Practice Essentials
Status asthmaticus is considered a medical emergency. It is the extreme form of an asthma exacerbation that can result in hypoxemia, hypercarbia, and secondary respiratory failure. In practice, the role of the physician is to prevent this from happening through patient compliance with controller medications (eg, steroid inhalers) in an outpatient setting.
Patient education plays a very major role in preventing recurrent attacks of status asthmaticus. In a study by Rice et al, [1] inpatient asthma education was studied in children and adolescents following status asthmaticus. Subjects were enrolled in two groups. One group received the usual posthospitalization instructions and the other group received additional education by lay asthma education volunteers. The group that received the additional education had better compliance in the outpatient setting.
Background
Status asthmaticus is an acute exacerbation of asthma that remains unresponsive to initial treatment with bronchodilators. Status asthmaticus can vary from a mild form to a severe form with bronchospasm, airway inflammation, and mucus plugging that can cause difficulty breathing, carbon dioxide retention, hypoxemia, and respiratory failure. (See Prognosis and Presentation.)
Patients report chest tightness, rapidly progressive shortness of breath, dry cough, and wheezing and may have increased their beta-agonist intake (either inhaled or nebulized) to as often as every few minutes. (See Presentation.)
Typically, patients present a few days after the onset of a viral respiratory illness, following exposure to a potent allergen or irritant, or after exercise in a cold environment. Frequently, patients have underused or have been underprescribed anti-inflammatory therapy. Illicit drug use may play a role in poor adherence to anti-inflammatory therapy. (See Etiology and Presentation.)
A study published in 2004 [2] noted the number of patients with status asthmaticus requiring intensive care admissions had declined over 10 years. The trend was toward less advanced presentations. This may reflect improvements in medication compliance, education, or access to medical care. Nonetheless, concern has been raised more recently about an increase that has since been observed in the severity of asthma symptoms and the need for more intensive care management. [3] (See Prognosis, Workup, Treatment, and Medication.)
See Pediatric Status Asthmaticus for information about status asthmaticus in children.
Treatment goals
Management goals for status asthmaticus are (1) to reverse airway obstruction rapidly through the aggressive use of beta2-agonist agents and early use of corticosteroids, (2) to correct hypoxemia by monitoring and administering supplemental oxygen, and (3) to prevent or treat complications such as pneumothorax and respiratory arrest. (See Treatment and Medication.
Etiology
Exposure to an allergen or trigger causes a characteristic form of airway inflammation in susceptible individuals, exemplified by mast cell degranulation, release of inflammatory mediators, infiltration by eosinophils, and activated T lymphocytes. Multiple inflammatory mediators may be involved, including interleukin (IL)–3, IL-4, IL-5, IL-6, IL-8, IL-10, and IL-13, leukotrienes, and granulocyte-macrophage colony-stimulating factors (GM-CSFs). These, in turn, incite involvement of mast cells, neutrophils, and eosinophils. (See the diagram below.)
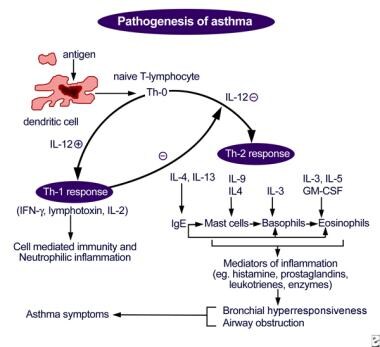 Figure depicting antigen presentation by the dendritic cell, with the lymphocyte and cytokine response leading to airway inflammation and asthma symptoms.
Figure depicting antigen presentation by the dendritic cell, with the lymphocyte and cytokine response leading to airway inflammation and asthma symptoms.
Physiologically, acute asthma has two components: an early, acute bronchospastic aspect marked by smooth muscle bronchoconstriction and a later inflammatory component resulting in airway swelling and edema.
Early bronchospastic response
Within minutes of exposure to an allergen, mast cell degranulation is observed along with the release of inflammatory mediators, including histamine, prostaglandin D2, and leukotriene C4. These substances cause airway smooth muscle contraction, increased capillary permeability, mucus secretion, and activation of neuronal reflexes. The early asthmatic response is characterized by bronchoconstriction that is generally responsive to bronchodilators, such as beta2-agonist agents.
Later inflammatory response
The release of inflammatory mediators primes adhesion molecules in the airway epithelium and capillary endothelium, which then allows inflammatory cells, such as eosinophils, neutrophils, and basophils, to attach to the epithelium and endothelium and subsequently migrate into the tissues of the airway. Eosinophils release eosinophilic cationic protein (ECP) and major basic protein (MBP). Both ECP and MBP induce desquamation of the airway epithelium and expose nerve endings. This interaction promotes further airway hyperresponsiveness in asthma. This inflammatory component may even occur in individuals with mild asthma exacerbation.
Bronchospasm, mucus plugging, and edema in the peripheral airways result in increased airway resistance and obstruction. Air trapping results in lung hyperinflation, ventilation/perfusion (V/Q) mismatch, and increased dead space ventilation. The lung becomes inflated near the end-inspiratory end of the pulmonary compliance curve, with decreased compliance and increased work of breathing.
