Practice Essentials
Early pregnancy loss, or miscarriage, is the loss of a pregnancy before 20 weeks.
In the first trimester, embryonic causes of spontaneous abortion are the predominant etiology and account for 80-90% of miscarriages (see the image below).
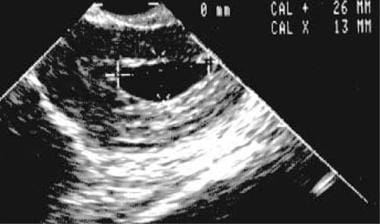 Second transvaginal sonogram obtained 1 week after the initial study fails to demonstrate fetal development. This confirms the diagnosis of an embryonic pregnancy.
Second transvaginal sonogram obtained 1 week after the initial study fails to demonstrate fetal development. This confirms the diagnosis of an embryonic pregnancy.
Signs and symptoms
Patients with spontaneous complete abortion usually present with a history of vaginal bleeding, abdominal pain, and passage of tissue. After the tissue passes, the vaginal bleeding and abdominal pain subsides.
Other symptoms, such as fever or chills, are more characteristic of infection, such as in a septic abortion. Septic abortions need to be treated immediately, otherwise they may be life-threatening.
Patients who are pregnant and bleeding vaginally need immediate evaluation.
See Clinical Presentation for more detail.
Diagnosis
Examination in women with suspected early pregnancy loss includes the following:
-
Assessment of hemodynamic stability, including vital signs
-
Abdomen: In a complete abortion, the abdomen is benign, with normal bowel sounds, no distention, no rebound, no hepatosplenomegaly, and mild suprapubic tenderness; complete abortion is unlikely if rebound tenderness or a distended abdomen is present— instead, assume ectopic pregnancy (and promptly initiate appropriate therapy)
-
Pelvis: In a complete abortion, some blood may be present on the perineum or vagina, but there is limited active bleeding, no cervical motion tenderness, a closed cervical canal, smaller uterus than expected for dates, uterus and adnexa nontender to mildly tender, no adnexal masses (unless a corpus luteum is still palpable)
The pelvic examination checklist includes assessment of the following:
-
Source of bleeding (cervical os)
-
Intensity of bleeding (active, heavy, clots)
-
Any presence or passage of tissue
-
Cervical motion tenderness (increases suspicion for ectopic pregnancy)
-
Cervical os closed for complete or threatened abortion (If it is open, consider inevitable or incomplete abortion.)
-
Uterine size and tenderness
-
Adnexal masses (suspicious for ectopic pregnancy)
Testing
Laboratory studies used in the evaluation of early pregnancy loss include the following:
-
Complete blood count with differential
-
Levels of beta-human chorionic gonadotropin
-
Blood type and screen (possible crossmatch)
-
Disseminated intravascular coagulopathy profile in women with significant bleeding (platelet count, fibrinogen level, prothrombin time, activated partial prothrombin time)
-
Urinalysis
Imaging studies
Perform pelvic ultrasonography using a vaginal probe to rule out an ectopic pregnancy, retained products of conception, hematometra, or other etiologies.
Procedures
When the diagnosis is unclear, the following procedures may be performed:
-
Culdocentesis
-
Diagnostic dilation and curettage
See Workup for more detail.
Management
A complete abortion usually needs no further treatment, medically or surgically. With missed, incomplete, or inevitable abortion present before 13 weeks' gestation, treatment may include misoprostol as an alternative to surgery or performance of suction dilation and curettage.
An ectopic pregnancy may be treated medically (methotrexate) or surgically (laparoscopy, laparotomy), depending on the clinical situation.
Pharmacotherapy
For a complete abortion, no medication is likely to be needed. Usually, the uterus contracts well after expelling the entire contents and the cervix is closed. The risk for infection is minimal.
