History of the Procedure
Distraction osteogenesis (DO), a well-established technique used for several decades by orthopedic surgeons to repair long bone defects, has, over the past 15 years, gained acceptance for correction of various craniofacial deformities. Bone distraction is not a new concept. Distraction was introduced first by Codvilla nearly a hundred years ago and was subsequently popularized during the 1940s by Ilizarov, who developed a single-stage procedure to lengthen long bones without the use of grafting material. [1] The feasibility of applying Ilizarov's principles to different craniofacial deformities was not considered until several decades after his pioneering work in the peripheral skeleton.
In the purest sense, the first reports of craniofacial DO were in the early 1960s, when rapid expansion of the palate was carried out in growing patients. This practice, however, involved distraction of a naturally occurring physis. Finally, in 1973, Snyder first described the Ilizarov technique to lengthen a surgical osteotomy of the canine mandible. Interest in craniofacial distraction at first grew slowly, with sporadic experimental reports appearing over the ensuing 2 decades. However, in the early 1990s, experimental investigation intensified following reports from New York University on lengthening of dog mandibles and from Constantino and Friedman et al, who used DO to successfully close canine segmental lower jaw defects. [2]
Thereafter, several studies (within various animal models) demonstrated the application of osteodistraction at a number of different sites, including the mandible, lower maxilla, midface, and cranial vault. [3] In 1992, the first clinical results of craniofacial DO were reported by McCarthy et al in a small series of patients with congenital mandible deformities. [4] Since then, several larger series with longer follow-up periods have appeared. More recently, the technique has been successfully used for midfacial and upper craniofacial skeletal defects. [5]
See the images below.
Problem
The underlying principle of DO, as described by Ilizarov, is "the mechanical induction of new bone between bony surfaces that are gradually distracted." The process of DO begins with careful preoperative assessment and planning, which are critical to success. At the initial surgery, osteotomies are performed and the distraction device is inserted. A waiting period (latency phase) is allowed to elapse during which bone healing is initiated at the bony gap. In this early period, periosteal integrity is restored and callus formation begins. The bone segments at either end of the gap are then progressively distracted over a period of several days (distraction phase) during which osteogenesis is induced, thus producing a so-called regenerate of immature bone laid down between the cut bone ends. Over time, the bone remodels into a more mature state (consolidation phase), and the surrounding soft tissues adapt to their new positions and lengths.
Pathophysiology
The histology and physiologic principles underlying DO have been well documented in long bones and, more recently, in the craniofacial skeleton. During the distraction phase, bone formation occurs in response to tension-stress forces exerted on the regenerate, and healing proceeds primarily by a regenerative membranous ossification process. The middle of the regenerate consists of a fibrous central zone where osteoid is deposited with collagen fibers oriented parallel to the direction of distraction.
Ossification occurs as a primary mineralization front advances from either end of the fibrous central zone, resulting in a bridge of immature bone across the distraction gap. Bone remodeling begins during the consolidation phase and continues over 1-2 years, eventually transforming the regenerate into a mature osseous structure similar in size and shape to the adjacent bone. Although the volume of new bone is comparable to that of adjacent bones, animal studies show that mineral content and radiodensity is approximately 30% less, as is the tensile strength of the regenerated segment.
In addition to bony changes, effects on the adjacent soft tissue occur in response to osseous distraction. Muscle and soft tissue mass increase via a process referred to as distraction histogenesis. Clinically, this offers a distinct advantage because several craniofacial anomalies have soft tissue hypoplasia in addition to deficient bony structures. Neurovascular elements contained within distracted bony segments are also stimulated to regenerate. Experimental studies in dogs demonstrate regeneration of the mandibular canal containing both neural and vascular elements. However, the functional level of the regenerated neurovascular structures is less than normal. [6]
A number of factors are known to influence the physiologic process of DO, and these can be separated into 2 basic groups: bone factors and distraction factors.
Bone factors
Osteocyte viability is essential to provide an adequate source of osteoblastic activity at the distraction site; hence, exercise careful surgical technique to minimize thermal or mechanical bone injury. Similarly, an adequate blood supply to the distraction site is critical to osteogenesis. Arterial insufficiency may lead to ischemic fibrogenesis within the regenerate, yielding a loose irregular collagen network instead of the desirable dense regular collagen pattern. Venous outflow obstruction has been associated with cystic degeneration of the regenerate.
The clinician, therefore, must ensure that soft tissues surrounding the site of proposed distraction are well vascularized. Early studies in long bones concluded that both an intact periosteum and endosteum were critical to successful osteogenesis; therefore, many advocated that a corticotomy be performed only through a minimal periosteal opening. More recently, however, investigators have demonstrated that the periosteum alone can provide sufficient osteogenic capacity for a healthy regenerate, and this is especially true in the well-vascularized membranous bone of the craniofacial skeleton.
Therefore, while some clinicians advocate a corticotomy, most reports of craniofacial DO describe the use of a complete osteotomy (taking care to preserve as much of the surrounding periosteum as possible). Prior radiation therapy to the distraction site does not adversely influence the results of distraction (in the canine model), and when using DO to repair segmental defects, the status of the surrounding soft tissues probably is the key factor influencing outcome.
