Background
The transnasal-sublabial approach to the pituitary has undergone an evolutionary refinement and today remains probably the most commonly used approach to selected pituitary tumors. The following article describes the history, technique, and complications of this useful surgical approach.
History of the Procedure
The evolution of the transnasal-transseptal approach to the pituitary traces its lineage and subsequent reintroduction to sequential developments in rhinosurgical and neurosurgical techniques.
In 1909, Hirsch combined the septal-submucous resection (as reported by Killian and Hajek's sphenoid sinusectomy) into a submucosal-septal approach to the sphenoid. [1] Halstead first described using a gingivolabial incision to approach the septum, incorporating the upper lip and nose as a composite flap. [2] In 1914, Cushing combined the gingivolabial incision and submucous resection as an approach to the pituitary. [3] However, Cushing eventually abandoned the transseptal procedure, citing the high risk of intracranial contamination that likely results from direct contamination by the nasal vault.
In Paris, Guiot reported success using the transseptal approach, following the influence of Cushing's pupil, Dott. [4, 5] Hardy subsequently reintroduced the transseptal procedure to North America. [6] Combined with the advent of antibiotics, the use of intravenous steroids, and the technological advancements in the use of the operating microscope, the transseptal approach to the pituitary remains the most popular approach today.
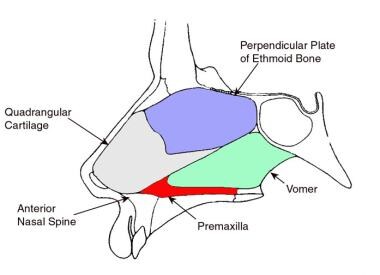
The normal median sagittal nasal anatomy is shown in the image below.
Indications
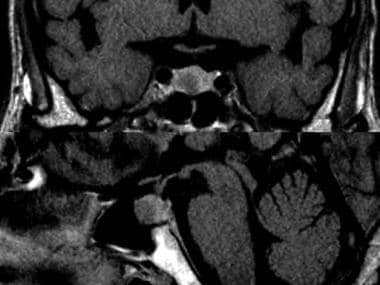
Pituitary adenoma (as seen in the image below)
Relevant Anatomy
Embryology, development, and surrounding anatomy of the sphenoid sinus
The sphenoid sinus begins as an evagination of the sphenoethmoidal recess during the fourth month of fetal life. Following the third year of life, the sinus begins to excavate into the pneumatizing sphenoid bone. This process progresses in the child from age 5-7 years. The adult size is not reached until age 18 years.
The extent of pneumatization by the sinus into the sphenoid bone varies greatly. The capacity of the sinus varies from 0.5-30 mL. Hamberger in 1961 [7] and Congdon in 1930 [8] classified 3 differing types of sella pneumatization, and each is conceptualized by the position in relation to the sella turcica. The presellar type (23%) has its posterior wall in contact with the anterior face of the sella. The sellar or postsellar type (67%) appears when the sinus extends posteriorly beyond the sella to the pons. The conchal type (5%) is similar to the presellar type, except that the most posterior part of the sinus is well anterior to the sella turcica.
The paired sphenoid sinuses rarely are symmetrical in size and have an intersinus septum that may be near horizontal in its orientation. This position renders the 2 sinuses in an over and under orientation, rather than in a lateral orientation. Important central nervous system, neurologic, and vascular structures surround the sphenoid sinus. Superiorly, the middle cranial fossa and the pituitary gland are in approximation to the sinus, while anterosuperiorly, the optic nerve and chiasm lie over the sinus. Anteriorly, a lateral margin of the sphenoid bone forms a portion of the posterior orbital wall, and the anterior sphenoid forms a crest that articulates with the perpendicular plate of the ethmoid bone.
The sphenoid ostia are located above the superior turbinate at approximately one-half the length from the anteroinferior-most border of the sinus. The ostia drain into the posterior aspect of the sphenoethmoidal recess. Laterally, the carotid artery may indent the sinus wall posteroinferiorly or even lie within the sinus, directly contacting the sinus mucosa. Likewise, the contents of the cavernous sinus, including the oculomotor, trochlear, and abducens nerves and the ophthalmic and maxillary branches of the trigeminal nerve, contact the lateral wall of the sinus. Inferiorly, the roof of the nasopharynx and the neurovascular anatomy of the pterygoid canal are found. The inferior surface forms the sphenoid rostrum and articulates with the vomer bone. Posteriorly, through the thick bony wall, the pons and basilar artery are located.
Contraindications
Contraindications to the transseptal-sublabial approach to the pituitary include the following:
-
Ongoing sinusitis that is untreated by either surgery and/or medical therapy
-
Highly vascular lesions
-
Dural-based lesions with a high risk for intraoperative and postoperative cerebrospinal fluid leak
-
Lesions with extensive suprasellar extension and carotid artery anatomy, wherein the arteries project into the sphenoid sinus and limit safe access
-
Coronal and median sagittal images of pituitary adenoma.
-
Normal median sagittal nasal anatomy.
-
Normal coronal nasal anatomy.
-
Elevation of septal mucoperichondrial-periosteal flap.
-
Coronal view of septal mucoperichondrial flap elevation.
-
Elevation of discontinuous septal mucoperichondrial and nasal floor mucoperiosteal flaps.
-
Continuous septal mucoperiosteal and nasal floor mucoperiosteal flaps.
-
Continuous septal and nasal flaps and contralateral nasal floor flap.
-
Transection of septal cartilage, vomer, and ethmoid bones.
-
Gingivolabial incision.
-
Insertion of speculum through gingivolabial incision.
-
Placement of speculum after removal of septal cartilage and bone.
-
Incision through nasal floor.
-
Medialization of nasal floor flap.





