Practice Essentials
Success in laser hair removal is typically reported in terms of permanent hair elimination or in terms of marked delay in its growth. [1, 2] Most investigators have assessed patients with light skin types (ie, Fitzpatrick skin types I-III), but more recent groups have studied newer lasers for Fitzpatrick skin types IV-VI.
See the image below.
Workup
Skin patch testing is the most important step in laser hair removal, with the results determining the settings for the laser and the safety profile. Perform testing in a low-visibility area with the same skin type as the area intended for treatment. If possible, allow at least 3 days before reexamining the site to assess for efficacy and for a reaction.
Procedure
Patients are instructed not to pluck hairs for several weeks prior to treatment and not to sunbathe for several weeks or even months before the procedure. The area to be treated is shaved before anesthetic cream is applied. The cream is later removed, and the area is marked and photographed. When treatment begins, the laser is applied to the target area at the fluence level predetermined by patch testing.
History of the Procedure
Goldman et al first described ruby-laser injury to pigmented hair follicles in 1963. [3] In 1983, Oshiro and Maruyama noted hair loss from nevi after treatment with a ruby laser. [4] However, at fluences affecting hair follicles, the epidermis was severely damaged.
The theory of selective photothermolysis that Anderson and Parrish developed in 1983 was based on a laser of particular wavelength and a pulse duration of light to target a particular chromophore. [5] By applying this theory, the target can be destroyed selectively, sparing the surrounding tissue.
Use of a topical suspension of carbon particles followed by treatment with a Q-switched neodymium-doped yttrium aluminum garnet (Nd:YAG) laser was the first laser treatment for hair removal the US Food and Drug Administration (FDA) approved. This initial method reportedly delayed regrowth by 3 months, but it did not provide permanent hair reduction.
In 1996, Grossman and associates, who used a normal-mode ruby laser, reported the first application of Anderson and Parrish's theory for hair removal. [6] In 1998, Dierickx and associates published their report of a 2-year follow-up study demonstrating long-term, permanent hair removal with this laser. [7]
Hair-removing lasers and light sources
Since then, the market has been flooded with numerous hair-removing lasers and light sources. [8]
Initial laser systems, such as the Q-switched Nd:YAG (1064 nm, Soft Light system; Thermolase Corp, San Diego, CA), used a suspension of carbon mineral oil to penetrate the hair follicle and to act as an energy-absorbing chromophore.
An optically filtered xenon flashlamp (Epi Light, ESC Luxar; Energy Systems Corp, Needham, MA) uses filters to select operating wavelengths of light at a cutoff of 690 nm, allowing light above this wavelength to pass through to affect hair.
The long-pulse ruby laser (EpiLaser 694 nm, Palomar Technologies, Lexington, MA; EpiTouch, Sharplan Laser, Allendale, NJ) uses the principle of selective thermolysis in which melanin acts as the target chromophore.
The long-pulse alexandrite laser (PhotoGenica LPIR 755 nm; Cynosure Inc, Chelmsford, MA) is based on the principle of thermokinetic selectivity and targets melanin in the hair follicle. In this way, the epidermis is allowed to cool efficiently while the melanin in the hair follicle is heated. [9, 10]
Coherent Medical (Santa Clara, CA) and Palomar (Lexington, MA) have introduced the LightSheer, a diode laser operating at 800 nm that has pulse durations of as long as 30 ms. This technology minimizes the size of the laser by replacing the laser tube in place of solid-state diode circuitry. [11]
Most technical improvements in laser devices have been incremental in terms of improving efficacy and reducing side effects. Some new models combine light- and heat-based methods by using radio-frequency (RF) energy; these are based on the theory that the heated areas can be further heated without causing damage to surrounding skin.
New devices are frequently introduced, and old models may be discontinued but still available as after-market products. Check with the manufacturers for latest information.
Home-use lasers and IPL devices
Several low-power devices have been marketed directly to consumers as home-use epilators. Originally, most were not capable of even epilation. More recently, the FDA has approved some devices for in-home use. Physicians should ascertain whether patients presenting with adverse effects were using one of these devices instead of medical-grade lasers. [12, 13]
Problem
Unwanted pigmented hair is a common cosmetic problem for both men and women.
