Overview
Any drug with the potential to cause toxic reactions to structures of the inner ear, including the cochlea, vestibule, semicircular canals, and otoliths, is considered ototoxic. Drug-induced damage to these structures of the auditory and balance system can result in hearing loss, tinnitus, and dysequilibrium or dizziness. The propensity of specific classes of drugs to cause ototoxicity has been well established, and over 100 classes of drugs have been associated with ototoxicity. [1]
Ototoxicity came to the forefront of clinical attention with the discovery of streptomycin in 1944. Streptomycin was used successfully in the treatment of tuberculosis; however, a substantial number of treated patients were found to develop irreversible cochlear and vestibular dysfunction. [2] These findings, coupled with ototoxicity associated with later development of other aminoglycosides, led to a great deal of clinical and basic scientific research into the etiology and mechanisms of ototoxicity. Today, many well-known pharmacologic agents have been shown to have toxic effects to the cochleovestibular system. The list includes aminoglycosides and other antibiotics, platinum-based antineoplastic agents, salicylates, quinine, and loop diuretics.
An image depicting inner ear anatomy can be seen below.
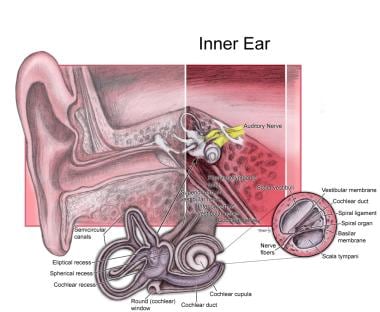 Inner ear anatomy.
Inner ear anatomy.
Ototoxicity is typically associated with bilateral high-frequency sensorineural hearing loss and tinnitus. Hearing loss can be temporary but is usually irreversible with most agents. Generally, antibiotic-induced ototoxicity is bilaterally symmetrical, but it can be asymmetrical. The usual time of onset is often unpredictable, and marked hearing loss can occur even after a single dose. Additionally, hearing loss may not manifest until several weeks or months after completion of antibiotic or antineoplastic therapy.
Vestibular injury is also a notable adverse effect of aminoglycoside antibiotics and may appear early on with positional nystagmus. If severe, vestibular toxicity can lead to dysequilibrium and oscillopsia.
Permanent hearing loss or balance disorders caused by ototoxic drugs may have serious communication, educational, and social consequences. Therefore, the benefits of ototoxic drugs must be weighed against the potential risks, and alternative medications should be considered when appropriate. Management emphasis is on prevention, as most hearing loss is irreversible. No therapy is currently available to reverse ototoxic damage; however, basic scientists and clinicians are continually seeking to find new methods to minimize ototoxic injury while retaining the therapeutic efficacy of these agents. For severe hearing loss, amplification may be the only treatment option.
Aminoglycosides
Since their introduction in 1944, multiple aminoglycoside preparations have become available, including streptomycin, dihydrostreptomycin, kanamycin, gentamicin, neomycin, tobramycin, netilmicin, and amikacin. The aminoglycosides are bactericidal antibiotics that bind to the 30S ribosome and inhibit bacterial protein synthesis. They are active only against aerobic gram-negative bacilli and cocci.
Although the ototoxic effects of aminoglycosides are well documented, this class of drugs is still widely used today. Aminoglycosides may be used in combination with penicillin in staphylococcal, streptococcal, and, especially, enterococcal endocarditis. An aminoglycoside is often added to a beta-lactam antibiotic when serious Pseudomonas aeruginosa infections are treated. Aminoglycosides can also be effective in the treatment of tuberculosis. Particular groups of patients, including those with cystic fibrosis, immune dysfunction, and certain chronic infectious disease, are more likely to be treated with this class of antibiotics.
Of all ototoxic drugs, the aminoglycosides are the most vestibulotoxic, although they vary greatly in their differential effects on the vestibular and cochlear systems. [3] Kanamycin, amikacin, neomycin, and dihydrostreptomycin are preferentially cochleotoxic. Gentamicin affects both cochlear and vestibular systems; however, most authors include gentamicin as primarily vestibulotoxic. Streptomycin, tobramycin, and netilmicin are also primarily vestibulotoxic.
