Practice Essentials
Fractures of the mandibular body may be classified by anatomic location, condition and position of teeth relative to the fracture, favorableness, or type.
Body fractures occur between the distal aspect of the canines and a hypothetical line corresponding to the anterior attachment of the masseter. These fractures are proximal to the third molar.
Mandible fractures are also described by the relationship between the direction of the fracture line and the effect of muscle distraction on fracture fragments. Mandible fractures are favorable when muscles tend to draw bony fragments together and unfavorable when bony fragments are displaced by muscle forces. Vertically unfavorable fractures allow distraction of fracture segments in a horizontal direction. These fractures tend to occur in the body or in symphysis-parasymphysis areas. Horizontally unfavorable fractures allow displacement of segments in the vertical plane. Evidence demonstrates that there is no need to apply different treatment modalities to mandibular fractures regardless of whether the factures are favorable. [1, 2]
Body fractures often are unfavorable because of the actions of the masseter, temporalis, and medial pterygoid muscles, which distract the proximal segment superomedially. Additionally, the mylohyoid muscle and anterior belly of the digastric muscle may contribute to the unfavorable nature of this fracture by displacing the fractured segment posteriorly and inferiorly.
The image below depicts the vertical and horizontal forces acting on the mandible, as well as the relationship of muscle pull to fracture angulation.
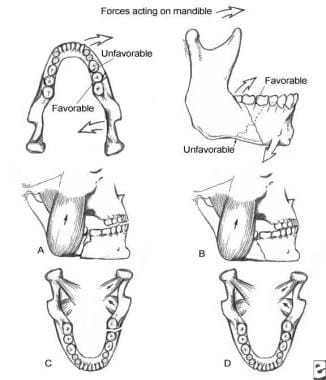 Forces acting on the mandible and demonstration of the relationship between muscle pulls and fracture angulation. (A) Horizontally unfavorable. (B) Horizontally favorable. (C) Vertically unfavorable. (D) Vertically favorable.
Forces acting on the mandible and demonstration of the relationship between muscle pulls and fracture angulation. (A) Horizontally unfavorable. (B) Horizontally favorable. (C) Vertically unfavorable. (D) Vertically favorable.
Signs and symptoms of mandibular body fractures
Anesthesia, paresthesia, or dysesthesia of the lower lip may be evident.
A body fracture may cause the lateral aspect of the face to appear flattened. Loss of the mandibular body on palpation may be due to an unfavorable fracture. The anterior face may be displaced forward, causing elongation. Damage to the condylar growth center can cause retarded growth of the mandible and facial asymmetry in children.
Lacerations may provide diagnostic evidence of the type of fracture sustained. Hematoma and ecchymosis may alert the clinician to a mandibular fracture.
Workup in mandibular body fractures
The single most informative radiologic study used in mandibular fracture diagnosis is panoramic radiography.
However, computed tomography (CT) scanning and plain radiography using lateral-oblique, posteroanterior, occlusal, and periapical views may also be helpful.
Management of mandibular body fractures
Medical therapy
Patients with isolated nondisplaced or minimally displaced condylar fractures may be treated with analgesics, soft diet, and close observation. Patients with coronoid process fractures may be treated similarly. Additionally, these patients may require mandibular exercises to prevent trismus. If the fractured coronoid restricts mandible movement, medical therapy is contraindicated. Use prophylactic antibiotics for compound fractures. Penicillin remains the antibiotic of choice.
Surgical therapy
Mandibular fractures can be managed through closed reduction and fixation or by way of open reduction and internal fixation.
The intraoral approach may be used in fractures with no or only slight dislocation. The extraoral approach is necessary with fractures that have a high degree of dislocation or comminution, because placing longer and stronger plates is difficult via the intraoral approach. The extraoral approach is also undertaken with fractures lying between the inferior and lingual aspects of the body.
The following techniques for rigid fixation of the mandible have been developed:
-
The bicortical Luhr system, using vitallium plates
-
The Arbeitsgemeinschaft für Osteosynthesefragen/Association for the Study of Internal Fixation (AO/ASIF) system of stainless steel compression or reconstruction plates with bicortical screws [3]
-
The Champy miniplate technique placed along the "line of ideal osteosynthesis," using monocortical screws
Epidemiology
Frequency
In general, mandible fractures of the body, condyle, and angle have nearly the same incidence, while fractures of the ramus and coronoid process are rare. The literature suggests the following mean frequency percentages based on location: body (29%), condyle (26%), angle (25%), symphysis (17%), ramus (4%), and coronoid process (1%).
The mandible is involved in 70% of patients with facial fractures.
The number of mandible fractures per patient ranges from 1.5-1.8. Approximately 50% of patients with a mandible fracture have more than 1 fracture.
The multicenter, prospective European Maxillofacial Trauma (EURMAT) project found mandibular fractures, particularly condylar and body fractures, to be the most prevalent maxillofacial fractures in children. The study, which included 114 children aged 15 years or younger, reported 47 mandibular fractures, including 18 condylar fractures and 12 body fractures. [4]
A retrospective US study of pediatric mandibular fractures by Siwani et al found that among all types of mandibular fractures, including body fractures, patients most frequently incurred injury through motor vehicle accidents (52 patients, 43%), sports (24 patients, 20%), and assault (13 patients, 11%). The study, which involved 122 patients (216 mandibular fractures), all of whom were aged 18 years or younger, found that 11 patients (9%) had a history of attention deficit hyperactivity disorder (ADHD), 23 (19%) had a history of a non-ADHD mental disorder, 17 (14%) had asthma, 18 (15%) used tobacco, 13 (11%) used alcohol, and 11 (9%) used marijuana. The investigators suggested that the relatively high proportion of mental disorders and substance abuse found in this report could have treatment implications in pediatric mandibular fractures. [5]
Etiology
Vehicular accidents and assaults are the primary causes of mandibular fractures worldwide. The mandible fracture patterns of a suburban trauma center found that violent crimes such as assault and gunshot wounds accounted for the majority of fractures (50%), while motor vehicle accidents were less likely (29%).
