Overview
Over the past 3 decades, expanding knowledge of vocal fold anatomy and physiology has revolutionized the clinical and surgical practice of laryngology. Since Hirano's original description of the layered microstructure of the human vocal fold in the 1970s, [1] increasingly sophisticated diagnostic and surgical techniques have evolved to more precisely address and preserve vocal production. Innovative diagnostic modalities have grown out of an improved understanding of the critical importance of vocal-fold pliability to voice production. Videostroboscopy has evolved as the most practical and useful technique for the clinical evaluation of the visco-elastic properties of the phonatory mucosa. [2]
Video documentation of laryngeal anatomy along with its mechanical function is a painless, office-based procedure done with topical anesthesia and is essential for state-of-the-art management of human voice disorders. Videolaryngoscopy with stroboscopy is the essential diagnostic procedure for the evaluation of laryngeal mucosa, vocal fold motion biomechanics, and mucosal vibration. [3, 4] These are the key elements for detecting and assessing pathology as well as determining the impact on voice and airway function.
Stroboscopy is a special method used to visualize vocal fold vibration.5 22 It uses a synchronized, flashing light passed through a flexible or rigid telescope. The flashes of light from the stroboscope are synchronized to the vocal fold vibration at a slightly slower speed, allowing the examiner to observe vocal fold vibration during sound production in what appears to be slow motion.
This slow motion picture is an illusion, as the speed of actual vocal fold vibration is not changed by stroboscopy. This special viewing allows the voice care team to evaluate each vocal fold's vibration properties during the different phases of the vocal fold's vibration cycle. Because vocal fold vibration is so fast, the slow motion view is actually derived from many successive vibration cycles. The information acquired from the stroboscopic examination of the vocal folds is essential for planning effective phonomicrosurgery (endoscopic surgery to enhance vocal function). Optimal human voice production is dependent on optimal vocal fold vibration. This requires aerodynamically competent closure of vocal folds along with pliable phonatory mucosa.
Videostroboscopy fulfills several important requirements of a complete office voice examination. It provides useful, real-time information concerning the nature of vibration, an image to detect vocal pathology, and a permanent video record of the examination. As important as any of these aspects, stroboscopy substantially improves the sensitivity of subtle laryngeal diagnoses over techniques with continuous nonstroboscopic light sources (eg, rigid or flexible transnasal laryngoscopy).
Relevant anatomy
The vocal folds, also known as vocal cords, are located within the larynx (also colloquially known as the voice box) at the top of the trachea. They are open during inhalation and come together to close during swallowing and phonation. When closed, the vocal folds may vibrate and modulate the expelled airflow from the lungs to produce speech and singing. For more information about the relevant anatomy, see Vocal Cord and Voice Box Anatomy and Larynx Anatomy.
Background and Surgical Principle
The concept of stroboscopy is not new. For several centuries, stroboscopic images generated by using a flashing light source have been used to create the illusion of motion for entertainment. From the early 19th century, several examples illustrate the creation of moving-picture and optical toys, as well as scientific instruments. One device that used rotating disks to observe apparent motion, developed by a Viennese scientist named Stampfer, was called a stroboscope. This term is still used today to connote any pulsatile light-generating device designed to observe motion.
The history of using a stroboscopic light source to examine the larynx is nearly as long as that of the continuous light source, dating back to the introduction of the laryngeal mirror by Manuel Garcia in 1855. In 1874, Oertel conceived laryngeal stroboscopy, but the feasibility of the device was not realized until 1895, after the introduction of electricity. His device was comprised of a perforated wheel that interrupted the light used to illuminate the vocal folds so that vocal fold vibration could be perceived. The application of the stroboscopic light source allowed the observer to view the vibrating vocal folds in arrested or apparent slow motion, permitting detailed observations of the structure in the open or closed positions. Because of the limitations in illumination, precise control of the flashing frequency, and image quality, members of the scientific community did not embrace this technique.
In the early to mid 1900s, nearly 100 years after Plateau first suggested the use of an intermittent spark to illuminate moving objects to produce a stationary pattern for the purpose of study, H.E. Edgerton and associates developed gas discharge tubes for stroboscopy. They used an oscillator to control the frequency of the discharge and the flashing rate. Many of the principles of modern stroboscopic devices evolved from this early instrumentation.
