Practice Essentials
The activities of swallowing and speaking depend upon the ability to obtain adequate closure of the velopharyngeal port. Both are complex motor skills that involve the coordination of a diverse group of muscles along the upper aerodigestive tract. Velopharyngeal movements during phonation are quite distinct from those involved in swallowing, as is clinically evident in patients who are able to obtain good closure during swallowing yet are unable to obtain adequate closure when speaking.
Phonation involves the generation of a column of air pressure passing from the subglottis into the upper airway. Inadequate velopharyngeal closure (VPC) allows air to escape through the nose during the generation of consonants requiring high oral pressure, leading to inappropriate nasal resonance during speech production. Pharyngeal closure patterns are shown below.
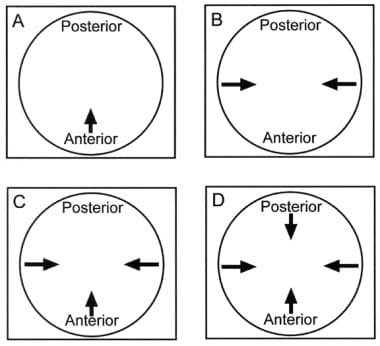 Pharyngeal closure patterns important in velopharyngeal insufficiency. (A) Coronal. (B) Sagittal. (C) Circular. (D) Circular with the Passavant ridge.
Pharyngeal closure patterns important in velopharyngeal insufficiency. (A) Coronal. (B) Sagittal. (C) Circular. (D) Circular with the Passavant ridge.
Causes of hypernasality and velopharyngeal dysfunction (VPD) are many and range from structural causes (eg, cleft palate) to neuromuscular problems (eg, those observed in velocardiofacial [VCF] syndrome). Functional etiologies also exist, including splinting of the palate after tonsillectomy, imitation of cultural or familial role models, and phoneme-specific problems.
Workup in velopharyngeal insufficiency
Voice and resonance evaluation includes the following:
-
Articulation assessment
-
Oral motor assessment
-
Measurement of nasal airflow
Other tests include cephalometry, fiberoptic nasoendoscopy, and videofluoroscopy (VF).
Management of velopharyngeal insufficiency
Conservative management
Speech therapy improves velopharyngeal function when VPD is minimal or due to articulation errors and in postoperative patients. Compensatory articulation techniques secondary to VPD also can be corrected with speech therapy. However, in patients with a specific anatomic deficiency that precludes adequate closure of the velopharynx, speech therapy cannot replace surgery.
Continuous positive airway pressure (CPAP) therapy is beneficial for patients whose VPD seems related to oral motor issues or velar weakness rather than structural problems of the velum. CPAP therapy is a palate-strengthening program using CPAP equipment, including a nasal mask, that is carried out 6 days per week for 8 weeks in the patient's home.
Prosthetic devices are helpful when surgery is contraindicated or the cause of velopharyngeal insufficiency (VPI) is neuromuscular in nature or as a temporizing measure until surgery can be performed.
Surgery
The primary indications for surgical intervention include a structural defect of the velum or a functional problem that results in poor or inconsistent velar closure. Surgical procedures include the following:
-
Pharyngoplasty - The goal of pharyngoplasty is to develop a more functional sphincter by improving the dynamics and bulk of the velopharyngeal tissues and by tightening and reducing the size of the velopharyngeal opening
-
Pharyngeal flap - This procedure aims to develop a central flap of tissue to obturate the midline of the pharyngeal port and decrease the degree of air escape into the nasal cavity
-
Posterior wall augmentation - This approach is appropriate in the presence of a persistent gap in the central velopharyngeal port measuring at most 1-3 mm; it also is indicated when the patient can achieve touch closure that is not tight enough to prevent air escape with high oral pressure; persistent postadenoidectomy VPI is also an appropriate indication for this procedure
Problem
Velopharyngeal closure (VPC) is an important part of speech. All phonemes in the English language with the exception of 3 (/m/, /n/, /ng/) are produced with oral airflow, meaning that the velopharynx should be closed. The nasal phonemes (/m/, /n/, /ng/) are produced with nasal resonance, requiring that the velopharynx be open during their production. With so many phonemes in English requiring oral airflow, oral resonance is important to production of intelligible speech.
