Overview
The skull base forms the floor of the cranial cavity and separates the brain from other facial structures. This anatomic region is complex and poses surgical challenges for otolaryngologists and neurosurgeons alike. Working knowledge of the normal and variant anatomy of the skull base is essential for effective surgical treatment of disease in this area.
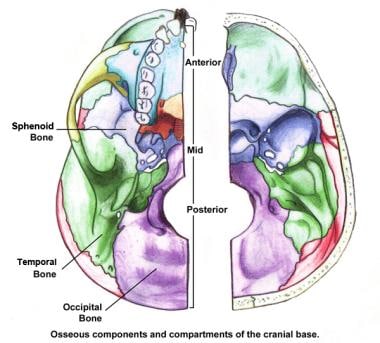
The 5 bones that make up the skull base are the ethmoid, sphenoid, occipital, paired frontal, and paired temporal bones. The skull base can be subdivided into 3 regions: the anterior, middle, and posterior cranial fossae. (See the image below.) The petro-occipital fissure subdivides the middle cranial fossa into 1 central component and 2 lateral components. This article discusses each region, with attention to the surrounding structures, nerves, vascular supply, and clinically relevant surgical landmarks. [1, 2, 3, 4, 5, 6, 7, 8, 9]
Anterior Skull Base
Boundaries
The anterior limit of the anterior skull base is the posterior wall of the frontal sinus. The anterior clinoid processes and the planum sphenoidale, which forms the roof of the sphenoid sinus, mark the posterior limit. The frontal bone forms the lateral boundaries. The frontal bone houses the supraorbital foramina, which, along with the frontal sinuses, form 2 important surgical landmarks during approaches involving the anterior skull base. (See the image below.)
The greater portion of the anterior floor is convex and grooved by the frontal lobe gyri. This portion of the skull base consists of the orbital portion of the frontal bone. The ethmoid bone forms the central part of the floor, which is the deepest area of the anterior cranial fossa. In the center of this region is the cribriform plate, through which the olfactory tracts pass. The fovea ethmoidalis, or the roof of the ethmoid cavity, continues laterally from the cribriform plate. The cribriform plate may be more than 1 cm lower than the roof of the ethmoid cavity (fovea ethmoidalis), and it is made of extremely thin bone compared with the relatively thick bone of the lateral fovea ethmoidalis. During transethmoidal approaches to the anterior skull base, this relationship is extremely important to remember.
The foramen cecum sits between the frontal crest and the prominent crista galli and is a site of communication between the draining veins of the nasal cavity and the superior sagittal sinus. The crista galli, which projects up centrally between the cerebral hemispheres, serves as the site of attachment for the falx cerebri.
The optic chiasm, or chiasmatic sulcus, sits slightly posteriorly in the midline. The anterior clinoid processes form the posterolateral segment and help form the roof of the optic canal. In the medial aspect, the lesser wing of the sphenoid forms the anterior clinoid process, an important landmark for the optic nerve and supracavernous internal carotid artery (ICA).
Inferior relationships — extracranial aspects
The most important anatomic structures below the anterior cranial fossa are the orbits and the paranasal sinuses. A thorough description is beyond the scope of this article, but important anatomy and relationships are discussed.
The bony orbit is often a route for intracranial and extracranial spread of infection and tumors because of its direct proximity to the anterior fossa. The posterior wall is thin and adjacent to the superior sagittal sinus and frontal lobe dura. The posterior aspect includes the optic canal, the superior orbital fissure (SOF), and the inferior orbital fissure (IOF). The SOF conveys the oculomotor, trochlear, abducens, and ophthalmic nerves (cranial nerves [CN] III, IV, VI, and V1, respectively), as well as the ophthalmic veins.
The IOF transmits the maxillary nerve (CN V2) and infraorbital vessels, and it communicates with the infratemporal and pterygomaxillary fossae. The lateral portion of the IOF is an important surgical landmark for positioning lateral orbital osteotomies during anterior skull base resections. The optic canal transmits the optic nerve (CN II) and the ophthalmic artery.
