Background
Severe blunt injury to the chest continues to be one of the leading causes of morbidity and mortality in both young and old trauma victims. [1] Flail chest is one of the worst subset of these injuries and is likely the most common serious injury to the thorax seen by clinicians.
See the image below.
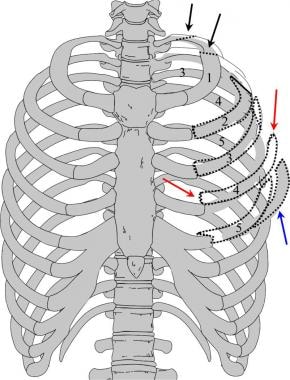 Image depicting multiple fractures of the left upper chest wall. The first rib is often fractured posteriorly (black arrows). If multiple rib fractures occur along the midlateral (red arrows) or anterior chest wall (blue arrows), a flail chest (dotted black lines) may result.
Image depicting multiple fractures of the left upper chest wall. The first rib is often fractured posteriorly (black arrows). If multiple rib fractures occur along the midlateral (red arrows) or anterior chest wall (blue arrows), a flail chest (dotted black lines) may result.
Multiple care patterns and treatment modalities have emerged, many based on anecdotal clinical observation and evidence. Within the last 20 years, more rigorous scientific methods have been applied to the problem of flail chest, in both the clinical setting and laboratory. More advanced radiologic work-up with multislice computed tomography (MSCT) scanners is increasing the frequency of diagnosis of this problem. This article reviews the most salient data of the recent literature and discusses some of the diagnostic and treatment options that are now available in the treatment of flail chest.
History of the Procedure
Flail chest has been observed and reported for many years in the medical and emergency medical science literature. The relatively infrequent occurrence in any one geographic location made large-scale treatment trials difficult, if not impossible. The 1958 Emergency War Surgery NATO Handbook mentions flail chest twice, once as a potential cause of failed resuscitation and once to note field treatment. This field treatment consisted of "firm strapping" of the affected area to prevent the flail-like motion. By 1988, the Emergency War Surgery NATO Handbook (second US revision) mentions flail chest only once, without noting treatment recommendations and broaches the concept that the underlying lung injury—not the flail segment itself—is the major determinant of morbidity.
Older surgical textbooks contain photographs depicting the use of towel clips placed around rib segments and placed on traction to stabilize the rib cage. With the advent of intensive care units (ICUs), older textbooks often advocated orotracheal intubation with positive pressure ventilation to pneumatically stent the ribcage. However, this treatment was subsequently proven to increase morbidity and mortality in patients who did not need intubation for other reasons. Although many patients with flail chest require intubation, advances in the knowledge of physiology and chest wall mechanics, as well as the potential morbidity of prolonged mechanical ventilation, have reestablished that it is the severity of the underlying lung injury and not the flail segment that causes a problem.
Problem
Flail chest is traditionally described as the paradoxical movement of a segment of chest wall caused by fractures of 3 or more ribs anteriorly and posteriorly within each rib. Variations include posterior flail segments, anterior flail segments, and flail including the sternum with ribs on both sides of the thoracic cage fractured.
Flail chest is foremost a clinical finding and observation that is often accompanied by physiologic derangements, which are sometimes globally lumped into the diagnosis. The lumping of signs and symptoms has resulted in confusion regarding both the treatment strategies and the overall importance of the clinical finding.
Mechanically, flail chest generally requires a significant force diffused over a large area (ie, the thorax) to create multiple anterior and posterior rib fractures. If the structural components (ie, the ribs) are weakened for any reason (eg, osteoporosis), then much lower force may be required. The actual motion of the flail segment is usually limited by the surrounding structural components, the intercostals, and the surrounding musculature. This mechanical limitation of motion affects the actual size of the changes in thoracic volume and patient-generated tidal volume. Underlying pulmonary or cardiac disease determines the physiologic perturbations to respiration caused by the flail segment.
Even more important is the amount of injury to the underlying structures, specifically the lungs and heart. Respiratory insufficiency in flail chest is much more likely to be a result of the underlying severity of pulmonary contusion and ventilation perfusion mismatch than the actual structural defect to the chest wall. Thus, the adept surgeon usually looks past the structural deformity and determines the physiologic compromise caused by the pain of the rib fractures, the tidal volume changes, and the underlying pulmonary and cardiac injury.
See the image below.
 Multiple left rib fractures, pulmonary contusion, and hemothorax in an elderly man after a motor vehicle accident.
Multiple left rib fractures, pulmonary contusion, and hemothorax in an elderly man after a motor vehicle accident.
Epidemiology
Frequency
The exact incidence of flail chest is not precisely known. The Major Trauma Outcome Study of more than 80,000 patients documented about 75 patients with flail chest injuries. [2] From 1971 to 1982, Landercasper et al documented 62 consecutive patients. [3] From 1981 to 1987, the Detroit Receiving Hospital noted 57 patients with flail chest. In 1995, Ahmed and Mohyuddin documented 64 cases over a 10-year period. [4] Borman evaluated data from the Israel National Trauma Registry noting 262 fail chest diagnoses of 11,966 chest injuries (118,211 total patients) examined between 1998 and 2003. [5]
The true incidence of flail chest may be even higher than those noted above, based on newer diagnostic modalities and procedures including MSCT scanning of the chest. Based on these articles, an average American College of Surgeons (ACS)-verified level 1 or level 2 trauma center will see about 1-2 cases per month. The incidence of flail chest at nontrauma center facilities is currently unknown. Flail chest in a neonate has been reported as a potential marker of child abuse. [6]
Etiology
Flail chest requires significant blunt force trauma to the torso to fracture the ribs in multiple areas. Such trauma may be caused by motor vehicle accidents, falls, and assaults in younger, healthy patients. Flail chest is an indicator of significant kinetic force to the chest wall and rib cage, but it may also may occur with lesser trauma in persons with underlying pathology, including osteoporosis, total sternectomy, and multiple myeloma, as well as individuals with congenital absence of the sternum.
