History Of The Procedure
In 1898, the temporoparietal fascia flap was described nearly simultaneously for reconstruction of the external ear (after a horse bite) and for reconstruction of the lower eyelid. [1, 2, 3] Despite these descriptions of its use in head and neck reconstruction, the flap remained an obscure and underused tool until an explosion of new descriptions of its use (as either a pedicled or a microvascular free tissue transfer) resurrected it in recent times. [4, 5]
In 1983, Brent et al reported the successful use of the flap as an axial-pattern fascial flap, a random-pattern fascial flap, and a free fascial flap for secondary ear reconstruction. [6] In 1993, Cheney et al described 21 cases using the flap for a variety of reconstructions in the head and neck. [7] Today, the temporoparietal flaps remain the only single-layered fascia flap that can be used as a pedicled vascular flap in the head and neck. The flap is thin and pliable, and it readily accepts a skin graft. Temporoparietal flaps can drape into concavities and over convexities, such as those present in the external ear, and they are highly vascular and resistant to infection. This reliability and versatility, particularly in the setting of trauma and devascularized tissue beds, make it a flap limited only by the surgeon's imagination.
See the image below.
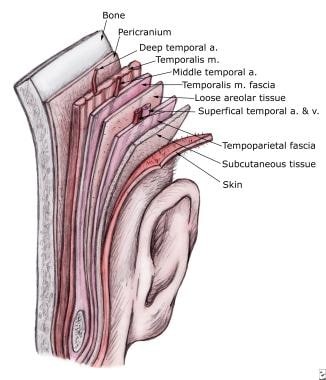 Temporoparietal fascia flap. A more accurate description of the layers of the scalp, demonstrating the relationship of the temporoparietal fascia to the overlying skin and subcutaneous tissue and the deeper muscular fascia.
Temporoparietal fascia flap. A more accurate description of the layers of the scalp, demonstrating the relationship of the temporoparietal fascia to the overlying skin and subcutaneous tissue and the deeper muscular fascia.
Indications
Temporoparietal fascial flaps have been described for vascularized soft tissue coverage in a remarkable variety of head and neck defects as follows:
-
Pedicled fascial flap for auricular reconstruction (primary and secondary)
-
Pedicle for vascularized calvarial bone grafts
-
Composite skin and cartilage graft from helical root for alar reconstruction
-
Composite fascia and hair-bearing skin for scalp and lip reconstruction, soft tissue filler in temporal and parotid defects
-
Microvascular free tissue graft - Microvascular anastomosis use with or without a vein interposition graft to obviate the limitation of the pedicle
-
Coverage of large scalp defects
-
Coverage of contralateral temporal defects
-
Double-layered fascial graft - Another description of the temporoparietal flap when it is harvested with temporalis muscular fascia supplied by the middle temporal artery (This flap can accept cartilage and bone grafts placed in the envelope between the 2 layers of fascia.)
-
Nasal reconstruction
-
Oral reconstruction
In a study of 11 patients who underwent parotidectomy, Movassaghi et al reported that the resulting defect can be successfully filled with a temporoparietal fascia flap to prevent cheek contour deformity, with the tissue barrier possibly also helping to prevent Frey syndrome. [8]
A retrospective study by Pellini et al found that in patients who undergo salvage total laryngectomy, prevention of postoperative pharyngocutaneous fistulas through reinforcement of the pharyngeal suture with a temporoparietal fascia flap is comparable to that achieved when a pectoralis major myocutaneous flap is used. The investigators did find increased surgical time when the temporoparietal fascia flap was employed, but evidence indicates better functional outcomes with this flap in selected patients. [9]
Relevant Anatomy
The relevant anatomy of the scalp is emphasized to every medical student with the following mnemonic:
-
S - Skin
-
C - Subcutaneous tissue
-
A - Aponeurosis and occipitofrontalis muscle
-
L - Loose subaponeurotic tissue
-
P - Pericranium
In the temporoparietal region, this mnemonic is an oversimplification. The literature surrounding this anatomy contains a jumbling of nomenclature describing the various layers of temporal fascia, which can further frustrate surgeons trying to master this flap.