Pathophysiology
Aminoglycoside toxicity primarily targets renal and cochleovestibular systems; however, no clear correlation exists between degree of nephrotoxicity and ototoxicity. Cochlear toxicity that results in hearing loss usually begins in the high frequencies and is secondary to irreversible destruction of outer hair cells in the organ of Corti, predominantly at the basal turn of the cochlea. In the vestibular apparatus, type I hair cells are more sensitive than type II hair cells. [4]
Aminoglycosides are cleared more slowly from inner ear fluids than from serum, and therefore a latency exists to the ototoxic effects of aminoglycosides. This latency can result in progression of hearing loss or onset of hearing loss after cessation of aminoglycoside treatment. Continuing to monitor the patient for cochleotoxic and vestibulotoxic effects up to 6 months after cessation of aminoglycoside treatment is important.
The exact mechanisms of aminoglycoside ototoxicity remain unknown. Many cellular processes have been implicated, and this continues to be an active area of research. [5] It does appear that aminoglycoside agents must enter hair cells to induce cell death. [6] After entry into hair cells, many cellular mechanisms and processes may be involved. Disruption of mitochondrial protein synthesis, formation of free oxygen radicals, activation of c-Jun N-terminal kinase (JNK), and activation of caspases and nucleases can ensue. Aminoglycosides have also been shown to have direct effects on cellular membrane potentials through interactions with potassium channels. [7] In addition, aminoglycoside interaction with transition metals such as iron and copper potentiate the formation of free radicals and further cell damage.
Ultimately, some interaction of these many processes leads to permanent loss of sensory hair cells in both the cochlea and vestibular apparatus, resulting in permanent hearing loss or balance dysfunction. [8, 9]
Aminoglycoside ototoxicity is likely multifactorial, and further investigation continues. Some studies are investigating iron chelators and antioxidants as possible agents to prevent hearing loss during therapy, while other studies are exploring forms of gene therapy as future treatment options. Currently, no treatment is available apart from amplification and cochlear implantation; therefore, prevention is paramount.
Epidemiology
In certain countries, antibiotics are prescribed freely or are available without prescription. In these areas, aminoglycosides cause as many as 66% of cases of deaf mutism. Depending on agent and dosing, up to 33% of adult patients may have audiometric changes with aminoglycoside treatment. Vestibular toxicity is also well documented; it occurs in as many as 4% of adult patients. The incidence of patients who experience toxicity due to aminoglycosides may be decreasing because of improvements in monitoring and heightened awareness.
Studies indicate that cochlear toxicity from aminoglycosides is less common in neonates and children than in adults. The incidence of aminoglycoside-induced cochlear toxicity in neonates has been estimated at around 2%. [10]
Risk factors
Certain factors may put patients at increased risk for ototoxicity. Aminoglycoside ototoxicity is more likely to occur with larger doses, higher blood levels, or longer duration of therapy. Other high-risk patients include elderly patients, those with renal insufficiency, those with preexisting hearing problems, those with a family history of ototoxicity, and those receiving loop diuretics or other ototoxic or nephrotoxic medications.
A genetic predisposition exists in mitochondrial RNA mutation 1555A>G, which has been found to be associated with nonsyndromic and aminoglycoside-induced hearing loss. [11] The defect creates an alteration in mitochondrial protein synthesis. Chinese patients with this defect have more rapid and severe effects of aminoglycoside ototoxicity. Careful evaluation of family history is important and may prevent many cases. In addition, some have suggested that high-risk populations (eg, patients with cystic fibrosis, a family history, and immune dysfunction) should be screened for this mutation. [12, 9]
A literature review by Scott et al indicated that variants in the genes ACYP2 and TPMT increase patient susceptibility to cisplatin-induced ototoxicity. While an ACYP2 variant has been linked to greater susceptibility in children and adults, variants in TPMT have been associated specifically with pediatric susceptibility. [13]
Signs and symptoms
Clinically, acute cochlear damage may present as tinnitus. Early hearing loss may go unrecognized by the patient and initially manifest as an increase in the threshold of highest frequencies (>4000 Hz). With progression, lower speech frequencies are affected and the patient may become profoundly deaf if the drug is continued. If the drug is stopped early in the course of damage, further loss may be prevented, and partial recovery of auditory thresholds may be possible. However, the loss is usually permanent.
Symptoms of vestibular toxicity typically include imbalance and visual symptoms. The imbalance is worse in the dark or in situations in which footing is uncertain. Spinning vertigo is unusual. The visual symptoms, called oscillopsia, occur only when the head is moving. Quick movements of the head are associated with transient visual blurring. This can cause difficulties with seeing signs while driving or recognizing people's faces while walking. Clinically, nystagmus may be present as an early sign.