In describing the problem of hypernasal speech, differentiation between velopharyngeal mislearning, velopharyngeal incompetency, and velopharyngeal insufficiency (VPI) is important. Velopharyngeal mislearning is best described as incorrect closure of the velopharyngeal port in the nasopharynx as a result of articulation difficulties. Velopharyngeal incompetency is inadequate VPC secondary to a functional problem due to oral motor difficulties (eg, paresis, apraxia, dysarthria).
VPI, in contrast, is inadequate closure of the velopharyngeal port resulting from a structural problem with the velum (eg, submucous cleft palate, shorted velum relative to the depth of the posterior pharyngeal wall, overt cleft palate). The effect of velopharyngeal incompetency or VPI on the patient's speech is usually the same; therefore, these 2 terms typically are used interchangeably or best referred to in general as velopharyngeal dysfunction (VPD).
Etiology
When describing etiologies of velopharyngeal dysfunction (VPD), categories of classification include structural abnormalities of the palate, dynamic impairment of a structurally normal palate, and functional abnormalities unassociated with anatomic or dynamic palatal defects. An overview of common etiologies follows.
Overt cleft palate, either before or after repair, is by far the most common cause of VPD. This condition occurs in approximately 1 of 2000 live births. VPD has been reported in as many as 30-50% of patients following palate repair. A retrospective cohort study by Smyth and Wu found that of 271 nonsyndromic infants who underwent a cleft palate repair involving levator veli palatini muscle repositioning with or without lateral palatal release, fistulae occurred in 28 patients (10.3%) followed up at age 5 years. The investigators also found that the existence of fistulae led to a three-fold increase in VPI, with the VPI rate rising from 18% to 54%. The rate reached 71% when fistulae complicated bilateral cleft lip and palate repair. [1]
A submucous cleft palate is defined by the presence of a bifid or double uvula, muscular diastasis of the soft palate (zona pellucida), and notching of the posterior border of the hard palate. This is usually evident on examination of the oral cavity, especially with elevation of the palate when pronouncing the phoneme /ah/.
By contrast, an occult submucosal cleft palate is an absence or deficiency of the musculus uvulae with a diastasis of the levator veli palatini but without the presence of a bifid uvula or grooving of the oral surface of the soft palate. An occult submucous cleft is best visualized endoscopically as midline notch on the nasal surface of the soft palate during palate elevation.
Most patients with either overt or occult submucous cleft palate can produce normal speech. However, because of their abnormal musculature, these patients may be predisposed to VPD from any changes to the velopharyngeal anatomy, such as adenoidectomy.
Transient VPD with hypernasal resonance following adenoidectomy, with or without tonsillectomy, is not uncommon. This condition may persist for several days to weeks and usually resolves spontaneously. Some nasal regurgitation of liquids may be present during this period. Incidence of persistent VPD after adenoidectomy has been reported to range from 1 per 1,500 to 1 per 10,000 patients. While the adenoid pad is not necessary for normal VPC, it may assist in closure in children with structural or functional abnormalities of the soft palate. Children at risk of developing persistent VPD after adenoidectomy often can be identified preoperatively by presence of repaired cleft palate, submucous cleft palate, palatopharyngeal disproportion (ie, abnormally deep pharynx), or palatal hypotonia.
A predisposition to VPD is also present in patients with trisomy 21 (ie, Down syndrome). The combination of oromotor and developmental delays, generalized hypotonia, and intellectual delays constitute significant risk factors for development of VPD following adenoidectomy. Because patients with trisomy 21 often have a narrow velopharynx and a shallower skull base, resulting in less distance for the palate to traverse to effect closure, this risk is somewhat balanced.
Velocardiofacial syndrome (VCF) is an autosomal dominant entity linked to microdeletions in the long arm of chromosome 22. Major findings include cleft palate (overt, submucous, or occult submucous), conotruncal heart anomalies, mental disabilities, and a characteristic facies. VPD is common in patients with VCF syndrome due to the presence of a cleft palate and pharyngeal hypotonia.
Another syndrome in which VPD is a common feature is Kabuki syndrome (KS). Many findings of KS are similar to those of VCF syndrome, including cleft palate, cardiac abnormalities (typically coarctation of the aorta), muscular hypotonia, and characteristic facial features. As with VCF syndrome, poor muscular tone of the velopharynx is a major cause of VPD in patients with KS.
Velopharyngeal incompetency or VPI also may be a feature of other syndromes (eg, neurofibromatosis, myotonic dystrophy, or any syndrome in which low muscle tone is a feature).