The following medications may be used in women with early pregnancy loss:
-
Immune globulins (eg, Rho (D) immune globulin)
-
Ergot alkaloid and derivatives (eg, methylergonovine)
-
Antimetabolite antineoplastic agents (eg, methotrexate)
-
Prostaglandins (eg, misoprostol)
Surgical option
Surgical intervention may include the following:
-
Complete abortion: None
-
Inevitable and incomplete abortions: Suction dilation and curettage
-
Septic abortion: Broad spectrum antibiotic therapy and suction dilation and curettage
-
Ectopic pregnancy: Treat medically for appropriate patients; the rest require surgery such as linear salpingostomy or partial or complete salpingectomy via laparoscopy or laparotomy
-
Unclear diagnosis: Diagnostic suction dilation and curettage with diagnostic laparoscopy
See Treatment and Medication for more detail.
Background
An abortion is the spontaneous or induced loss of an early pregnancy. The period of pregnancy prior to fetal viability outside of the uterus is considered early pregnancy. Most consider early pregnancy to end at 20 weeks' gestation or when the fetus weighs 500 grams. The term miscarriage is used often in the lay language and refers to spontaneous abortion.
Pathophysiology
A spontaneous abortion is a process that can be divided into 4 stages—threatened, inevitable, incomplete, and complete. The 4 stages of abortion form a continuum. Most studies do not differentiate separately between the epidemiology and pathophysiology of each entity.
The combination of oxidative stress, a more hypoxic environment, and defective placentation may lead to increased serum ischemia-modified albumin (IMA) concentrations, which in turn, may play a role in the pathophysiology of early pregnancy loss. [1]
Threatened abortion
Threatened abortion consists of any vaginal bleeding during early pregnancy without cervical dilatation or change in cervical consistency. Usually, no significant pain exists, although mild cramps may occur. More severe cramps may lead to an inevitable abortion.
Threatened abortion is very common in the first trimester; about 25-30% of all pregnancies have some bleeding during the pregnancy. Less than one half proceed to a complete abortion. On examination, blood or brownish discharge may be present in the vagina. The cervix is not tender, and the cervical os is closed. No fetal tissue or membranes have passed. The ultrasound shows a continuing intrauterine pregnancy. If an ultrasound was not performed previously, it is required at this time to rule out an ectopic pregnancy, which could present similarly. If the uterine cavity is empty on ultrasound, obtaining a human chorionic gonadotropin (hCG) level is necessary to determine if the discriminatory zone has been passed.
The discriminatory zone is the level of hCG beyond which a normal, singleton, intrauterine pregnancy is consistently visible by ultrasound. The discriminatory zone may vary depending on a number of factors, including the hCG assay type and reference calibration standard used, ultrasound equipment resolution, the skill and experience of the sonographer, and patient factors (eg, obesity, leiomyomas, uterine axis, multiple gestations). Also, the discriminatory zone will vary depending on whether the ultrasound is performed abdominally or vaginally. Therefore, having a universal discriminatory zone is difficult, and it optimally should be calculated at each site.
Some studies recommend that a gestational sac should be visualized by 5.5 weeks' gestation; a gestational sac should be visualized with an hCG level of 1500-2400 mIU/mL for transvaginal ultrasound or with an hCG level over 3000 mIU/mL for a transabdominal ultrasound. If the hCG level is higher than the discriminatory zone and no gestational sac is visualized in the uterus, then consider that an ectopic pregnancy may be present. [2] Multiple gestations are an exception and can have higher hCG levels earlier in gestation because more hCG is being made by the trophoblasts from the multiple implantations. Thus, the gestational sac(s) may not be visible on ultrasound despite the hCG levels being higher than the discriminatory zone. Even with multiple gestations, the gestational sacs should be visible at a similar gestational age as singleton gestations or about 6 weeks' gestation if the dating is good.
A clinician should be concerned about ectopic pregnancy but cannot make the diagnosis of ectopic pregnancy just because the hCG level is higher than the discriminatory zone and the uterus appears empty on ultrasound. Many of these pregnancies are abnormal intrauterine pregnancies as opposed to ectopic. One needs to take into consideration the clinical history, and estimated gestational age by LMP or date of conception, if known. A positive pregnancy test result and an ultrasound that does not reveal the location is known as a pregnancy of unknown location (PUL). [3] Occasionally, a normal intrauterine pregnancy does result. Depending on the clinical scenario, a clinician may choose to observe this patient with serial hCG levels and ultrasonography instead of intervening, or a clinician may need to intervene depending on the situation.