Prevention
Prevention of aminoglycoside ototoxicity involves careful monitoring of serum drug levels and renal function as well as hearing evaluations before, during, and after therapy. Measure baseline audiometric function before therapy; however, this is not always possible in acute situations. Daily administration decreases incidence of ototoxicity and should be considered whenever possible. Conscientiously identify high-risk patients and select alternative antibiotics for them. Lastly, because aminoglycosides remain in the cochlea long after therapy has ended, instruct patients to avoid noisy environments for 6 months after therapy completion because they remain more susceptible to noise-induced cochlear damage.
Animal studies have involved the administration of free-radical scavengers, iron chelators, and inhibitors of cell death pathways as possible mechanisms to prevent ototoxicity. Several promising agents, including vitamin E, alpha lipoic acid, Ebselen (an organic selenium compound), and ginkgo biloba, have been found to be otoprotective and effective in some animal studies. Further clinical trials are needed to determine if the protective mechanisms demonstrated in animal studies can be replicated in patients while maintaining therapeutic effects of the aminoglycosides. [8, 14]
A study by Kocyigit et al suggested that the antioxidant N-acetylcysteine (NAC)—which has been in use for years to treat hepatoxicity from acetaminophen overdose and has a relatively low side-effect profile with long-term oral administration—can also protect against amikacin ototoxicity. The study involved 46 patients who received amikacin for peritoneal dialysis-related peritonitis, with NAC being administered to half of the patients and a placebo being given to the other half. Otoacoustic emission measurements in the NAC and placebo groups indicated that NAC protected cochlear function, particularly at higher frequencies. In addition, oxidative stress measurements indicated that antioxidant status significantly improved in the NAC patients. [15]
A systematic review by Kranzer et al also indicated that NAC has an otoprotective effect when administered with aminoglycosides. Their review of three studies included 146 patients with end-stage renal failure who showed reduced ototoxicity with NAC administration while undergoing aminoglycoside treatment. They identified a pooled relative risk for otoprotection of 0.14 but cautioned that the overall quality of the study evidence was low due to risk of bias from study design. [16] More robust research is needed to determine the clinical significance of NAC's otoprotective benefit.
Specific aminoglycosides
Streptomycin
Streptomycin was the first clinically applied aminoglycoside and was used successfully against gram-negative bacteria in the past. Streptomycin preferentially affects the vestibular system rather than the auditory system. Vestibular damage due to streptomycin is common with prolonged use and in patients with impaired renal function. Because of its toxicity, and because of widespread resistance, this agent is used infrequently today. However, streptomycin use has risen for treatment of tuberculosis.
Gentamicin
As with streptomycin, gentamicin has a predilection for the vestibular system. Therapeutic peak serum levels of 10-12 mcg/mL are generally considered safe but may still be toxic in some patients. Carefully adjust dosing in patients with renal disease.
Neomycin
This agent is one of the most cochleotoxic aminoglycosides when administered orally and in high doses; therefore, systemic use generally is not recommended. Neomycin is among the slowest aminoglycosides to clear from the perilymph; consequently, delayed toxicity (1-2 wk) may ensue after discontinuation of therapy. Neomycin is mainly used as an effective otic and ototopical agent. Although neomycin is generally considered safe when used topically in the ear canal or on small skin lesions, equally effective alternatives are available.
Kanamycin
Although less toxic than neomycin, kanamycin is quite ototoxic. Kanamycin has a propensity to cause profound cochlear hair cell damage, marked high-frequency hearing loss, and complete deafness. The damaging effect is primarily to the cochlea, while the vestibular system is usually spared injury. Kanamycin has limited clinical use today. As with neomycin, parenteral administration is generally not recommended.
Amikacin
Amikacin is a derivative of kanamycin and has very little vestibular toxicity. Its adverse effects primarily involve the auditory system; however, it is considered less ototoxic than gentamicin. In the treatment of severe infections, amikacin is mainly indicated on the basis of results of susceptibility tests and patient response. [17]
Tobramycin
Ototoxicity of tobramycin is similar to that of amikacin; high-frequency hearing loss results. As with kanamycin, vestibular toxicity is less common. Tobramycin is frequently used in otic and topical preparations. Topical use, although not without controversy, is generally considered safe.