Epidemiology
Frequency
About 4% of young, healthy randomly selected White women feel disfigured by their facial hair. The percentage is even higher in people of color and increases with age. This percentage does not reflect the vast number of patients who have unwanted hair in other areas, and it does not account for the huge number of men who feel disfigured by unwanted hair (eg, on the ears and back).
Etiology
Excessive hair growth affects the healthy population, but it also severely affects patients with hormonal disturbances, such as polycystic ovary disease, congenital adrenal hyperplasia, hirsutism, hypertrichosis, and congenital hairy nevi.
Excessive hair growth has been implicated in the pathogenesis of pilonidal disease and in the unfavorable outcome of some reconstructive flaps.
Pathophysiology
Hirsutism is characterized by the excessive growth of coarse terminal hairs in women in a pattern similar to that of adult men. Given the subjectiveness of this perception, especially in different racial groups, Ferriman and Galway developed a scoring scale. Nine body areas are used to grade hair growth on a scale of 0-4. The scores for the 9 body parts are added, and a total score of 8 or more defines hirsutism. On the basis of this scale, 5% of women in the United States have hirsutism.
Hyperandrogenism (ie, increased plasma androgen levels) is sometimes the cause. This condition may be related to adrenal causes (eg, congenital adrenal hyperplasia, androgen-producing tumors), pituitary causes (eg, Cushing disease), ovarian causes (eg, polycystic ovary disease, ovarian tumors), or exogenous causes (eg, anabolic steroids, testosterone).
Idiopathic hirsutism is likely caused by subtle forms of ovarian or adrenal hypersecretion, alterations in serum androgen-binding proteins or androgen metabolism, or (most likely) excessive genetic sensitivity of hair follicles to normal androgen levels.
Presentation
Patients typically have a history of either excessive hair growth or hair growth in undesired body locations. For men, these areas are often the shoulders, back, and ears. For women, these areas are often the face, breasts, legs, and lower abdomen.
Take a complete history, including menstrual, pregnancy, and family histories. Discuss the degree of past, recent, and potential future sun exposure.
Perform a full external physical examination. If a hormonal problem is suspected, consider referring the patient to an endocrinologist or a gynecologist.
Indications
The indication for hair removal is mostly subjective. A desire for hair removal is the only criterion for laser surgery.
Relevant Anatomy
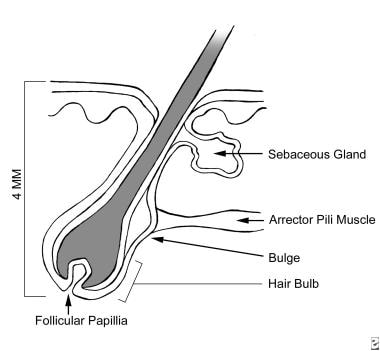
Each hair has 3 distinct components: the bulb, which lies near the insertion of the erector pili, the isthmus, and the infundibulum.
Pluripotential cells in the bulb and bulge areas cause growth of the hair follicle. Melanocytes are present in these areas. For most people, the bulb is approximately 4 mm beneath the surface of the skin (deeper in some individuals). Therefore, a considerable laser-penetration depth is required to remove the bulb.
Hair grows in cycles. Anagen is the active growth phase, catagen is the transition phase, and telogen is the resting phase. The duration of the anagen phase governs the length of hair at different body sites. Lasers are truly effective in only the anagen phase, when hair-matrix cells divide rapidly and migrate outward from the shaft and when the melanin load is at its highest. During the catagen phase, mitosis ceases, the hair matrix regresses, the papilla retracts to a place near the bulge, and capillary nourishment diminishes. In the telogen phase, the follicle detaches from the papillae and contracts to a third of its original depth, eventually falling out. The telogen phase varies in duration from one body area to the next. For example, the telogen phase may last as long as a year for hair on the leg.
The ratio of anagen follicles to telogen follicles varies with body location. Because not all of the hairs are in the anagen phase at any 1 time, laser treatment must be repeated to capture the new hairs coming into the anagen phase.
