Practice Essentials
The term sulcus vocalis is used specifically to describe a groove or infolding of mucosa along the surface of the vocal fold. In the area of the sulcus, the mucosa is scarred down to the underlying vocal ligament, giving it a retracted appearance.
Essentially, no differences exist between vocal fold scarring where an identifiable sulcus is present and scarring where an identifiable sulcus is not present. In either case, an alteration in the normal physiology of vocal fold vibration exists, which affects voice production. Therefore, this chapter will focus on vocal fold scarring and its effect on vocal physiology.
Most clinicians agree that presentation of sulcus vocalis is hoarseness, vocal fatigue, voice weakness, and increased effort. However, clinicians may disagree on terminology, diagnosis, and treatment of this disorder. Certainly, widespread acceptance of videostroboscopy has allowed more clinicians to recognize the disorder. This has spurred new interest in its diagnosis and treatment.
Workup in sulcus vocalis
In sulcus vocalis, videostroboscopy reveals an area of decreased mucosal wave corresponding to the sulcus and more clearly shows associated incomplete closure.
Other diagnostic studies commonly employed by the laryngologist include the following:
-
Acoustic analysis - Reveals some information about vocal production efficiency and voice strength
-
Airflow measurements - Useful in gauging vocal support and glottic constriction
Management of sulcus vocalis
Medical therapy
Prior to considering surgical therapy, all known sources of mechanical trauma are maximally reduced to determine the reversibility of sulcus vocalis and hopefully prevent a postoperative recurrence. This is accomplished in part by medical and speech therapy, which are aimed at decreasing vocal trauma through improved phonatory technique and vocal hygiene. When voice therapy is combined with external measures (eg, amplification) and behavioral alterations (eg, scheduling vocal rest periods), vocal fatigue may dissipate.
Surgical therapy
When low volume and loss of projection are major complaints in sulcus vocalis, medialization of the scarred vocal fold may significantly improve vocal performance while decreasing effort and fatigue. [1]
Medialization alone, however, may not significantly impact vocal quality. An attempt to reconstitute the lamina propria may be considered for patients who have adequate volume but poor vocal quality. [2]
Current opinion holds that placing a biocompatible material between the vocal ligament and cover or within the layers of the lamina propria could compensate for lost tissue and restore the sliding movement of the mucosal cover. This additional layer also may prevent fibroblast migration from deeper layers and further scar formation.
History of the Procedure
Patients may experience hoarseness but more often have symptoms of glottal insufficiency, including fatigue, poor volume, and poor projection. However, the voice may be normal with more subtle symptoms (eg, fatigue, decreased vocal range with singing).
Problem
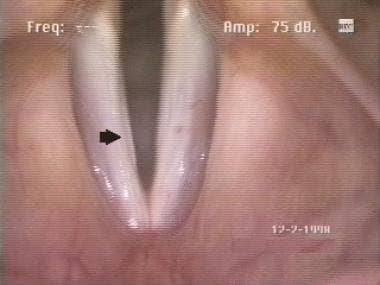
The term sulcus vocalis is used to describe a depression or groove in the surface of vocal fold mucosa that is typically found on the leading edge of the vibratory surface. Along the sulcus, the mucosal cover is scarred down to the underlying vocal ligament and therefore is tethered. A linear sulcus, nearly the length of the true vocal fold, can be seen in the image below.
A mucosal bridge is a variation on the simple sulcus and is formed when 2 parallel sulci simultaneously appear on the medial and superior surface of the true vocal fold. This creates an area of normal-appearing mucosa between 2 mucosal defects. These lesions are more difficult to treat than single sulci but fortunately are very rare.
Epidemiology
Frequency
The incidence of sulcus vocalis is impossible to determine due to variation in presentation and diagnosis. Most sulci are undiagnosed because of subclinical symptoms, lack of clinician awareness, and difficulty in identification due to limited availability of laryngeal videostroboscopy. In a study of autopsy specimens by Nakayama et al, sulci were identified in 20% of specimens. [3, 4]
Etiology
Sulcus vocalis may be congenital or secondary to vocal trauma, infection, degeneration of benign lesions, or surgery. [5] In addition, Bouchayer et al proposed a relationship with ruptured congenital epidermoid cysts and also suggested that the disorder may demonstrate familial patterns. [6] Typically, patients with congenital sulci have a lifelong history of disordered voice.
Presence of parallel sulci associated with a mucosal bridge is consistent with ruptured cyst etiology. Surgical causes include overresection of the superficial layer of the lamina propria, resulting in remucosalization over the deficient area and damage to the vocal ligament and deep layers of the lamina propria. Nonsurgical causes include untreated benign lesions, chronic vocal abuse, and repeated intracordal hemorrhage. Microvascular lesions (ie, varices, capillary ectasias) also may result in scarring secondary to hemorrhage and fibrosis.
A retrospective study by Lee et al indicated that epithelial pathology plays a significant role in sulcus vocalis, with the prevalence of parakeratosis, dyskeratosis, and epithelial thickening found to be particularly high in sulcus vocalis. The investigators suggested that epithelial changes cause perilesional inflammation, which in turn produces clinical changes. [7]
Pathophysiology
A defect in the medial surface of the true vocal fold along the sulcus may produce a glottic gap. More importantly, the cover may fibrose to the vocal ligament and result in a diminished or absent vocal mucosal wave. This decreased pliability restricts the Bernoulli and myoelastic effects, whereby transglottic airflow medializes the leading edge of the vocal fold. The overall effect is usually a higher fundamental frequency with significantly reduced harmonics and harsher voice quality.
Presentation
Patients experience hoarseness and often have symptoms and signs of glottal insufficiency, including poor volume, poor projection, and vocal fatigue. On initial interview, the voice may be hoarse and breathy or acceptable, but most patients have an overall decrease in vocal performance.
Examination of the true vocal fold reveals a linear depression or an area of incomplete closure. Videostroboscopy reveals an area of decreased mucosal wave corresponding to the sulcus and more clearly demonstrates the associated incomplete closure.
Relevant Anatomy
Awareness of the body-cover principle of vocal fold vibration is essential to the understanding of sulcus vocalis. The vocal fold is composed of a muscle covered by a free mucosal edge that vibrates and can be separated into discrete layers in which various types of pathology may develop. Each layer has distinct mechanical properties and can be differentiated by the concentration of elastin and collagen fibers that run parallel to the leading edge.
Histologically, the vocal fold is a complex structure. The delicate arrangement of extracellular matrix proteins within the lamina propria permits passive movement of the vocal cover over the vocal ligament and muscle, or body. This results in formation of the mucosal wave as air is passed through the glottis as a release of building subglottic pressure. Violation of deeper layers of the lamina propria and vocal ligament, as was once common with stripping procedures, is now known to be associated with scar and sulcus formation.
-
Linear sulcus nearly the length of the true vocal fold.
-
Sulcus under normal light indirect laryngoscopy: Note the very subtle appearance.
-
Sulcus under stroboscopy: Note the defect in the vibratory surface caused by the sulcus.