Other Antibiotics
Macrolides
Erythromycin was introduced in 1952 and has seen widespread use in clinical medicine. Generally, erythromycin is considered a safe medication. Erythromycin has been considered the substitute of choice in group A streptococcal and pneumococcal infections for penicillin-sensitive individuals. Erythromycin remains the antibiotic of choice for Legionella pneumonia and other atypical pneumonias. The first reports of ototoxicity were not noted until 1973. Since then, only sporadic cases of ototoxicity have been reported, and they have generally been reversible. These patients tended to have other risk factors, including renal failure, hepatic failure, doses of more than 4 g/d, and intravenous administration. Clinically significant hearing loss also has been reported in recipients of renal allografts who were treated with intravenous erythromycin. Onset is generally within 3 days of starting treatment. Speech frequencies may be affected rather than higher frequencies.
Azithromycin and clarithromycin are newer macrolide antibiotics. These antibiotics have seen widespread clinical use because they have fewer GI side effects and a broader antimicrobial spectrum than erythromycin. However, some reports have pointed to possible ototoxic effects. [18] Through systematic review, Ikeda et al uncovered 78 cases of macrolide-associated sensorineural hearing loss documented via audiometry across 44 studies, including in association with oral azithromycin and clarithromycin treatment at standard doses. In the majority of cases (92.3%), hearing loss was reversible after drug cessation. [19] Thus, subjective complaints of hearing loss in patients taking macrolides should be respected and merit discontinuation of the agent and objective evaluation of hearing.
A study by Vanoverschelde et al indicated that macrolide use increases the risk of developing prevalent tinnitus by 25%. The association with tinnitus was found to be especially prominent in individuals in whom the cumulative macrolide dose reached more than 14 defined daily doses (DDD) and for patients on intermediate- or long-acting macrolides. [20]
Vancomycin
Vancomycin is a glycopeptide antibiotic that was introduced in the 1950s. It is a commonly used medication in light of its efficacy in methicillin-resistant staphylococcal infections. Several reports of ototoxicity, usually manifesting as tinnitus, have been presented in patients with elevated serum concentrations attributed to renal failure or in those patients receiving concomitant aminoglycoside therapy. [21] The data are unclear but suggest that ototoxicity is reversible in at least some individuals. No studies demonstrate conclusive evidence of ototoxicity with vancomycin administration alone and in therapeutic doses. No recommendations have been made regarding its use; however, the authors suggest caution with coadministration of vancomycin and other ototoxic agents, and documentation of vancomycin serum levels.
Loop Diuretics
Loop diuretics exert therapeutic effects at the loop of Henle. This class of medications includes several different chemical groups, including sulfonamides, phenoxyacetic acid derivatives, and heterocyclic compounds. These drugs are used to treat congestive heart failure, renal failure, cirrhosis, and hypertension. The most effective and frequently used diuretics (eg, ethacrynic acid, furosemide, bumetanide) can cause ototoxicity. Several less-commonly used loop diuretics also have been experimentally shown to cause ototoxicity; this group includes torsemide, azosemide, ozolinone, indacrinone, and piretanide.
Pathophysiology
The ototoxic effects of loop diuretics seem to be associated with the stria vascularis, which is affected by changes in the ionic gradients between the perilymph and endolymph. These changes cause edema of the epithelium of the stria vascularis. Evidence also suggests that endolymphatic potential is decreased; however, this is usually dose dependent and reversible.
Ototoxicity caused by ethacrynic acid seems to develop more gradually and takes longer to resolve than that caused by furosemide or bumetanide. Overall, ototoxicity attributed to this group of medications is usually self-limited and reversible in adult patients, although irreversible hearing loss has been reported in neonates.
Epidemiology
Ototoxicity is estimated to occur in 6-7% of patients taking loop diuretics. Occurrence of loop diuretic ototoxicity depends on several factors, including dose, infusion rate, history of renal failure, and co-administration of other ototoxic agents.
Signs and symptoms
Depending on the particular loop diuretic, patients usually relate a history of hearing loss soon after taking the agent. Patients also may complain of tinnitus and dysequilibrium; however, these symptoms are less common and seldom occur without hearing loss. Some patients may experience permanent hearing loss, especially those with renal failure, those receiving high doses, or those receiving aminoglycoside antibiotics concurrently.