Distraction factors
The latency, rate, and rhythm of distraction are all known to influence the quality of the regenerate. Of these factors, the effect of latency is the most controversial. Most craniofacial surgeons have empirically applied the conclusions from long bone studies and recommend waiting 4-7 days following osteotomy before initiating the distraction process. In younger children, the high rate of bone metabolism would favor a shorter waiting period. [7, 8] Some clinicians, however, use a zero latency period and begin distracting upon appliance insertion, claiming no adverse effects on outcome, while substantially shortening the treatment period.
Waiting too long prior to distraction (ie, >10-14 d) substantially increases the risk of premature bone union. In contrast to latency, the rate and frequency (ie, rhythm) of distraction are considered important variables. If widening of the osteotomy site occurs too rapidly (ie, > 2 mm/d), then a fibrous nonunion results, whereas if the rate is too slow (ie, < 0.5 mm/d), then premature bony union prevents lengthening to the desired length. These findings in long bones have been empirically applied to the craniofacial skeleton, and most studies have described a rate of 1.0 mm/d.
According to Ilizarov's work in long bones, the ideal rhythm is a continuous form of distraction; however, this is impractical on a clinical basis. [1] Therefore, most reports have used distraction frequencies of 1-2 times daily. The length of the consolidation phase has been recommended to range from 6-12 weeks in long bones, depending on the length of the distraction segment. In the craniofacial skeleton, most authors advocate a range of 4-8 weeks. The general rule holds that the consolidation period should be at least twice the duration of the distraction phase.
Finally, appliance rigidity during distraction and consolidation is a critical element to ensure that bending or shearing forces do not result in microfractures of the immature columns of new bone within the regenerate, which lead to focal hemorrhage and cartilage interposition.
Indications
Craniofacial DO is well accepted for several underlying disorders. Distraction osteogenesis (DO) has also been described for several less common etiologies, albeit on a more sporadic basis. Current usage falls into 3 broad groups as follows:
Lower face (mandible)
See the list below:
-
Most common application to date
-
Unilateral distraction of the ramus, angle, or posterior body for hemifacial microsomia
-
Bilateral advancement of the body for severe micrognathia, particularly in infants and children with airway obstruction as observed in the Pierre Robin syndrome
-
Vertical distraction of alveolar segments to correct an uneven occlusal plane or to facilitate implantation into edentulous zones
-
Horizontal distraction across the midline to correct crossbite deformities or to improve arch form
Midface (maxilla, orbits)
See the list below:
-
Advance the lower maxilla at the Le Fort I level
-
Complete midfacial advancement at the Le Fort III level [9]
-
Closure of alveolar bony gaps associated with cleft lip and palate deformities
Upper face (fronto-orbital, cranial vault)
See the list below:
-
Advancement of the fronto-orbital bandeau, alone or in combination with the midface as a monobloc or facial bipartition
-
New use of distraction as a means of cranial vault remodeling by gradual separation across resected stenotic sutures
Established indications for craniofacial DO include the following:
Congenital indications
See the list below:
-
Nonsyndromic craniosynostosis - Coronal (bilateral or unilateral) or sagittal
-
Syndromic craniosynostosis - Apert, Crouzon, and Pfeiffer syndromes
-
Cleft lip and palate
-
Hemifacial microsomia
-
Pierre Robin syndrome [10]
Acquired indications
See the list below:
-
Posttraumatic deformity (midfacial retrusion or mandibular collapse)
-
Atrophy of edentulous segments
-
Oncologic mandible defects
Relevant Anatomy
See Pathophysiology.
Contraindications
Several factors can limit or preclude the use of distraction osteogenesis (DO) to correct craniofacial deformities. Few absolute contraindications to the use of this technique exist; however, caution is advised in patients who, for one reason or another, will not comply with the distraction regime.
From a surgical standpoint, an adequate bone stock is necessary to accept the distraction appliances and to provide suitable opposing surfaces capable of generating a healing callus. Therefore, in patients who have undergone several craniofacial procedures in the past, the facial skeleton may exist in several small discontinuous fragments unsuitable for distraction. In these cases, bone grafting the gaps first may be possible, followed by distraction on a delayed basis.
Age should also influence the surgeon's decision. Although distraction has enabled procedures to be performed in patients of a much younger age than with conventional craniofacial surgery, exercise caution in the very young because working with the small fragile bones in these patients becomes increasingly difficult. Also, remember that many relatively straightforward cases exist, in which equivalent results can be obtained with conventional techniques. In such scenarios, prudence calls for use of the time-tested procedures. Such caution is especially true in orthognathic repositioning for most dentofacial deformities.
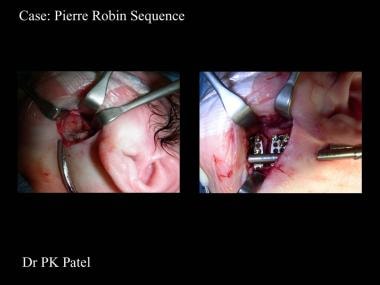
-
Intraoperative photographs of distractor placement.
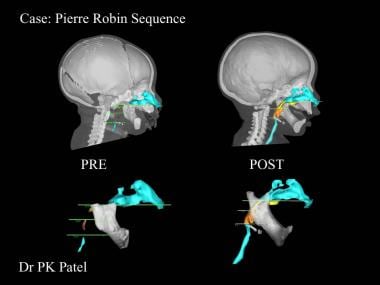
-
Typical airway changes after mandibular distraction.





