addition to cellular mechanisms, anticryptococcal antibodies and soluble anticryptococcal factors have been described. Antibodies to cryptococcal antigens play a critical role in enhancing the macrophage- and lymphocyte-mediated immune response to the organism. Researchers have used monoclonal antibodies to capsular polysaccharide to passively immunize mice against C neoformans.
C neoformans infection is usually characterized by little or no necrosis or organ dysfunction until late in the disease. Organ damage may be accelerated in persons with heavy infections. The lack of identifiable endotoxins or exotoxins may be partly responsible for the absence of extensive necrosis early in cryptococcal infections. Organ damage is primarily due to tissue distortion secondary to the expanding fungal burden. Extensive inflammation or fibrosis is rare. The characteristic lesion of C neoformans consists of a cystic cluster of yeast with no well-defined inflammatory response. Well-formed granulomas are generally absent.
C neoformans can cause an asymptomatic pulmonary infection followed later by the development of meningitis, which is often the first indication of disease. If limited to the lungs, C neoformans infection may cause pneumonia, poorly defined mass lesions, pulmonary nodules, and, rarely, pleural effusion. Although immune defects are common in patients with meningitis or disseminated infection, patients with disease that is confined to the lungs are usually immunocompetent.
Epidemiology
Frequency
United States
Prior to 1946, only 200 patients with cryptococcal disease had been reported in the medical literature. The development and use of corticosteroids and improvement in patient survival with some malignancies increased the reported incidence of cryptococcal disease. Since the mid 1980s, most cryptococcal disease has occurred in patients with AIDS. A study published in March 2005 that reviewed data from 1981-2000, the first 2 decades of the AIDS epidemic, showed that the annual incidence per million person-years was 19 cases in men and 2.6 cases in women. The highest incidence occurred from 1981-1992; afterward, the incidence began to decline. In women, the peak incidence occurred in 1997. The overall incidence in cryptococcal disease decreased and preceded the availability of of highly active antiretroviral therapy for AIDS.
Approximately 7%-15% of patients with AIDS develop cryptococcal infections. In 1993, the US Centers for Disease Control and Prevention reported that 6% of 274,150 patients with AIDS developed cryptococcal disease. Furthermore, patients with AIDS-associated cryptococcal infections now account for 80%-90% of all patients with cryptococcosis.
International
C neoformans has a worldwide distribution and, similar to in the United States, preferentially infects immunosuppressed individuals, especially those with AIDS. Cryptococcal meningitis associated with HIV infection is responsible for more than 600,000 deaths per year worldwide. [18] In sub-Saharan Africa, 15%-30% of all patients with AIDS develop cryptococcal disease. However, in some areas, such as Zimbabwe, 88% of patients with AIDS have cryptococcal infection as their AIDS-defining illness. Most case reports of C gattii have been from Australia, with a few case reports from the southern California coast and tropical regions of Central and South America. As mentioned above, some recent cases have been reported from Vancouver, British Columbia, Canada and the states of Washington and Oregon, United States.
An outbreak of a hypervirulent strain of C gattii has been linked to climate changes in the northwestern United States and British Columbia. [19]
Mortality/Morbidity
Prior to the use of amphotericin B (Throughout this article, the term amphotericin B refers to amphotericin B desoxycholate.), cryptococcal meningitis and disseminated disease were invariably fatal; however, with the availability of amphotericin B, lipid preparations of amphotericin B, flucytosine, fluconazole, and other azoles, the mortality rate of cryptococcal disease dramatically decreased. In 1995, Speed and Dunt reported a 14% mortality rate among patients with cryptococcal disease who were treated with amphotericin B plus flucytosine and a 28% mortality rate among patients treated with other regimens. [20]
Race
No clear racial predilection has been reported for either cryptococcal infection or disease. No occupational predilection has been defined.
Sex
In most studies, cryptococcal disease is reportedly more common in men than in women.
Age
In a 1972 review, Lewis and Rabinovich reported that almost two thirds of patients with cryptococcal disease were older than 40 years [21] ; furthermore, in patients aged 50 years and older, cryptococcal disease was more than 3 times as common in men as in women. However, the pandemic of AIDS has led to a simultaneous and dramatic rise in the incidence of cryptococcal disease and a reduction in the average age of affected patients.
-
Axial T2-weighted magnetic resonance image shows clustered hyperintensities in the left caudate; these are consistent with enlarged Virchow-Robin spaces caused by small cryptococcomas.