Pioneers of modern strobolaryngoscopy include Dr. J.W. van den Berg at the University of Groningen, Dr. Rolf Timke at the University of Hamburg, Dr. Hans von Leden at the University of California, and Dr. Elimar Schonharl in Erlanger, who wrote the first definitive book on stroboscopic examination of the larynx in 1960. With the subsequent improvements in audio- and video-recording technology and with the ongoing advancements in optical image resolution and fiberoptic light-source intensity, the modern videostroboscopic unit can now produce a crisp, brightly illuminated, magnified image. [5, 6]
The Talbot law takes into account the physical reality that images on the human retina linger for 0.2 seconds after exposure (persistence of vision). Therefore, sequential images produced at intervals less than 0.2 seconds produce the illusion of a continuous image. This understanding, along with the concept of correspondence (interpretation of a corresponding portion of sequential images representing an object in motion), allows for the illusion of motion when rapidly produced still images are presented. Finally, a characteristic of the visual system permits interpretation of a series of slightly altered still images by filling in the gaps between frames and completing the illusion of continuous motion.
Strobolaryngoscopy takes advantage of these principles by producing intermittent light flashes in close relation to the frequency of the vocal-fold vibration. A microphone picks up the frequency of the examinee's sustained voice, which triggers the stroboscopic light source. With the provision that the vocal vibrations are periodic, a frequency of light flashes equal to the vocal frequency produces a clear, still image of the same portion of the vibratory cycle.
When the frequency of the flashes is slightly less than the vibration of the vocal fold, it causes a delay in the portion of each vibratory cycle illuminated, and the illusion of slow motion is obtained. However, in all healthy humans, vocal-fold vibrations are aperiodic to a greater or lesser degree. Therefore, strobolaryngoscopy does not demonstrate fine detail of each individual vibratory cycle; rather, it shows a pattern averaged over many successive nonidentical cycles. In this sense, it is a less-than-perfect illustration of the true vibratory nature.
Instrumentation
A videostroboscopic unit consists of a stroboscopic light source and microphone, a video camera, an endoscope, and a video recorder. Stroboscopy can be performed by using either rigid or flexible endoscopes; each has its own benefits and drawbacks.


Although flexible endoscopy is ideal for observing unaltered laryngeal behavior from various angles and for viewing the glottis through a narrow supraglottic aperture, it suffers from the low intensity of light carried through the long fiberoptic bundle to the tip of the narrow endoscope. With standard endoscopes, the light bouncing off objects being observed must then travel the length of the endoscope back to a camera or the operator's eye to be detected.
The introduction of distal-chip technology to flexible endoscopes, in which the camera is placed at the distal end of the scope, effectively lessened the drawback profile of flexible laryngoscopes. The enhanced digital picture quality with improved illumination has greatly improved the quality and resolution of transnasal laryngeal stroboscopy.

Rigid telescopic transoral endoscopy produces the optimal image to assess phonatory mucosal pliability because of its magnified bright image; however, it requires extracting the patient's tongue forward throughout the examination, which distorts the natural phonatory posture of the pharynx and larynx. Moreover, the patient must have suitable anatomy and the physical tolerance (gag reflex) to allow the clinician to visualize the entire glottis.
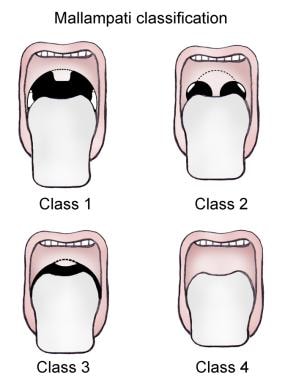
Rigid endoscopy additionally requires increased patient cooperation and amenable patient anatomy for successful visualization of the larynx. Recent research has suggested that the application of the Mallampati classification system is useful for predicting the adequacy of transoral rigid laryngoscopic exposure for stroboscopy. [7]
Clinical Application
Several parameters may be evaluated during the course of the stroboscopic examination. [8]
-
Fundamental frequency: The fundamental frequency is measured by using the strobe unit and is used to set the frequency of the light flashes. Strobe light is typically produced at a frequency several hertz slower than the vocal frequency to produce the illusion of a slow-motion vibratory cycle. An identical frequency is emitted in the locked mode that produces a still image of a single portion of the vibratory cycle.