Inevitable abortion
Inevitable abortion is an early pregnancy with vaginal bleeding and dilatation of the cervix. Typically, the vaginal bleeding is worse than with a threatened abortion, and more cramping is present. No tissue has passed yet. On ultrasound, the products of conception are located in the lower uterine segment or the cervical canal.
Incomplete abortion
Incomplete abortion is a pregnancy that is associated with vaginal bleeding, dilatation of the cervical canal, and passage of products of conception. Usually, the cramps are intense, and the vaginal bleeding is heavy. Patients may describe passage of tissue, or the examiner may observe evidence of tissue passage within the vagina. Ultrasound may show that some of the products of conception are still present in the uterus.
Complete abortion
Complete abortion is a completed miscarriage. Typically, a history of vaginal bleeding, abdominal pain, and passage of tissue exists. After the tissue passes, the patient notes that the pain subsides and the vaginal bleeding significantly diminishes. The examination reveals some blood in the vaginal vault; a closed cervical os; and no tenderness of the cervix, uterus, adnexa, or abdomen. The ultrasound demonstrates an empty uterus.
Missed abortion
A fifth term that does not follow the continuum but is important to be aware of is missed abortion. A missed abortion is a nonviable intrauterine pregnancy that has been retained within the uterus without spontaneous abortion. Typically, no symptoms exist besides amenorrhea, and the patient finds out that the pregnancy stopped developing earlier when a fetal heartbeat is not observed or heard at the appropriate time. An ultrasound usually confirms the diagnosis. No vaginal bleeding, abdominal pain, passage of tissue, or cervical changes are present.
Etiology
In the first trimester, embryonic causes of spontaneous abortion are the predominant etiology and account for 80-90% of miscarriages (see the image below).
Second transvaginal sonogram obtained 1 week after the initial study fails to demonstrate fetal development. This confirms the diagnosis of an embryonic pregnancy.
One study suggested that an inflammatory reaction occurs in normal pregnancy and may be disrupted during miscarriage. [4]
Genetic abnormalities within the embryo (ie, chromosomal abnormalities) are the most common cause of spontaneous abortion and account for 50-65% of all miscarriages. The most common single chromosomal anomaly is 45,X karyotype, with an incidence of 14.6%. Trisomies are the single largest group of chromosomal anomalies and account for approximately one half of all anomalies associated with miscarriage. Trisomy 16 is the most common trisomy found. Approximately 20% of genetic abnormalities are triploidies.
Teratogenic and mutagenic factors may also play a role in spontaneous abortion, but quantification is difficult. Iatrogenic causes include Asherman syndrome.
Maternal causes of spontaneous miscarriage include the following:
-
Genetic: Maternal age is directly related to the aneuploidy risk (>30% in people aged 40 y). Couples with recurrent miscarriages have a 2-3% incidence of a parental chromosomal anomaly (ie, balanced translocation).
-
Structural abnormalities of the reproductive tract include the following: Congenital uterine defects (particularly uterine septum), fibroids, cervical incompetence
Acute maternal factors include the following:
-
Corpus luteum deficiency
-
Active infection (eg, rubella virus, cytomegalovirus, Listeria infection, toxoplasmosis, malaria, brucellosis, human immunodeficiency virus (HIV), dengue fever, influenza, as well as vaginal infection with bacterial vaginosis [5, 6] )
Chronic maternal health factors include the following:
-
Poorly controlled diabetes mellitus (A successful pregnancy requires much tighter control.)
-
Renal disease
-
Untreated thyroid disease: A meta-analysis evaluating the association between thyroid autoantibodies and miscarriage and preterm birth in women with normal thyroid function found a strong link between maternal thyroid autoantibodies and miscarriage and preterm birth. [7] Evidence suggests that treatment with levothyroxine may attenuate the risks.
-
Severe hypertension
-
Antiphospholipid syndrome
Exogenous factors include the following:
-
Tobacco
-
Alcohol
-
Cocaine
-
Caffeine (high doses)
Independent risk factors for a spontaneous miscarriage include the following [8, 9, 10] :
-
Advanced age
-
Extremes of age
-
Feeling stressed
-
Advanced paternal age
Symptoms of vaginal bleeding but not abdominal pain are associated with increased risk of miscarriage. One paper suggests that miscarriage can occur in about 50% of patients who present with threatened abortion.