Prevention
Prevention of ototoxicity caused by loop diuretics consists of using the lowest doses possible to achieve desired effects and avoiding rapid infusion rates. Additionally, the risk factors associated with administration of these drugs must be diligently assessed, including co-administration of other ototoxic medications and history of renal failure. As potentiation and synergism of ototoxic effects of aminoglycosides and loop diuretics is well documented, co-prescription of these drugs is not recommended.
Antineoplastic Agents
Antineoplastic agents most commonly associated with ototoxicity are the platinum-based compounds cisplatin and, to a lesser degree, carboplatin. These agents are widely used in gynecologic, lung, central nervous system, head and neck, and testicular cancers. Antineoplastics are cell-cycle nonspecific alkylating agents that insert into the DNA helix, disrupting replication.
Cisplatin is distributed widely, but the highest concentrations are found in the kidneys, liver, and prostate. Cisplatin irreversibly binds to plasma proteins and can be detected up to 6 months after completion of therapy. Carboplatin is not protein bound and is more readily cleared by the kidneys. Dose and efficacy of cisplatin and carboplatin are limited largely by adverse effects. Most notably, these agents produce nephrotoxicity and ototoxicity with increasing dose.
Pathophysiology
The mechanism of platinum ototoxicity is mediated by free-radical production and cell death. Platinum compounds damage the stria vascularis in the scala media and cause outer hair cell death beginning at the basal turn of the cochlea. Free radical species are produced by NADPH oxidase in the inner hair cells following cisplatin exposure. NADPH oxidase is the enzyme that catalyses the formation of superoxide radicals. A particular form of NADPH oxidase, NOX3, is highly and selectively produced in the inner ear and is an important source of free radical generation in the cochlea, which might contribute to hearing loss. [8] The free radicals generated by this mechanism then lead to mitochondria-mediated and caspase-mediated apoptotic cell death, and ultimately permanent hearing loss.
Epidemiology
Incidence and severity of ototoxicity depend on dose, infusion rate, and number of cycles, renal status, and co-administration of other ototoxic agents. Incidence and severity is also higher in the pediatric population and in patients receiving radiation therapy to the head and neck. Some studies describe a hearing loss of 61% of children receiving platinum-based chemotherapy. [22] This is comparable with earlier studies.
A study by Funt et al found that of 106 patients who underwent high-dose chemotherapy (which included high-dose carboplatin) for germ cell tumors, moderate to profound hearing loss in the speech frequencies (0.5-4 kHz) occurred in 70 (66%). Patients who, prior to such chemotherapy, had moderate to profound hearing loss only in the high frequencies (6-8 kHz) were particularly likely to experience clinically significant hearing loss in the speech frequencies after high-dose chemotherapy (94% vs 61% of the other patients). [23]
A prospective cohort study by Waissbluth et al of 28 pediatric cancer patients who underwent platinum-based chemotherapy (with cisplatin and/or carboplatin) reported that by mean 21.5-month follow-up, 28.6% had sensorineural hearing loss. [24] Another prospective cohort study by Waissbluth and colleagues found that in 12 pediatric patients who were treated with cisplatin and/or carboplatin, 58.3% had suffered hearing loss by median 11.9-year follow-up. [25]
Risk factors
The following risk factors have been identified for development and potentiation of platinum-induced ototoxicity: (1) high dose and increasing number of cycles, (2) concurrent or past cranial irradiation, (3) age extremes, (4) dehydration, (5) co-administration of other ototoxic agents, and (6) renal failure.
In the aforementioned research by Waissbluth et al, a greater risk of sensorineural hearing loss was found in pediatric patients who received a cumulative cisplatin dose of over 400 mg/m2, who underwent cranial irradiation, or who were below age 5 years. [24]
Signs and symptoms
Patients with platinum-induced ototoxicity may report tinnitus and experience subjective hearing loss. Hearing loss associated with cisplatin toxicity is usually bilateral, sensorineural, irreversible, and progressive. High-frequency hearing is typically affected first, but loss may not appear until several days or months after the last dose. Conversely, severe hearing loss may occur after a single dose.
Prevention
Obtain baseline audiograms and periodic follow-up audiograms during therapy for all patients receiving these agents. Perform these studies immediately before subsequent drug cycles so the maximal effect of the previous cycle can be determined. Lastly, patients should continue to undergo audiometric testing because of significant drug retention long after completion of therapy. Also advise patients to avoid noise exposure for up to 6 months.