Pathophysiology
In an adult, a transfer of significant kinetic energy in blunt trauma to the rib cage or a crushing rollover injury is the most frequent cause of flail chest. In children, who have a more compliant chest wall, flail chest is observed with lower frequency than injury to the underlying structures, including the lungs, heart, and mediastinal structures.
Presentation
Flail chest is a clinical anatomic diagnosis noted in blunt trauma patients with paradoxical or reverse motion of a chest wall segment while spontaneously breathing. This clinical finding disappears after intubation with positive pressure ventilation, which occasionally results in a delayed diagnosis of the condition.
The strict definition of 3 ribs broken in 2 or more places can be confirmed only by x-ray, but the inherent structural stability of the chest wall due to the ribs and intercostal muscles usually does not show abnormal or paradoxical motion without 3 or more ribs involved. Patients may demonstrate only the paradoxical chest wall motion, and they may have minimal to incapacitating respiratory insufficiency, although these individuals usually show some tachypnea with a notable decrease in resting tidal volume due to fracture pain. The degree of respiratory insufficiency is typically related to the underlying lung injury, rather than the chest wall abnormality.
Relevant Anatomy
The chest wall is inherently stable, with 12 ribs attaching posteriorly to the spinal column and anteriorly to the sternum. Intercostal muscles with fascial attachments, coupled with other muscle groups, including the trapezius and the serratus groups, add further strength to the bony cage around the thoracic organs. The arch design of the ribs allows for some flexing, more so in children than adults, which can absorb small amounts of blunt kinetic energy. Crush or rollover injuries, especially with heavy objects or significant deceleration injury commonly breaks a rib in 1 position, but only a significant impact breaks a rib in 2 or more positions.
See the image below.
Image depicting multiple fractures of the left upper chest wall. The first rib is often fractured posteriorly (black arrows). If multiple rib fractures occur along the midlateral (red arrows) or anterior chest wall (blue arrows), a flail chest (dotted black lines) may result.
Outcome and Prognosis
Overall, patients with flail chest have a 5-10% reported mortality if they reach the hospital alive. Patients who do not need mechanical ventilation do better statistically, and overall mortality seems to increase with increasing injury severity scores (ISS), age, and number of total rib fractures.
Few long-term follow-up studies regarding flail chest are available. In the absence of concomitant lethal injuries, Freedland et al reported adverse outcomes to be more likely with more severe associated injuries noted by ISS scoring, excessive blood loss and transfusion requirements, bilateral flail chest, and patient age older than 50 years. [7] A report by Albaugh and associates in New Jersey noted flail chest mortality increased 132% with each decade of life, [8] but another report by Athanassiadi and associates found no correlation with age. [9] Both studies noted increasing mortality with increasing ISS. As previously noted, some reports suggest a high rate of disability after flail chest; however, most patients do well and return to normal function after 6-12 months.
Dehghan et al conducted a retrospective analysis of data from the National Trauma Data Bank of injury patterns, management, and clinical outcomes for 3,467 patients in whom flail chest was identified from 2007 to 2009. The mean age of the patients was 52 years; 77.5% were male. Treatment practices included use of epidural catheters (8%); surgical fixation of the chest wall (0.7%); and mechanical ventilation (59%). Complications included pneumonia (21%); adult respiratory distress syndrome (14%); sepsis (7%); and death (16%). More than 99% of patients were treated nonoperatively, and a small proportion (8%) received aggressive pain management with epidural catheters. The authors concluded that alternative methods of treatment, including more consistent use of epidural catheters for pain and surgical fixation, should be investigated. [10]
A study by Daskal et al included 407 patients with blunt trauma who had at least three rib fractures and were hospitalized at a level 2 trauma center. Both pneumothorax and hemothorax were more common among the 79 patients in the study with flail chest. [11]
Complications
Reports in the medical literature note a high level of long-term disability in patients sustaining flail chest. Beal and Oreskovich reported a 22% disability rate with over 63% having long-term problems, including persistent chest wall pain, deformity, and dyspnea on exertion. [12] Kishikawa et al, however, noted resolution of altered pulmonary function within 6 months, even with chest wall deformity still present. [13]
-
Image depicting multiple fractures of the left upper chest wall. The first rib is often fractured posteriorly (black arrows). If multiple rib fractures occur along the midlateral (red arrows) or anterior chest wall (blue arrows), a flail chest (dotted black lines) may result.
-
Multiple left rib fractures, pulmonary contusion, and hemothorax in an elderly man after a motor vehicle accident.
-
Axial computed tomography image of the chest in a patient with left posterior rib fractures. The left pneumothorax (white arrows) is associated with a displaced posterior left rib fracture (black arrow). Secondary effects on the left lung include a pulmonary contusion and volume loss.