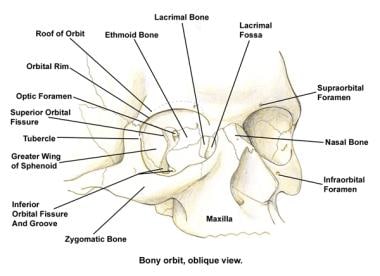
The image below demonstrates the relationship of the openings described above. The medial wall is closest to the apex and is formed by the orbital process of the frontal, lacrimal, ethmoid, and sphenoid bones. The medial wall transmits the anterior and posterior ethmoid arteries through their respective foramina. These foramina help in identifying the frontoethmoid suture line, which marks the inferior extent of the anterior cranial fossa. The posterior ethmoid artery foramen is also an important surgical marker for the location of the optic canal and nerve, which lies about 0.5 cm posterior to it.
The lesser wings of the sphenoid and the frontal process of the maxilla form the lateral walls. The posteriormost segment of the lateral orbital wall forms the anterior wall of the middle cranial fossa and is discussed in greater detail in the next section.
The ethmoid sinuses can be found inferior to the anterior cranial fossa and medial to the orbits. The frontal sinuses arise as evaginations of ethmoid air cells into the frontal bone and have a thick anterior and thinner posterior wall. The posterior wall is adjacent to the superior sagittal sinus and the frontal lobe dura. As a result, the frontal sinus can be used as a route of surgical entry into the anterior cranial fossa. Infectious processes and tumors can exploit this relationship as well, to gain intracranial access.
Contents
The dura mater attaches anteriorly at the frontal crest and crista galli to form the falx cerebri, which transmits the superior and inferior sagittal sinuses. The superior sagittal sinus drains the superior cerebral and frontal diploic veins of Breschet. These veins form a potential pathway for infection to spread intracranially, causing complications such as sagittal sinus thrombosis, empyema, and abscess.
The foramen cecum, found anterior to the crista galli, usually ends blindly, though it may transmit a vein from the nasal mucosa to the superior sagittal sinus. Its patency may lead to the formation of developmental anomalies, such as nasal dermoid cysts, nasal gliomas, encephaloceles, and meningoencephaloceles. [10]
The frontal lobes occupy the anterior fossa and sit superior to the orbits and sinonasal tract. The major structures in this area are the olfactory bulb and tract. The olfactory bulb lies along the medial edge of the frontal orbital plate and connects with the olfactory tract, which courses above the cribriform plate and planum sphenoidale.
Middle Skull Base
Boundaries — intracranial aspects
The greater wing of the sphenoid helps form the anterior limit of the middle skull base. The posterior limit is the clivus, which is formed from the sphenoid and occipital bones. The greater wing of the sphenoid forms the lateral limit as it extends laterally and upward from the sphenoid body to meet the squamous portion of the temporal bone and the anteroinferior portion of the parietal bone. The greater wing of the sphenoid forms the anterior floor of the fossa. The anterior aspect of the petrous temporal bone forms the posterior floor of the middle cranial fossa.
The body of the sphenoid makes up the central portion of the middle fossa and houses the sella turcica. The sella turcica can be found between the anterior and posterior clinoid processes and is composed of 3 sections. The tuberculum sellae is an olive-shaped swelling and sits on the anterior slope between the chiasmal sulcus and the sella turcica. The hypophyseal or pituitary fossa lies immediately posterior to the tuberculum sellae. The dorsum sellae is the furthest posterior. In this region lies the sigmoid groove for the ICA as it traverses the petrous apex through the cavernous sinus.
The floor and the lateral walls are grooved for the middle meningeal artery, which courses anterolaterally from the foramen spinosum and which divides into frontal and parietal branches. The former ascends across to the pterion, where it courses posteriorly. The pterion is an H -shaped suture, where the frontal bone, the greater wing of the sphenoid bone, the squamous temporal bone, and the parietal bone meet. This suture is approximately 3.5 cm behind the zygomaticofrontal suture and 4 cm above the zygomatic arch.
The pterion is made up of thin bone and can be easily fractured during trauma. If fractured, it can result in injury to the anterior branches of the middle meningeal artery, with eventual formation of an epidural hematoma.