Studies have explored agents such as alpha-tocopherol (a vitamin E derivative), sodium thiosulfate, D-methionine (an amino acid), salicylates, iron chelators, N-acetylcysteine, caspase or calpain inhibitors, and even gene therapy as preventives if used in combination with platinum-based chemotherapeutic agents. These studies have shown significant benefit in animal models but must be replicated in human models while preserving the antineoplastic effects of agents such as cisplatin. [14]
A multicenter trial by Freyer et al studied the effects of sodium thiosulfate versus observation in a randomized trial of 104 pediatric patients undergoing a cisplatin-containing chemotherapy regimen for various malignancies. Forty-nine patients received intravenous sodium thiosulfate after each cisplatin dose, while 55 were observed. The development of hearing loss was significantly lower in the sodium thiosulfate group (28.6% of participants) than in the control group (56.4% of patients). It should be noted that 3-year overall survival was significantly lower in the sodium thiosulfate group (45% vs 84% in observed). While the study's results were promising, the authors concluded that further investigation is warranted to define the role of sodium thiosulfate in cisplatin-based treatment protocols. [26]
Salicylates
Acetylsalicylic acid, commonly known as aspirin, is used widely for its anti-inflammatory, antipyretic, and analgesic properties. Aspirin is an inhibitor of platelet aggregation and is used to treat patients with a history of transient ischemic attacks, stroke, unstable angina, or myocardial infarction. Acetylsalicylic acid is absorbed rapidly after oral administration and is hydrolyzed in the liver to its active form, salicylic acid. Therapeutic levels range from 25-50 mcg/mL for analgesic and antipyretic effects to 150-300 mcg/mL for treatment of acute rheumatic fever. However, tinnitus can occur at serum levels as low as 200 mcg/mL.
Pathophysiology
Salicylic acid quickly enters the cochlea, and perilymph levels parallel serum levels. Increasing levels produce tinnitus and, generally, a reversible flat sensorineural hearing loss. The mechanism is multifactorial but appears to cause metabolic rather than morphologic changes within the cochlea.
Epidemiology
Incidence of ototoxicity is as high as 1% and is most commonly observed in elderly patients, even at low doses.
Risk factors
Risk factors associated with salicylate ototoxicity include high dose, elderly age, and dehydration.
Signs and symptoms
Tinnitus is the most common adverse effect of salicylate toxicity. Other adverse effects include hearing loss, nausea, vomiting, headache, confusion, tachycardia, and tachypnea. Hearing loss is typically mild to moderate and bilaterally symmetric. Recovery usually occurs 24-72 hours after cessation of the drug.
The onset of tinnitus has been used in the past as an early sign of ototoxicity. Later studies found that the onset of tinnitus should not be used as a predictor of serum salicylate level because ototoxic effects can be present at low blood levels. [27]
Treatment
Salicylate toxicity is treated by electrolyte monitoring and fluid administration, with the addition of alkaline diuresis, if necessary. Oxygen administration and mechanical ventilation also may be needed in severe cases.
Quinine
Derived from cinchona tree bark, quinine was historically used to treat malaria and for its antipyretic qualities. Use today is limited by availability of less-toxic alternatives. Quinine is occasionally used to treat nocturnal leg cramps and as an adjunct to antimalarial therapy. Quinine primarily undergoes hepatic metabolism.
Signs and symptoms
Quinine toxicity can produce tinnitus, hearing loss, vertigo, headache, nausea, and vision loss. Hearing loss is usually sensorineural and reversible. A characteristic sensorineural notch often is present at 4000 Hz. Irreversible hearing loss rarely has been reported with quinine use.
Treatment
Treatment for quinine ototoxicity mainly consists of discontinuation of therapy; amplification can be used in rare cases of irreversible hearing loss.
Methods of Audiologic Monitoring
Baseline testing should be obtained before the start of chemotherapeutic agents, especially cisplatin and carboplatin. In those patients taking aminoglycosides, baseline testing should be obtained within 72 hours of the start of treatment. Patient selection, complicating medical factors, level of consciousness, and age play a role in selecting methods for early detection.
Baseline testing, when possible, should be comprehensive. At a minimum bilateral pure-tone air-conduction thresholds at standard audiometric frequencies from 0.25 to 8 kHz should be obtained. If equipment allows threshold frequencies about 8 kHz should also be measure. Additional testing would include a case history including family history, otoscopic examination, immittance or bone-conduction testing, speech reception thresholds, and word recognition scores.