The increased pleural and intra-alveolar pressures that result from obstruction and hyperinflation, together with the mechanical forces of the distended alveoli, eventually lead to a decrease in alveolar perfusion. The combination of atelectasis and decreased perfusion leads to V/Q mismatch within lung units. The V/Q mismatch and resultant hypoxemia trigger an increase in minute ventilation.
Complications
In the early stages of acute asthma, hyperventilation may result in respiratory alkalosis. This is because obstructed lung units (slow compartment) are relatively less numerous than unobstructed lung units (fast compartment). Hyperventilation allows carbon dioxide removal via the fast compartment. However, as the disease progresses and more lung units become obstructed, an increase in the slow compartments occurs, resulting in decreased ability for carbon dioxide removal and eventually causing hypercarbia.
Risk factors
Asthma results from a number of factors, including genetic predisposition and environmental factors. Patients often have a history of atopy. The severity of asthma has been correlated with the number of positive skin test results.
Gastroesophageal reflux disease is another risk factor for asthma, with studies indicating that the reflux of gastric contents with or without aspiration can trigger asthma in susceptible children and adults. Animal studies have shown that the instillation of even minute amounts of acid into the distal esophagus can result in marked increases in intrathoracic pressure and airway resistance. This response is thought to be due to vagal and sympathetic neural responses.
Risk factors for asthma also include the following:
-
Viral infections
-
Air pollutants - Such as dust, cigarette smoke, and industrial pollutants
-
Medications - Including beta-blockers, aspirin, and nonsteroidal anti-inflammatory drugs (NSAIDs)
-
Cold temperature
-
Exercise
Epidemiology
Occurrence in the United States
Asthma affects up to 10% of the US population. Prevalence has increased by 60% in all ages in the past two decades. A significant rise in hospitalization and asthma mortality rates has accompanied the increased incidence.
Status asthmaticus is usually more common among persons in low socioeconomic groups, regardless of race, as they have less access to regular specialist medical care. [4] People who live alone are particularly affected.
International occurrence
The worldwide incidence of asthma is unclear but is estimated to be about 20 million cases. The dramatic rise in incidence has been attributed, in part, to pollution and industrialization.
Demographics
In the United States, asthma prevalence is higher among children, women, blacks, and persons with reported income below the federal poverty level. [5]
Prognosis
In general, unless a complicating illness such as congestive heart failure or chronic obstructive pulmonary disease is present, status asthmaticus has a good prognosis if appropriate therapy is administered. A delay in initiating treatment is probably the worst prognostic factor. Delays can result from poor access to health care on the part of the patient or even delays in using corticosteroids. Patients with acute asthma should use corticosteroids early and aggressively.
Complications
Complications of asthma can include the following:
-
Cardiac arrest
-
Respiratory failure or arrest
-
Hypoxemia with hypoxic ischemic central nervous system (CNS) injury
-
Pneumothorax or pneumomediastinum
-
Toxicity from medications
Pneumothorax may complicate acute asthma because of increased airway pressure or as a result of mechanical ventilation. Superimposed infection can also occur in intubated patients. Patients may require a chest tube for pneumothorax or aggressive antibiotic therapy for a superimposed infection.
Mortality
The mortality rate from asthma has increased at an alarming rate. From 1993-1995, the overall annual age-adjusted death rate for asthma increased 40%. The rise in the mortality rate has been even higher among blacks, among people living in poverty, and among children aged 4 years or younger and those aged 9-16 years. More recently, asthma mortality rates are trending lower. [6]
The mortality risk is also particularly high in patients who delay medical treatment, especially treatment with systemic corticosteroids. Patients with other preexisting conditions (eg, restrictive lung disease, congestive heart failure, chest deformities) are at particular risk of death from status asthmaticus. Patients who smoke regularly have chronic inflammation of the small airways and are also at greater risk of death from status asthmaticus. Data also suggest higher mortality in persons of lower socioeconomic status, with psychiatric illness, with recent poorly controlled asthma, or with a history of prior intubation. One study links exposure to the common mold Alternaria alternata and mortality in asthma. [7]
Patient Education
Asthma is a chronic illness. Patients and their families must be provided with a team that can offer education and follow-up care. Prior to discharge, the team that provides asthma education should meet with the family and the patient to impart information regarding maintenance, monitoring, and measures for environmental control. Early identification of exacerbations and the importance of adherence with therapy are paramount.
Studies have also demonstrated the importance of an asthma education plan. Guidelines regarding this literature have been published. [8]
Patients require instruction in the appropriate use of inhalers, to be compliant with therapy, and to practice stress-avoidance measures. Stress factors (ie, triggers of asthma attacks) include pet dander, house dust, and mold. Strongly discourage patients from smoking, this habit should be avoided at all costs.
For patient education information, see the Asthma Center, as well as Asthma, Asthma FAQ, and Understanding Asthma Medications.
-
Figure depicting antigen presentation by the dendritic cell, with the lymphocyte and cytokine response leading to airway inflammation and asthma symptoms.