Gestational exposure to nonaspirin NSAIDs may increase the risk for miscarriage. Nakhai-Pour et al identified 4705 women who had spontaneous abortions by 20 weeks’ gestation. Each case was matched to 10 control subjects (n=47,050) who did not have a spontaneous abortion. In the women who had a miscarriage, 352 (7.5%) were exposed to a nonaspirin NSAID, whereas NSAID exposure was lower (1213 exposed [2.6%]) in women who did not have a miscarriage. [11]
A study by Hahn et al indicates that obesity increases the likelihood of spontaneous abortion, with the risk being highest in the first two months of pregnancy. The study, of 5132 women, found that compared with women of normal weight, women with a body mass index of 30 or above had a hazard ratio (HR) for spontaneous abortion of 1.34 prior to eight weeks’ gestation, after which it dropped to 1.23. The data also indicated that small stature (height < 166 cm) and a low waist-to-hip ratio are additional risk factors for spontaneous abortion. However, neither waist circumference nor the location of typical weight gain was found to significantly affect the risk. [12]
Select vaginal bacteria may also increase the risk of early pregnancy loss. A multicenter study of 418 pregnant of whom 74 had a miscarriage showed that the greatest risk of miscarriage among young women with high levels of was bacterial vaginosis-associated bacteria 3 (BVAB3). [5]
A Danish nationwide study by Mølgaard-Nielsen et al found that 147 of 3315 women exposed to oral fluconazole in their 7th through 22nd weeks of gestation experienced a spontaneous abortion compared to 563 of the 13,246 unexposed pregnancies. [13, 14]
Nausea and vomiting were associated with a reduced risk for pregnancy loss among women with 1 or 2 prior pregnancy losses in a study by Hinkle et al. [15, 16]
Epidemiology
United States statistics
The overall miscarriage rate is reported as 15-20%, which means 15-20% of recognized pregnancies result in miscarriage. The frequency of spontaneous miscarriage increases further with maternal age. With the development of highly sensitive assays for hCG levels, pregnancies can be detected prior to the expected next period. When these highly sensitive hCG assays are used early, the magnitude of pregnancy loss significantly increases to about 60-70%. Late implantation by the conceptus beyond the usual 8-10 days after ovulation also has an increased risk of miscarriage.
About 80% of miscarriages occur within the first trimester. The frequency of miscarriage decreases with increasing gestational age. Recurrent early pregnancy loss, defined as 2-3 consecutive losses of clinical pregnancies, affects about 1% of all couples.
Risk factors
Independent risk factors for a spontaneous miscarriage include advanced age, extremes of age, feeling stressed, and advanced paternal age. [8, 9, 10] Other risk factors for early pregnancy loss include very low or very high body mass index, Black ethnicity, previous miscarriages, smoking, alcohol use, working night shifts, air pollution, and exposure to pesticides. [17] Symptoms of vaginal bleeding but not abdominal pain are associated with increased risk of miscarriage. One paper suggests that miscarriage can occur in about 50% of patients who present with threatened abortion.
International statistics
No significant difference exists between international rates and the rates in the United States.
Race-, sex-, and age-related demographics
Early pregnancy loss may occur in any race without distinction.
Early pregnancy loss only affects females.
As women mature, the incidence of spontaneous miscarriages increases. Typically, the distribution of miscarriage rates by age occurs as follows: younger than 35 years old, 15% miscarriage rate; 35-39 years old, 20-25% miscarriage rate; 40-42 years old, about 35% miscarriage rate; and older than 42 years old, about 50% miscarriage rate.
Women who conceive using donor eggs have miscarriage rates that are similar to the egg donor's age and not the recipient's age. This information is well documented on the CDC's Assisted Reproductive Technology Web site, and it indicates that miscarriages are increased significantly due to aging oocytes rather than due to the aging uterus.
Prognosis
The prognosis for early pregnancy loss is excellent. After one complete abortion, no increased risk exists for another one. Patients need reassurance. "Tender loving care" with subsequent pregnancies is proven effective therapy in some studies. [18, 19, 20] This approach includes early quantitative hCG levels and ultrasounds weekly, after the hCG threshold is reached, with more frequent visits available if needed for reassurance.