For patients unable to cooperate or tolerate standard testing objective testing with otoacoustic emission (OAE), EChochG, and/or auditory brainstem response (ABR) testing should be obtained for documentation and monitoring. OAE testing is specifically sensitive to the status of the outer hair cells in the cochlea and is a relatively efficient objective test to assess cochleotoxicity. EChochG is a more invasive and time-consuming transtympanic test that evaluates cochlear and neural responses. ABR is also a time-consuming test and is additionally limited to stimuli responses to frequencies between 1 and 4 kHz.
Monitoring should continue during therapy at regular intervals. With any sign of ototoxicity, measures should be taken to reduce toxicity as possible. For aminoglycoside antibiotics, weekly to bi-weekly testing has been suggested. For chemotherapeutic medication, weekly testing is recommended. The interval for testing should decrease with the first sign of ototoxic change. Monitoring should continue for at least 3-6 months following cessation of the potentially ototoxic medication or until the hearing stabilizes.
Definition and grades of ototoxicity
The definition and criteria for ototoxicity has been established by the American Speech-Language-Hearing Association (ASHA), the National Cancer Institute Common Terminology Criteria for Adverse Events (CTCAE), and by Brock.
ASHA define ototoxicity as: (a) 20db or greater decrease in pure-tone threshold at one frequency, (b) 10db or greater decreased at 2 adjacent frequencies, or (c) loss of response at 3 consecutive test frequencies in which responses were previously obtained, when OAE or ABR is used.
The CTCAE and Brock have determined grades to further define ototoxicity as follows:
-
CTCAE ototoxicity grades 1-4
Grade 1 - Threshold shift or loss of 15-25 dB relative to baseline, averaged at two or more contiguous frequencies in at least one ear.
Grade 2 - Threshold shift or loss of > 25-90 dB, averaged at two contiguous test frequencies in at least one ear
Grade 3 - Hearing loss sufficient to indicate therapeutic intervention, including hearing aids (eg, > 20 dB bilateral HL in the speech frequencies; > 30 dB unilateral HL; and requiring additional speech-language related services)
Grade 4 - Indication for cochlear implant and requiring additional speech-language related services
-
Brock's hearing loss grades
Grade 0 - Hearing thresholds less than 40 dB HL at all frequencies
Grade 1 - Thresholds 40 dB or greater at 8,000 Hz
Grade 2 - Thresholds 40 dB or greater at 4,000-8,000 Hz
Grade 3 - Thresholds 40 dB or greater at 2,000-8,000 Hz
Grade 4 - Thresholds at 40 dB or greater at 1,000-8,000 Hz
Knight et al suggest that traditional CTCAE has under-reported ototoxicity and minimized the significance of hearing loss in children treated with platinum-based chemotherapeutic agents. [22]
Vestibulotoxicity
Vestibulotoxic criteria have not been well established. Standard battery of vestibular testing, including caloric testing, VEMP, and VNG, are useful for documenting vestibulopathy. In addition, given oscillopsia as the main symptom, addition of rotational testing, especially at high frequencies, is recommended. The presence of rotational function may not be evident after caloric testing and can indicate intact responses in other areas of vestibular sensitivity that may otherwise be missed. Intact function may separate the patient who will benefit from vestibular rehabilitation from the patient who will not.
Patients with vestibulotoxicity have bilateral deficits and will not present with nystagmus or complaints of vertigo. Clinical tests such as dynamic visual acuity testing, bedside head thrust testing, [28] eye chart testing, and horizontal head impulse testing [29] have been used to examine the deficit of the vestibulo-ocular reflex (VOR) in patients with bilateral vestibulopathy caused by vestibulotoxic medications. Unfortunately, the subjective reports of patients do not correlate well with testing parameters. [28]
A bedside test for dynamic visual acuity is the eye chart test. In this examination, the examiner holds a miniature version of an eye chart about 18 inches in front of the subject to be tested. The person reads the smallest line possible. This represents the person's best normal vision. The examiner then rotates the head forward and backward about once per second and asks the person to read the smallest line possible. A person with an intact vestibular system and VOR should be able to read the same line. A person with oscillopsia, however, can only read the lines with much bigger print. The number of lines "lost" is indicative of the degree of oscillopsia. [30]
Another bedside test used to assess the VOR is the head thrust. The head-thrust test is performed by grasping the patient’s head and applying brief small amplitude, high acceleration head thrusts, first to one side and then to the other. The patient is asked to fixate on the examiner’s nose and the examiner watches for ‘catch-up saccades,' a sign of decreased horizontal VOR gain on the side ipsilateral to which the head had been turned. [31]
Management
The primary concern is to maintain patient communication capabilities during what is generally a serious illness. Consult an audiologist early for baseline assessment. Additionally, it is essential to counsel patients and parents regarding the risks of ototoxic medications and emphasize the importance of prompt reporting of symptoms such as tinnitus, hearing loss, oscillopsia, and dysequilibrium.