VPD may be caused by tonsil hypertrophy that prevents the palate from adequately moving superiorly during attempted velopharyngeal closure. Tonsillectomy may be appropriate in these patients.
Acquired VPD may present in persons affected by stroke or head injury, especially if damage occurs to motor centers controlling cranial nerves responsible for pharyngeal muscle control. Other neurologic diseases (eg, muscular dystrophy, multiple sclerosis, amyotrophic lateral sclerosis [ALS], Parkinson disease) also may lead to VPD in the more advanced stages of disease. Articulation problems and VPD are especially common in patients undergoing pallidotomy for severe Parkinson disease.
Pathophysiology
Oral resonance (as contrasted to nasal resonance) is obtained by velopharyngeal closure (VPC), a seal between the nasopharynx and the oral cavity. Typically VPC is accomplished by elevation of the velum and approximation of the lateral walls to close off the nasopharynx. In a small group of patients, formation of a Passavant ridge on the posterior pharyngeal wall may contribute to closure. Velopharyngeal dysfunction (VPD) describes what happens when velopharyngeal closure is impaired.
Effects of VPD on a patient's speech include: hypernasality; decreased speech intelligibility; and nasal emissions (ie, air escape out of the nose during speech). How severely a patient's speech is affected depends on several factors, including the following: the amount of gap with a closed velum; the patient's articulation and oral motor ability; and compensatory strategies the patient may have developed to decrease nasal emission or hypernasality.
Common compensatory strategies include: speaking with soft intensity (ie, volume) to decrease airflow through the nasal cavity; speaking with loud intensity or pushing to try to project the voice; and substituting phonemes that require less airflow for the correct phoneme.
Presentation
Historical factors in velopharyngeal dysfunction (VPD) are related primarily to problems with speech intelligibility. The voice is described as having a nasal resonance, and nasal emissions (ie, air escape through the nasal passage with speech) also may be present. Often, compensatory articulation errors are present, worsening speech intelligibility. Hoarseness also commonly is observed in children with VPD due to vocal strain to overcome nasal escape.
Nasal regurgitation, especially in infants, may be a precursor to VPD. Parents may describe a history of food and liquids coming through the nose with feeding and spitting up. In older children and adults, recurrent and chronic sinus infections may be a sign of nasopharyngeal reflux and repeated contamination of the nasal cavity. Persistent otorrhea with ear grommets in place also may be due to nasopharyngeal reflux extending up the Eustachian tube and through the middle ear. A history of recurrent ear infections or persistent middle ear effusions may also be an indicator of poor palatal function.
When eliciting a history from patients with VPD, looking for other factors that may lead to diagnosis of a congenital syndrome is important. Poor feeding and hypotonia in infancy may suggest the presence of a neuromuscular disorder. Congenital heart defects in association with VPD are common features of both velocardiofacial syndrome (VCF) and Kabuki syndrome (KS). A family history may reveal other affected individuals, also pointing to a genetic etiology.
Relevant Anatomy
Six muscles comprise the velopharyngeal sphincter, as follows:
-
Tensor veli palatini: This muscle arises from the scaphoid fossa, spine of the sphenoid, and the cartilaginous portion of the eustachian tube. It inserts into a tendon winding around the hamular process. Innervated by the mandibular branch of cranial nerve (CN) V, it tenses the soft palate and opens the eustachian tube during swallowing.
-
Levator veli palatini: This muscle arises from the petrous apex and cartilaginous portion of the eustachian tube. Its fibers fan out in the soft palate and blend with the contralateral levator. Innervated by the pharyngeal plexus from CN IX and X, it pulls the velum in a posterosuperior direction and serves as the major elevator for the velum.
-
Musculus uvulae: This muscle arises from the palatal aponeurosis posterior to the hard palate and inserts into the uvula mucosa. Innervated by the pharyngeal plexus, it functions to add bulk to the dorsal aspect of the uvula.
-
Palatoglossus: The palatoglossus arises from the anterior surface of the soft palate and inserts into the lateral aspect of the tongue base. Innervated by the pharyngeal plexus, it simultaneously lowers the velum and elevates the tongue upwards and backwards.
-
Palatopharyngeus: The palatopharyngeus arises from the soft palate and inserts into the posterior border of the thyroid cartilage. Innervated by the pharyngeal plexus, it positions the velum and narrows the velopharyngeal orifice by adducting the posterior pillars and constricting the pharyngeal isthmus. This muscle also raises the larynx and lowers the pharynx.