The petrous portion of the temporal bone forms the posteromedial limit of the middle cranial fossa. The superior petrosal sinus creates a longitudinal groove in the petrous ridge. The anteromedial petrous tip houses the trigeminal or gasserian ganglion in a region known as Meckel cave. This area is superior to the point at which the ICA enters the cavernous sinus just above the foramen lacerum. Along the superomedial surface of the petrous temporal bone, the roof of the carotid canal is frequently dehiscent, a feature that makes dural elevation risky.
The arcuate eminence is the superior extent of the superior semicircular canal. It can be appreciated on the superior aspect of the midpetrous ridge. The eminence is an important landmark during the middle fossa approach for localization of the internal auditory canal (IAC). Lateral to the arcuate eminence, the thin tegmen tympani and tegmen mastoideum cover the middle ear and mastoid, respectively. The tegmen is a thin plate of bone that separates the dura of the middle lobe from the middle ear and the mastoid cavity. The bone of the floor of the middle fossa may be dehiscent over the geniculate ganglion of the facial nerve.
Foramina — intracranial aspects
The SOF, foramen rotundum, foramen ovale, and foramen spinosum lie in an anteroposterior and mediolateral plane. (See the image below.) Beginning lateral to the clinoid process anteriorly, the SOF extends inferomedially and toward the orbital apex and transmits the oculomotor nerve (CN III); the trochlear nerve (CN IV); the lacrimal, frontal, and nasociliary branches of CN V1; and the abducens nerve (CN VI). It also transmits the superior ophthalmic vein.
The foramen rotundum lies posteroinferior to the base of the SOF, at the level of the sella turcica. It transmits the maxillary division (CN V2) of the trigeminal nerve into the pterygopalatine fossa. The foramen sits near the lateral wall of the sphenoid sinus. The foramen ovale is posterior and lateral and transmits the mandibular division (CN V3) of the trigeminal nerve, the accessory meningeal artery, the lesser superficial petrosal nerve (LSPN), and emissary veins to the pterygoid plexus into the infratemporal fossa.
The foramen spinosum lies further posterolaterally and transmits the middle meningeal artery, as well as the meningeal branch of the facial nerve (CN VII).
The carotid canal forms where the petrous apex articulates with the sphenoid and occipital bone. It continues into the foramen lacerum on the undersurface of the skull base. The jagged foramen lacerum lies posteromedial to the foramen ovale. Two inconsistent foramina are the innominate foramen, which may be found medial to the foramen spinosum, and the foramen of Vesalius, found medial to foramen ovale. The foramen of Vesalius is found in 40% of individuals and transmits an emissary vein, which drains the cavernous sinus.
Of note, the petro-occipital fissure, a gap between the medial border of the petrous temporal bone and the lateral border of the clivus, is an important radiographic and preoperative surgical landmark, because it lies in close proximity to various middle cranial fossa foramina. It also serves to anatomically divide the middle skull base into a central compartment and 2 lateral compartments.
Contents
Important structures in the middle fossa include but, are not limited to, the temporal lobe, the pituitary gland, the trigeminal or gasserian ganglion, the greater superficial petrosal nerve (GSPN), the intracranial portion of the ICA, and the cavernous sinus and its contents. In the middle fossa, the dura strongly adheres to the clinoid processes, the petrous and sphenoid ridges, and the basal foramina. In the midline, it forms the diaphragma sellae—a circular dural plate—which covers the pituitary gland. The pituitary stalk or infundibulum and the hypophyseal veins perforate this structure. The cavernous sinus resides on both sides of the sella turcica and the body of the sphenoid bone.
The temporal lobe takes up most of the space of the middle fossa and extends to the inferior portion of the anterior fossa. The GSPN branches from the geniculate ganglion and passes through a small hiatus into the middle fossa before coursing parallel to the petrous ridge of the temporal bone and entering the foramen lacerum. The GSPN, which is composed of parasympathetic fibers from the facial nerve to the lacrimal gland, is an important surgical landmark. It is easily identified and can be followed back medially to the foramen lacerum and the petrous ICA.