Morbidity/mortality
A complete abortion is unlikely to cause any significant risk of mortality unless significant blood loss or infection occurs. Morbidity would be increased if anemia or infection develops. Patients who are pregnant may bleed quickly and significantly. Distinguishing the causes of bleeding during pregnancy is important.
Incomplete and inevitable abortions are a cause for concern when significant bleeding or infection occurs. If treatment is not performed in a timely manner, significant morbidity and mortality may occur. Retained products of conception may occur after a spontaneous abortion or after a suction D&C.
Patients with retained products usually return for medical care with symptoms of increased bleeding, increased cramping, and/or infection. Caring for these patients quickly with intravenous antibiotics is important, and, after the antibiotics are administered, then a suction D&C is performed. These patients are at risk for developing Asherman syndrome, which consists of adhesions within the uterine cavity. Patients who develop Asherman syndrome may present with amenorrhea or decreased menstrual flow. Asherman syndrome may compromise future fertility. When significant bleeding occurs, fluid management and transfusions may be required while stabilizing the patient prior to a suction D&C.
A complication of D&C is perforation of the uterus, which may be handled by observation. If the patient shows signs of uncontrolled bleeding, then proceeding to a laparoscopy or laparotomy to control the bleeding may be necessary. The choice for laparoscopy or laparotomy depends on the stability of the patient. Occasionally, the perforation is in the area of the uterine vessels or other area where the bleeding is difficult to control and a hysterectomy or uterine artery embolization may be necessary. When bleeding is severe, the patient can easily go into hypovolemic shock or disseminated intravascular coagulopathy (DIC). Both of these situations need prompt attention and treatment.
Surveillance data suggest that spontaneous miscarriages and induced abortions accounted for about 4% of pregnancy-related deaths in the United States. [21]
A prospective survey study by Farren et al that included 186 women reported that of those in the early pregnancy loss group who responded after 1 month, 28% met the criteria for PTSD and 32% for anxiety. Of those in the early pregnancy loss group that responded after 3 months, 38% met criteria for PTSD and 20% for anxiety. [22]
Complications
In a long-term study of more than 1 million women, researchers found an association between pregnancy loss and an increased risk of subsequently developing atherosclerosis, particularly among women younger than 35 years. [23, 24] Women who had miscarriages had a 13% increased risk of subsequent myocardial infarction, a 16% increased risk of cerebrovascular infarction, and a 20% increased risk of renovascular hypertension relative to women who had not had miscarriages. The effect on adverse outcomes appeared to be cumulative, with each additional miscarriage increasing the risk of myocardial infarction (by 9%), cerebral infarction (by 13%), and renovascular hypertension (by 19%). [23, 24]
Complete abortions may be complicated by infection or accumulation of clot in the uterine cavity without expulsion due to uterine atony. Both of these complications are rare.
Occasionally, a decidual cast is passed and is mistaken for products of conception. In these cases, an ectopic pregnancy is likely.
Patient Education
The patient needs to hear that one miscarriage does not put her at increased risk for another miscarriage. Her next pregnancy is likely to last to term if she is young and has no other risk factors.
Advise the patient to return to the emergency department if any of the following symptoms occur:
-
Profuse vaginal bleeding
-
Severe pelvic pain
-
Temperature greater than 100°F
Patients may experience intermittent menstrual-like flow and cramps during the following week. The next menstrual period usually occurs in 4-5 weeks.
Patients may resume regular activities when able, but they should refrain from intercourse and douching for approximately 2 weeks.
For patient education resources, see the Pregnancy Center, as well as Miscarriage, Abortion, Ectopic Pregnancy, and Dilation and Curettage (D&C).
-
Second transvaginal sonogram obtained 1 week after the initial study fails to demonstrate fetal development. This confirms the diagnosis of an embryonic pregnancy.
-
1a Video courtesy; Armando Hernandez
-
1b Video courtesy; Armando Hernandez
-
1c Video courtesy; Armando Hernandez
-
1d Video courtesy; Armando Hernandez
-
1e Video courtesy; Armando Hernandez