-
Superior constrictor: This muscle arises from the lower portion of the pterygoid plate and the hamular process and inserts into the median raphe. Innervated by the pharyngeal plexus, it produces medial movement of the pharyngeal walls and assists in drawing the velum posteriorly.
When viewed endoscopically, several topical anatomic features of the velopharynx (nasopharynx) are important to note.
-
Pharyngeal ostium of the eustachian (auditory) tube: This opening and its associated structures comprise the lateral wall of the nasopharynx. The ostium is bordered anteriorly by the salpingopalatine fold and posteriorly by the cartilaginous torus tubarius. Posterior to the torus tubarius is the pharyngeal recess. Extending inferiorly from the torus tubarius is the salpingopharyngeal fold, which overlies the salpingopharyngeal muscle. Inferior to the ostium and torus, the pterygopharyngeal portion of the superior pharyngeal constrictor muscle comprises the lateral wall of the nasopharynx.
-
Pharyngeal tonsil (ie, adenoid): The adenoid, which is a closely aggregated collection of lymphoid nodules, is directly posterior in the nasopharynx and overlies the basilar portions of the sphenoid and occipital bones. The adenoid lies directly between the torus tubarius on either side and may extend laterally into the pharyngeal recess, where it is commonly known as the eustachian or Gerlach tonsil. Superiorly, the adenoid may extend up into the nasal choanae, and inferiorly, it ends at or near the level of the anterior arch of the atlas. The prevertebral fascia and the atlanto-occipital membrane lie deep to the pharyngeal tonsil.
-
Posterior pharyngeal wall: Immediately inferior to the pharyngeal tonsil, the posterior pharyngeal wall comprises mainly the superior pharyngeal constrictor muscle. Contraction of this muscle in the axial plane at the level of VPC constitutes a structure known as the Passavant ridge.
-
Pharyngeal surface of the soft palate: This structure is formed by the aponeuroses of several muscles including the superior pharyngeal constrictor muscle, levator veli palatini muscle, salpingopharyngeus muscle, palatopharyngeus muscle, and uvular muscle. The insertion and innervation of these muscles is described above.
Contraindications
One factor to consider in preoperative planning is whether breathing is obstructed preoperatively. Placement of a pharyngeal flap increases the degree of nasal airway obstruction and may worsen any preexisting obstructive sleep apnea. This is especially true in patients with Pierre Robin syndrome, in which retrognathia may result in upper airway obstruction. In such instances, consideration should be given to pharyngoplasty instead of pharyngeal flap, since the risk of worsening airway obstruction postoperatively is lessened with pharyngoplasty.
The location of the internal carotid arteries as they traverse the lateral pharynx is also an important consideration, especially in patients with velocardiofacial syndrome (VCF). In patients with VCF, the internal carotid artery can take a more medial position, with a theoretical risk of injury to the ICA during pharyngeal surgery. Preoperative evaluation with contrast-enhanced CT scan or magnetic resonance angiography can elucidate the course of the ICA. In practice, the ICA will lateralize when the head is extended for surgery and will not be in the operative field during pharyngoplasty or pharyngeal flap surgery, and the presence of a medially displaced ICA is not necessarily a surgical contraindication.
The presence of a primary bleeding disorder (ie, hemophilia or von Willebrand disease) may complicate surgical management. Likewise, anticoagulation for reasons such as a prosthetic heart valve may be a contraindication to surgery.
-
Pharyngeal closure patterns important in velopharyngeal insufficiency. (A) Coronal. (B) Sagittal. (C) Circular. (D) Circular with the Passavant ridge.
-
Coronal closure.
-
Sagittal closure.
-
Circular closure.
-
Circular closure with Passavant's ridge.
-
Patient with severe articulation disorder and velocardiofacial syndrome. Little or no velar closure is noted on nasopharyngoscopy, known as a "black hole." Surgical treatment is with a wide pharyngeal flap. Aberrant carotid arteries coursing through the nasopharynx complicate surgical management.
-
Infant born with heart murmur, submucous cleft palate, and lower lip asymmetry. Clinical findings are consistent with velocardiofacial syndrome.
-
Preschool child with hypernasal speech due to poor velar closure. Genetic findings demonstrated microdeletions of the 22q11.2 region.