Data from industrialized nations suggest that fractures have various causes, as follows:
-
Vehicular accidents - 43%
-
Assaults - 34%
-
Work-related causes - 7%
-
Falls - 7%
-
Sporting accidents - 4%
-
Miscellaneous causes - 5%
Assault most often causes mandible angle fractures.
Pathophysiology
Optimal mandible function requires maintenance of normal anatomic shape and stiffness (ie, resistance to deformation under load). Normal occlusion can be defined when the mesiolabial cusp of the maxillary first molar approximates the buccal groove of the mandibular first molar. Fractures result secondary to mechanical overload. Torque results in spiral fractures, avulsion in transverse fractures, bending in short oblique fractures, and compression in impaction and higher comminution. A fracture in which one cortex of the bone is broken while the other cortex is bent is termed a greenstick fracture.
Degree of fragmentation depends upon energy stored as a result of overload prior to the fracturing process. Therefore, wedge and multifragmentary fractures are associated with high-energy release.
An evidence-based study involving 3002 patients with mandibular fractures found that the presence of a lower third molar may double the risk of an angle fracture of the mandible. [6]
Presentation
History
Obtain a thorough history specific to preexisting systemic bone disease, neoplasia, arthritis, collagen vascular disorders, and temporomandibular joint (TMJ) dysfunction. Knowledge of the type and direction of the causative traumatic force helps determine the nature of injury. For example, motor vehicle accidents (MVAs) have a larger associated magnitude of force than assaults. As a result, a patient who has experienced an MVA most often sustains multiple, compound, comminuted mandibular fractures, whereas a patient hit by a fist may sustain a single, simple, nondisplaced fracture.
Knowing the direction of force and the object associated with the fracture also assists the clinician in diagnosing additional fractures.
Physical
Pertinent physical findings are limited to the injury site.
Change in occlusion may be evident on physical examination. Any change in occlusion is highly suggestive of mandibular fracture. Ask the patient how his or her bite feels.
Posttraumatic premature posterior dental contact (anterior open bite) and retrognathic occlusion may result from an angle fracture. Unilateral open bite is associated with a unilateral angle fracture.
Anesthesia, paresthesia, or dysesthesia of the lower lip may be evident. Most nondisplaced mandible fractures are not associated with changes in lower lip sensation; however, displaced fractures distal to the mandibular foramen (in the distribution of the inferior alveolar nerve) may exhibit these findings.
Change in facial contour or loss of external mandibular form may indicate mandibular fracture. A body fracture may cause the lateral aspect of the face to appear flattened. Loss of the mandibular body on palpation may be due to an unfavorable fracture. The anterior face may be displaced forward, causing elongation. In this case, the anterior mandible is displaced downward. Damage to the condylar growth center can cause retarded growth of the mandible and facial asymmetry in children.
Lacerations, hematoma, and ecchymosis are associated with mandibular fractures. Lacerations may provide diagnostic evidence of the type of fracture sustained. Hematoma and ecchymosis may alert the clinician to a mandibular fracture. Do not close facial lacerations before treating underlying fractures. Ecchymosis in the floor of the mouth is a diagnostic sign of a mandibular body or symphysis fracture.
Pain, swelling, redness, and localized heat are signs of inflammation evident in primary trauma.
Indications
Use the simplest means possible to reduce and fixate a mandibular fracture. Because open reduction carries an increased morbidity risk, use closed techniques whenever possible. Indications for closed reduction include (1) nondisplaced favorable fractures, (2) grossly comminuted fractures, (3) edentulous fractures (using a mandibular prosthesis), (4) fractures in children with developing dentition, and (5) coronoid and condylar fractures.
Indications for open reduction include (1) displaced unfavorable angle, body, or parasymphyseal fractures, (2) multiple facial fractures, (3) bilateral displaced condylar fractures, and (4) fractures of an edentulous mandible (with severe displacement of fracture fragments in an effort to reestablish mandible continuity).
Relevant Anatomy
The body or horizontal ramus of the mandible usually includes the third molar and is bounded anatomically from the distal symphysis to a line coinciding with the alveolar border of the masseter muscle.
Contraindications
Evaluate and monitor patients' general physical conditions prior to treating mandibular fractures.
Any force capable of causing a mandibular fracture also may injure other organ systems. Case reports have documented concurrent posttraumatic thrombotic occlusion of the internal carotid artery and basilar skull fractures.
Bilateral cervical subcutaneous emphysema, pneumothorax, pneumomediastinum, and spleen lacerations also have been associated with mandible fractures after trauma.
Patients should not undergo surgical reduction of mandible fractures until these issues are addressed.
-
A mandible body fracture with displacement. (A) Transverse fracture of the right mandible. (B) Fixation achieved using miniplates at the superior and inferior borders. (C) Postoperative radiograph demonstrating fixation.
-
Forces acting on the mandible and demonstration of the relationship between muscle pulls and fracture angulation. (A) Horizontally unfavorable. (B) Horizontally favorable. (C) Vertically unfavorable. (D) Vertically favorable.
-
(A) An oblique fracture of the body fixed with 1 lag screw, in combination with a compression plate at the inferior border and a dental splint for tension. (B) A fracture of the mandible body with a basal triangle. (C) Open reduction and adequate fixation using a miniplate at the superior border and a reconstruction plate at the inferior border. (D) Postoperative radiograph demonstrating fixation. An open hole in the reconstruction plate lies between the triangle and the corpus.









