Practice Essentials
Factor V is an essential component in the blood coagulation cascade. Inherited or acquired deficiencies in factor V are rare causes of bleeding disorders. [1, 2]
Factor V deficiency is also known as Owren disease. Dr. Paul Owren identified this defect in Norway in 1943. Using relatively primitive technology, he was able to deduce the existence of a fifth component required for fibrin formation, which he named factor V, thus beginning the era of Roman numerology for coagulation factors.
Dr. Owren's work defined factor V as the activity in normal plasma that corrected the prothrombin time (PT) of the plasma in a patient with factor V deficiency. Factor V deficiency has also been called parahemophilia, since hemarthrosis can occur with severe deficiencies and with increased bleeding time. [3, 4]
Pathophysiology
Factor V is an essential component in the blood coagulation cascade. Factor V is synthesized in the liver and possibly in megakaryocytes. Factor V circulates in an inactive form. During coagulation, factor V is converted to the active cofactor, factor Va, via limited proteolysis by the serine protease a-thrombin. Factor Va and activated factor Xa form the prothrombinase complex. The prothrombinase complex is responsible for the rapid conversion of the zymogen prothrombin to the active serine protease a-thrombin. [5, 6] Thrombin cleaves fibrinogen to form fibrin, leading to the ultimate step in coagulation, the formation of a fibrin clot. [7] See images below.
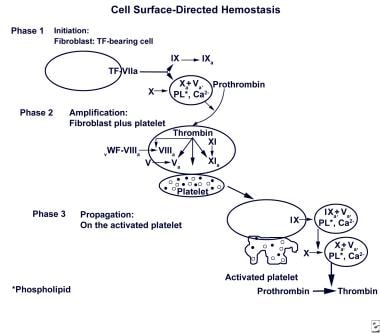 Cell surface-directed hemostasis. Initially, a small amount of thrombin is generated on the surface of the tissue factor (TF)–bearing cell. Following amplification, the second burst generates a larger amount of thrombin, leading to fibrin (clot) formation. Adapted from Hoffman and Monroe, Thromb Haemost 2001, 85(6): 958-65.
Cell surface-directed hemostasis. Initially, a small amount of thrombin is generated on the surface of the tissue factor (TF)–bearing cell. Following amplification, the second burst generates a larger amount of thrombin, leading to fibrin (clot) formation. Adapted from Hoffman and Monroe, Thromb Haemost 2001, 85(6): 958-65.
Inherited factor V deficiency is a rare autosomal recessive disorder that is associated with an abnormal factor V plasma level. Numerous mutations in the F5 gene have been identified in these patients. [5, 8, 9, 10, 11, 12]
Another rare autosomal recessive disorder, combined factor V and factor VIII deficiency, results from mutations in either LMAN1 (lectin mannose binding–1) or MCFD2 (multiple coagulation factor deficiency gene 2). Alterations in the proteins encoded by those two genes interfere with efficient secretion of factors V and FVIII. [13] The LMAN1 mutation is more common in Middle Eastern populations and MCFD2 is more common among Indian and European populations. [14]
Acquired factor V deficiency is a rare clinical condition in which the development of antibodies to factor V (factor V inhibitors) leads to hemorrhagic complications of varying severity. The addition of normal plasma cannot correct the prolonged PT and activated partial thromboplastin time (aPTT). Factor V inhibitors can occur after surgery, childbirth, use of bovine thrombin or medications, and in patients with autoimmune diseases and certain neoplasms. [15, 16] Acquired factor V deficiency is idiopathic in approximately 15% of cases. [17]
Factor V Leiden is a completely different inherited disorder that involves a single point mutation in the factor V gene. Factor V activity levels in patients with factor V Leiden are normal. [18] Proteolytic inactivation of factor Va and factor VIIIa by activated protein C (APC) normally limits clot formation; however, factor V Leiden resists inactivation by APC. Consequently, individuals who are homozygous for factor V Leiden have a high incidence of thrombosis. For more information, see Hereditary and Acquired Hypercoagulability.
Etiology
Factor V deficiency is caused by a large number of genetic abnormalities. The deficiency is a rare bleeding disorder whose genetic bases have been characterized in only a limited number of cases. [9] The inheritance of factor V deficiency is autosomal recessive, with varying expressivity in the heterozygote; however, other modes of inheritance have been described. Heterozygotes have lowered levels of factor V but probably never bleed abnormally.
Consanguinity has been observed in families with factor V deficiency, related to its autosomal recessive inheritance. Heterozygous deficiency states are generally unrecognized because of a lack of significant clotting time prolongation or bleeding risk.
Epidemiology
Frequency
International
Fewer than 200 cases of congenital factor V deficiency have been reported worldwide since 1943. Homozygous factor V deficiency is rare, occurring in approximately 1 per million population.
Delev et al presented 39 German patients with factor V deficiency. [8] In 36 cases with an identifiable causative mutation, 20 patients were heterozygous for the mutation, whereas 9 were homozygous, 6 were compound heterozygous, and 1 proband was pseudohomozygous. [8] There were no mutations found in the remaining 3 patients.
The investigators identified 33 uniquely different mutations of a total 42 genetic mutations: 19 missense mutations, 8 nonsense mutations, 4 small deletions, and 2 splice site mutations. [8] Of the 33 unique mutations, 23 were novel sequence variations not previously reported, and all changes found in exon 13 led to null alleles as nonsense mutations or small deletions.
Race-, sex-, and age-related demographics
No apparent racial predilection for factor V deficiency exists. Factor V deficiency affects males and females with equal frequency.
Combined factor V and factor VIII deficiency is more prevalent in areas of the Middle East, Mediterranean, and South Asia where consanguineous marriage is more common. [14]
Factor V deficiency affects persons of all ages. The age at presentation indirectly varies with the severity of disease.
Prognosis
The prognosis of patients with factor V deficiency is good with diagnosis and proper treatment. The severity of factor V deficiency varies from bruising to lethal hemorrhage. Complications of factor V deficiency are directly related to the site of bleeding (eg, hemarthrosis, intracranial hemorrhage, uncontrolled postoperative bleeding).
Recurrent miscarriage has been reported in women with factor V deficiency. [19]
Patient Education
Give patients and families instruction and educational materials to enable them to understand factor V deficiency. For patient education information, see Hemophilia.
-
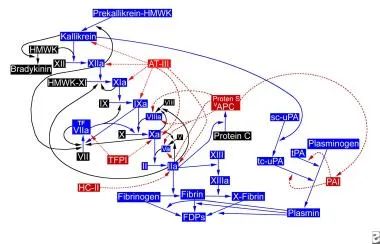
Antithrombin sites of action.
-
Cell surface-directed hemostasis. Initially, a small amount of thrombin is generated on the surface of the tissue factor (TF)–bearing cell. Following amplification, the second burst generates a larger amount of thrombin, leading to fibrin (clot) formation. Adapted from Hoffman and Monroe, Thromb Haemost 2001, 85(6): 958-65.