The GSPN and rostral LSPN run along the floor beneath the dura and parallel the anterior edge of the petrous bone into foramen lacerum. Here, the GSPN joins with the deep petrosal nerve to form the vidian nerve or the nerve of the pterygoid canal. This area is also a landmark for the ICA, which lies deep and parallel to the temporal bone and medial to the styloid process.
The facial nerve (CN VII) and vestibulocochlear nerve (CN VIII) originate from the caudal pons. They course through the subarachnoid space and enter the porus acusticus and IAC. CN VII continues through the temporal bone, the middle ear, and the mastoid bone to exit at the stylomastoid foramen and innervate the facial nerve musculature. The eustachian tube originates at the protympanum and runs anteromedially and inferiorly. The bone directly medial to the eustachian tube may be dehiscent, and the ICA may be seen. This feature is clinically relevant during surgical exploration of the middle fossa, because the eustachian tube must be traversed before the ICA is reached in this area.
Cavernous sinus
The cavernous sinus is a complex plexus of veins in the dura that can be found lateral to the sphenoid sinus. It extends from the SOF to the apex of the petrous temporal bone. The anterior and posterior petroclinoid folds serve as the lateral borders. Along the lateral wall runs the ICA, which gives off 2-6 caroticocavernous branches that supply the hypophysis and that join branches from the middle meningeal artery.
Running lateral to the ICA, the abducens nerve (CN VI) enters the dura superior to the clivus and enters the Dorello canal. Infection of the petrous apex classically manifests as abducens palsy due to inflammation in the Dorello canal. The petroclinoid and petrosphenoidal ligaments of Gruber form the roof of the canal; the roof lies in close proximity to the trigeminal ganglion and within 3 mm of the sphenoid sinus.
Running superoinferiorly in the lateral wall are the oculomotor nerve (CN III), the trochlear nerve (CN IV), the ophthalmic nerve (CN V1), and the maxillary nerve (CN V2). The oculomotor nerve divides into superior and inferior divisions at the most anterior portion of the cavernous sinus. The trochlear nerve enters at the angle between the anterior and posterior petroclinoid folds and courses the lateral wall.
The 3 divisions of the trigeminal nerve traverse inferior to the tentorium cerebelli into the Meckel cave, within the subarachnoid space. From here, V1, V2, and V3 pass into the lateral wall of the cavernous sinus.
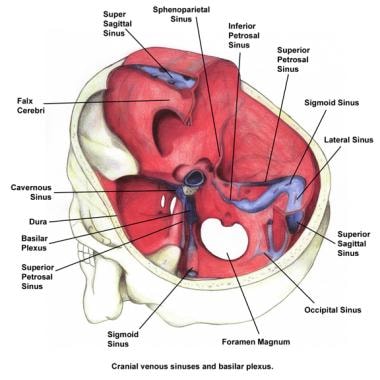
The cavernous sinus has complex venous drainage. It connects anteriorly to the superior ophthalmic vein and the sphenoparietal sinus and drains posteriorly into the superior and inferior petrosal sinuses en route to the basilar plexus. The superior and inferior petrosal sinuses emerge from the posterior aspect of the cavernous sinus and eventually drain into the sigmoid sinus and the internal jugular vein. The superficial, middle, and inferior cerebral veins drain into the cavernous sinus from above, and the emissary veins drain into the pterygoid plexus below the sinus. Interruption of the anastomotic branch of the superficial middle cerebral vein as it connects to the transverse sinus is likely to cause an infarction.
Knowledge of these complex relationships is necessary for recognizing the manifestations of carotid-cavernous fistulas, which are reported to occur with basilar skull fractures. In the case of such fistulas, traumatic tears of the intracavernous carotid result in high-pressure arterial blood flooding the cavernous sinus. Clinically significant backflow in the low-pressure superior ophthalmic veins draining into the cavernous sinus leads to venous engorgement, proptosis, and chemosis. In severe cases, pulsating exophthalmos can be observed.