-
Periodicity: Periodicity refers to the regularity of successive vocal vibratory cycles. Normal vibratory activity is regular and periodic.
-
Amplitude: Amplitude refers to the lateral excursion of the vocal folds during their displacement away from the midline during oscillation. It is highly dependent on pitch frequency (vocal fold tension) and loudness (subglottal lung pressure). Amplitude is generally graded as normal, less than normal, or greater than normal.
-
Symmetry: Normal motion (abduction and adduction) of the arytenoid cartilages is assessed during flexible or rigid telescopic laryngoscopy and vibratory characteristics of phonatory mucosa are assessed during stroboscopy.
-
Glottic closure: In a healthy person, the musculomembranous portion of the vocal folds completely closes during the vibratory cycle. The posterior cartilaginous glottis may remain partially open (posterior glottic chink) in some healthy people. [2]
-
Mucosal wave: Mucosal wave propagation reflects the rheological properties of phonatory mucosa (epithelium and superficial lamina propria) during a specific vocal task. Most hoarseness is due to diminished phonatory mucosal pliability from disease (acute and chronic), benign and malignant lesions, overuse, and general long-term use (vocal aging). Focal abnormalities of mucosal wave help to localize pathology in the vocal fold and direct strategies to manage the deficit.
Technique
Rigid strobolaryngoscopy
See the list below:
Videostrobolaryngoscopy begins by seating the patient in the examination chair at a height comfortable for the examiner. The patient leans forward with the neck flexed and the head extended at the atlo-occipital joint (Kirstein position).
Once in the appropriate position, it is often helpful to apply topical anesthesia (typically, Cetacaine spray) to the posterior aspect of the anterior tongue as well as the posterior oropharynx. The examiner should ensure that the microphone is calibrated properly and have the patient hold the laryngeal diaphragm against the thyroid lamina.
With mouth open and tongue protruded, the examiner retracts the tongue anteriorly and carefully inserts the rigid telescope. Optimal examination hinges on the examiner’s attention to achieving proper focus of the vocal folds. Proper focus demonstrates clear visualization of the subepithelial vasculature of the vocal fold. To avoid condensation on the scope, the tip of the telescope is dipped in hot water just prior to beginning the examination.
With the vocal folds in clear focus, the examiner can take the patient through a number of vocal tasks using the “ee” sound. This should be done at low, mid-range, and high frequency pitches as well as different volumes. Soft glottal onset and offset (low subglottal pressure), especially in high-pitch frequencies, may also be of use to help define some smaller lesions. The examiner is also able to comment on arytenoid and vocal fold mobility, glottic closure pattern, mucosal wave, and pliability. Ulcerative lesions or masses can also be observed.
This patient was evaluated for hoarseness. Stroboscopy shows the mucosal wave only with patient effort. Video courtesy of Vijay Ramakrishnan, MD.

Flexible strobolaryngoscopy
See the list below:
The patient is positioned as above. The nose and nasopharynx are typically anesthetized and decongested with a mixture of 0.25% phenylephrine and 2-3% lidocaine using an atomizer.
After allowing adequate time for decongestion, the flexible scope is inserted through the nose and passed in to position above the larynx. The examination described above can then be performed.
Diagnostic Findings
By increasing the illumination and evaluation of vibratory patterns, videostroboscopy has vastly increased the sensitivity of laryngologic diagnoses. [9] Despite the variations attributable to lesion size, concurrent vocal pathologies, and compensatory phonatory behaviors, generalizations can be made about stroboscopic findings accompanying specific true vocal-fold pathology. The most common benign laryngeal lesions and their typical stroboscopic findings are described below.
Vocal fold cysts
Vocal fold cysts are encapsulated, spheroid lesions containing either mucus or keratin located in the superficial lamina propria of the vocal fold. Keratin cysts are likely congenital and mucous cysts are likely acquired. They are generally unilateral, though several may be present at the time of diagnosis. On stroboscopy, the region of the cyst demonstrates diminished pliability, since the mucosal wave does not propagate normally through the region of the cyst. The exact characteristics of the mucosal-wave deficit depend on the size and location of the cyst. This is illustrated by the fact that small superior-surface cysts minimally affect vocal function.