Contraindications
For the laser to be effective, the hair pigment must be darker than the surrounding skin pigment. If this is not the case, the treatment will not work, and harmful complications may occur. Early in the evolution of the procedure, patients with Fitzpatrick skin types V or VI were not candidates, and even patients with skin types III and IV were at high risk. With new technologies, most patients can now be treated, though caution must still be exercised.
Recently, Aldraibi et al looked at using topical corticosteroid treatment to help minimize the side effects when treating skin types IV-VI with an Alexandrite laser system. [14] Their study showed that using a topical corticosteroid treatment appears to minimally help in reducing posttreatment erythema and edema and also decreases the duration of hyperpigmentation. It was felt in this study that treating skin type VI was "less safe."
A literature review by Fayne et al suggested that Fitzpatrick skin types IV-VI can undergo safe and effective laser hair reduction using longer wavelengths and employing Nd:YAG, diode, alexandrite, or ruby lasers. Some intense pulsed light sources were also found to be useful. [15]
Sun tanning is obviously contraindicated during or before treatment because the practice darkens the pigment of the skin surrounding the hair.
-
Pain-sensitivity diagram.
-
Anatomy of the hair follicle.
-
Absorption spectrum of melanin and oxyhemoglobin.
Tables
Anesthetic |
Active Ingredient |
Advantages |
Disadvantages |
Ametop gel |
Tetracaine 4% |
|
|
Betacaine cream |
Lidocaine, prilocaine |
|
|
ELA-Max or ELA-Max 5 cream |
Lidocaine 4% or 5%, respectively |
|
|
EMLA cream |
Lidocaine 2.5%, prilocaine 2.5% |
|
|
Mento-kaine liquid |
Benzocaine 20%, phenol, camphor, menthol |
|
|
Stud spray |
Lidocaine 9.6% |
|
|
Location |
Resting Hairs, % |
Growth Time |
||
Telogen |
Anagen |
Telogen |
Anagen |
|
Head |
||||
Scalp |
13 |
85 |
3-4 mo |
2-6 y |
Eyebrows |
90 |
10 |
3 mo |
4-8 wk |
Ear |
85 |
15 |
3 mo |
4-8 wk |
Cheeks |
30-50 |
50-70 |
NA |
NA |
Beard or chin |
30 |
70 |
10wk |
1 y |
Mustache or upper lip |
35 |
65 |
6 wk |
16 wk |
Body |
||||
Axillae |
70 |
30 |
3 mo |
4 mo |
Trunk |
NA |
NA |
NA |
NA |
Pubic area |
70 |
30 |
3 mo |
4 mo |
Arms |
80 |
20 |
18 wk |
13 wk |
Thighs |
80 |
20 |
24 wk |
16 wk |
Breasts |
70 |
30 |
NA |
NA |
NA = not applicable. *Adapted from Cutis. Mar 1990;45(3):199-202 [17] |
||||
Adverse event |
Long-Pulsed 694 nm Ruby |
Long-Pulsed 755 nm Alexandrite |
Long-Pulsed 800 nm Diode |
Long-Pulsed 810 nm Diode |
Long-Pulsed 1064 Nd:YAG |
IPL |
IPL/ Heat Energy |
Erythema |
... |
90% |
69% |
52% |
23% |
92% |
54% |
Burning |
... |
61% |
30% |
44% |
14% |
... |
4% |
Blistering/crusting |
8% |
... |
... |
5% |
... |
4%-12% |
... |
Hypopigmentation |
4% |
8% |
5% |
11%-25% |
... |
12% |
8% |
Hyperpigmentation |
16% |
40% |
31% |
9%-38% |
2% |
12% |
8% |
Other scarring |
... |
15% |
6% |
... |
2% |
... |
... |
* Adapted from J Drugs Dermatol. Jan 2007;6(1):40-6 [19] Laser hair removal has not been available long enough to permit a full assessment of its long-term health effects. At this time, short-term data indicate that laser hair removal is generally safe. Because studies have shown that laser hair removal can alter skin structures such as sweat and oil glands, they may cause lasting changes to the skin as adverse effects in some patients. |
|||||||