To be accurate, the scalp in the temporoparietal area consists of more than 5 separate layers, and significant creativity would be required to massage the mnemonic SCALP from them (see the image below).
Temporoparietal fascia flap. A more accurate description of the layers of the scalp, demonstrating the relationship of the temporoparietal fascia to the overlying skin and subcutaneous tissue and the deeper muscular fascia.
The first layer consists of the skin and subcutaneous tissue. Immediately deep and firmly bound to this layer is the temporoparietal (sometimes called superficial temporal) fascia. This layer is contiguous with the superficial musculoaponeurotic system (SMAS) as it passes over the zygomatic arch into the mid face, and it is contiguous with the galea aponeurotica above the superior temporal line.
Beneath the temporoparietal fascia lies a loose areolar and avascular tissue layer that separates the fascia from the temporalis muscular fascia (sometimes termed the deep temporal fascia). This areolar layer allows the superficial scalp to move freely over the deeper and more fixed temporalis muscular fascia, temporalis muscle, and pericranium.
Confusing the issue further is the division of the temporalis muscular fascia as it splits into a superficial and deep layer (of the deep temporal fascia) surrounding a fatty tissue pad at the temporal line of fusion, approximately 2 cm above the zygomatic arch. The temporalis muscular fascia is contiguous with the pericranium above the superior temporal line and is contiguous with the masseter muscle fascia below the arch.
The superficial temporal artery supplies the temporoparietal fascia flap. The artery emerges from the parotid tissue, gives off the middle temporal artery, and traverses a tortuous course in the preauricular area. Approximately 3 cm above the zygomatic arch, it divides into the terminal frontal and parietal branches. The superficial temporal vein generally runs superficial to and with the artery, but variability, including branching or a posterior course, may be encountered.
The auriculotemporal nerve, a sensory branch of the mandibular nerve, lies posterior to the superficial temporal artery within the temporoparietal fascia. The frontal branch of the facial nerve traverses an oblique course over the zygomatic arch, which can be estimated by a line connecting a point 0.5 cm inferior to the tragus to a point 1.5 cm lateral to the superior brow. This nerve also lies within the temporoparietal fascia, and flap elevation anterior to the frontal branch of the superficial temporal artery should proceed with caution to avoid injuring this nerve.
Contraindications
Although the temporoparietal fascia flap is highly vascular and reliable, prior injury to the temporal field could result in flap necrosis. Radiation therapy, trauma, or previous surgery around the superficial temporal arteriovenous supply may increase the risk of flap necrosis and should be considered relative contraindications. Preoperative Doppler assessment of the superficial temporal artery and its branches can confirm vascular flow to the flap. Significantly, in a 1985 report, Brent has described successful elevation and skin grafting of a random temporoparietal flap in a secondary microtia reconstruction when no axial vessels could be identified by Doppler assessment or surgical dissection. [10]
Prior trauma to the area may also increase the risk of postoperative alopecia, which is always a risk anytime this flap is harvested.
-
Temporoparietal fascia flap. A more accurate description of the layers of the scalp, demonstrating the relationship of the temporoparietal fascia to the overlying skin and subcutaneous tissue and the deeper muscular fascia.
-
Temporoparietal fascia flap. The important topography to mark on the scalp prior to incision includes the proximal trunk of the superficial temporal artery, the frontal and parietal arterial branches, the temporal line, and the approximate course of the frontal branch of the facial nerve.
-
Temporoparietal fascia flap. After elevating the flaps, the superior, posterior, and anterior borders of the temporoparietal flap are incised.
-
Temporoparietal fascia flap. After careful elevation of the flap with protection of the superficial temporal artery pedicle, the flap is draped into the recipient bed. The pliability of the flap make it uniquely suited for draping over cartilage and bone.