High-frequency sounds provide major contributions to speech intelligibility and can therefore have significant effects on communication and listening abilities. When hearing loss occurs, referring patients appropriately for hearing amplification to prevent communication, social, and education set-backs is essential.
The vestibular system is able to compensate for unilateral loss. Vestibular rehabilitation is recommended to aid an individual in facilitating compensation. In bilateral loss, rehabilitation will aid the patient in using other mechanisms to improve balance and function.
Topical Otic Preparations
Certain topical potentially ototoxic drugs that are commonly used in the ear for treatment of acute otitis media (AOM) and chronic suppurative otitis media (CSOM) have recently been evaluated and a consensus position has been presented by the American Academy of Otolaryngology-Head and Neck Surgery. The most commonly used ototopical medication is a combination of neomycin-polymyxin. Newer, available ototopical medications are of the class fluoroquinolones, including ciprofloxacin and dexamethasone (Ciprodex) and ofloxacin otic preparations.
The following recommendations have been made by the ototopical antibiotic consensus panel (updated 2004) [12] :
When possible, topical antibiotic preparations free of potential ototoxicity should be used in preference to ototopical preparations that have the potential for otologic injury if the middle ear or mastoid is open. (Aminoglycoside-containing topical drops are not FDA approved for use in the middle ear).
If used, potentially ototoxic antibiotic preparation should be used only in infected ears. Use should be discontinued after the infection has resolved. Round window permeability contributes to ototoxic effects. Animal data suggest that the thickened, edematous middle ear mucosa present in an infected ear may provide protection from ototoxicity.
If potentially ototoxic antibiotic drops are prescribed for use in the middle ear or mastoid, the patient/parent should be warned of the risk of ototoxicity. And should be instructed to call the physician should dizziness, vertigo, hearing loss, or tinnitus occur. The consensus panel did not feel routine auditory or vestibular monitoring was warranted.
If the middle ear and mastoid are intact and closed, then the use of potentially ototoxic preparations present no risk of ototoxic injury.
Overall, although evidence suggests that otologic injury from aminoglycoside ototopical preparations is infrequent, the evidence also suggests that they offer no advantage over nontoxic agents. Therefore, this author discourages routine use of neomycin ototopical preparations for AOE and CSOM and recommends fluoroquinolone preparations, such as ofloxacin otic drops and Ciprodex drops, especially in persons with open middle ear space or ventilation ear tubes.
A literature review by Harris et al indicated that quinolones, when used in postmyringotomy prophylaxis, are equal to or better than aminoglycosides against chronic suppurative otitis media. Four studies showed that the clinical outcomes for the two types of drugs were not significantly different, while two trials showed the quinolone clinical cure rate to be better than that for aminoglycosides (93% vs 71%, respectively). [32]
Other ototopical medications, including antiseptics such as Vosol and Gentian violet, have been implicated in causing ototoxicity. In preparation for surgical interventions, povidone-iodine has been shown to be safe for middle ear surgeries; however, chlorhexidine is toxic if it reaches the inner ear and should not be used. [33]
Therapeutic Toxicity
Over the past decade, intratympanic gentamicin has become a major treatment modality for intractable Ménière disease. Although early vestibular ablation used streptomycin, gentamicin is now the preferred preparation because it is more vestibulotoxic than cochleotoxic and therefore may ablate vestibular function while preserving hearing. The idea is that unilateral vestibular loss allows compensation from the contralateral vestibular system, allowing for improved overall function.
Gentamicin therapy is induced with 30-40 mg weekly until signs of unilateral vestibular loss are seen. Kaplan et al showed that with this regimen most patients experience ototoxicity by day 12. [34] In a meta-analysis including 15 trials and 627 patients, 74.7% of patients were shown to achieve complete vertigo control with intratympanic gentamicin treatment; complete or substantial control was achieved in 92.7% of patients. [35, 9]
-
Inner ear anatomy.