Vocal fold polyps
Vocal fold polyps may be unilateral or bilateral. These lesions represent phonotraumatic pathology due to collision forces and shearing stresses in the superficial lamina propria. They may be of any consistency, ranging from gelatinous to fibrotic. Glottic closure may be compromised, leaving gaps anterior and posterior to the lesion in maximal closure. The vibratory patterns of the 2 vocal folds are asymmetric, with diminution of vibration near the lesion. A medial-surface polyp also typically disturbs the vibratory pattern of the contralateral vocal fold during closure.
Vocal fold nodules
Vocal fold nodules are bilateral fibrovascular lesions that are roughly symmetric sessile masses, approximately 2-7 mm in size, that occur in the center of the musculomembranous region at the basement-membrane zone between the overlying epithelium and the underlying superficial lamina propria. Glottic closure is compromised, especially in high pitch frequencies. Mucosal wave is usually preserved bilaterally, though the pliability and amplitude of excursion are decreased in the region of the nodule.
Sulcus vocalis
Sulcus vocalis refers to a spectrum of phonatory mucosal vibratory deficits in which the stroboscopic findings demonstrate zones of diminished mucosal pliability. This surface observation during stroboscopy reflects the diminished visco-elastic properties of the superficial lamina propria in that region.
Future Applications
Although videostroboscopy greatly expands the diagnostic sensitivity of some aspects (phonatory mucosal wave vibration) of office-based laryngoscopy, its interpretation depends on the skill and experience of the clinician performing the study (eg, requested vocal tasks), and, specifically, the skill and experience of the diagnostic interpreter. The quality of the images collected is directly related to the skill of the operator performing the procedure. In addition, research suggests that stroboscopic interpretation is a poorly generalizable research metric. [3] Even among the most experienced interpreters, inter-rater correlations for judging specific parameters is moderate (kappa = 0.61-0.81) at best. Although increased experience in reviewing stroboscopic results appears to have a modest positive effect on a clinician's intra-rater reliability, it does not necessarily improve inter-rater correlation in a group of similarly experienced examiners.
Several technologies have been developed to improve objective measurements of the amplitude of vibration and mucosal wave. Software was developed to measure the glottic-area waveform (GAW), a plot of the glottic area against the time of opening and closing of the glottis during a representative vibratory cycle (taken from the stroboscopic image). From this information, glottal opening and closing rates are calculated. These measurements are purported to be correlates of vocal-fold pliability and differ statistically in preoperative and postoperative states for benign vocal-fold lesions. [10, 11]
An admitted limitation of the stroboscopic image is that vocal-fold vibration must be relatively periodic to visualize a slow-motion representation of the phonatory cycle. Efforts to extend the sensitivity of laryngoscopy to incorporate variations of wave characteristic across the glottis and in aperiodic patterns of vibration have yielded new techniques. [12]
The limitations that stroboscopy has in only being able to reveal a highly averaged composite view of vocal fold vibratory behavior during relatively periodic phonation is overcome by high speed imaging. [12] Systems for doing laryngeal high speed digital videoendoscopic recordings have been available for about a decade, but these have been limited, until recently, to black-and-white imaging at rates that were only adequate for relatively low-pitched phonation (2000 images per second). Recent advances in digital high-speed video (HSV) camera technology have resulted in clinical systems that can produce color images at higher rates (4000 images per second).
Even though HSV provides much more detailed information about vocal fold phonatory function than stroboscopy, its eventual adoption into standard clinical practice will depend on the extent to which remaining practical, technical, and methodological, challenges can be met. Such challenges include the relatively high cost of HSV systems, management of the large computer files that HSV recordings produce, limitations on the sampling of vocal behaviors obtained during the brief durations of HSV recordings, and a paucity of solid clinical research demonstrating that HSV significantly improves the diagnosis and management of voice disorders [13] (ie, controlled clinical trials).
-
Standard 70 degree rigid strobolaryngoscope.
-
Distal chip flexible laryngostroboscope.
-
Camera attachment with mounted microphone.
-
Laryngeal microphone.
-
Depiction of rigid strobolaryngoscopy.
-
Rigid strobolaryngoscopy.
-
Mallampati classification.
-
This patient was evaluated for hoarseness. Stroboscopy shows the mucosal wave only with patient effort. Video courtesy of Vijay Ramakrishnan, MD.