In rare cases, infections may enter the skull base from the facial venous system and travel retrograde through the valveless ophthalmic veins into the anterior portion of the cavernous sinus. The result is cavernous sinus thrombosis. Pimples and pustules, which occur in the medial canthal, nasal, and labial areas (danger zone of the face), may pass through the valveless angular and facial veins and drain superiorly into the ophthalmic veins. They may eventually seed the cavernous sinus. Dental infections may spread into the cavernous sinus by means of the pterygoid plexus.
Internal carotid artery
The course of the ICA is complex, and landmarks must be recognized during skull base surgery. The course can be divided into 4 parts: cervical, intratemporal, cavernous, and supracavernous.
The cervical portion passes near the third and fourth cervical vertebrae. At this point, it is deep to the posterior digastric muscle and styloid process and superior and posteromedial to the external carotid artery. The cervical ICA can be distinguished from the external carotid because it has no branches. This feature is clinically important, because the relationship with the external carotid may be aberrant. The ICA enters the petrous bone through the carotid foramen and runs cranially into the foramen lacerum.
The intratemporal segment is difficult to mobilize because of an adherent fibrous ring. This vertical portion ascends 5 mm and turns anteromedially into the horizontal portion. At this point, it is medial to the eustachian tube and anterolateral and inferior to the cochlea. At times, the carotid artery can be dehiscent in this area and extend into the middle ear cleft. In these cases, the artery is at great risk during surgery involving the middle ear. A dehiscent or aberrant ICA can appear as a pinkish or white-blue mass filling the inferior portion of the middle ear. A pulsatile tympanic membrane is sometimes observed. (See the image below.)
In the normal case, the temporal carotid artery runs forward along the petrous bone at a 45° angle to the midsagittal plane, giving off the caroticotympanic and pterygoid branches. At this point, the artery is superior and lateral to the sphenoid bone in an area referred to as the carotid siphon. The artery then enters the cavernous sinus medial to the abducens nerve (CN VI).
On traversing the roof of the cavernous sinus medial to the anterior clinoid process, the ICA enters the supracavernous portion. The last segment turns backward under the optic nerve to the anterior perforated substance, where it joins the circle of Willis through its terminal anterior and middle cerebral arteries.
Lateral relationships — extracranial aspects
As previously discussed, the petro-occipital fissure divides the middle cranial fossae into central and lateral components.
Boundaries — extracranial aspects
The anterior boundary of the middle cranial fossa is the posterolateral wall of the maxillary sinuses; the petro-occipital sutures form its posterior boundary. The lateral margin consists of primarily the squamous and petrous portions of the temporal bone.
Many surgical approaches in the lateral skull base involve the infratemporal fossa. Working knowledge of this area is imperative for the surgeon. The anterior boundary of the infratemporal fossa is the posterior wall of the maxillary sinus. The posteroinferior boundary is the parapharyngeal space. The lateral pterygoid plate forms the medial boundary, whereas the mandibular ramus and condyle create the lateral boundary. Finally, the greater wing of the sphenoid bone forms the superior border of the infratemporal fossa.
Contents — extracranial aspects
When viewed from the extracranial lateral aspect, the infratemporal fossa lies below the temporal bone, inferomedial to the zygomatic arch, and posterior to the maxilla. Structures first identified in the infratemporal fossa include the muscles of mastication, namely, the temporalis, masseter, and medial and lateral pterygoid muscles. The internal maxillary artery, one of the terminal branches of the external carotid artery, provides blood to these muscles and should be preserved in case a temporalis flap is necessary to reconstruct skull base defects. (See the image below.)
The medial and lateral pterygoid muscles take up most of the space of the infratemporal fossa. Dissecting further in a medial direction reveals the cartilaginous eustachian tube and the tensor and levator veli palatini muscles.
Moving anteriorly past the pterygoid process, one finds the pterygomaxillary fissure, which transmits the maxillary artery to the pterygomaxillary fossa. (See the image below.) The greater petrosal nerve joins the deep petrosal nerve to form the vidian nerve, which enters the fossa through the vidian or pterygoid canal en route to the pterygopalatine ganglion. The maxillary nerve enters through the foramen rotundum and branches thereafter to supply sensory information from regions of the face. Both nerves send branches to the parasympathetic sphenopalatine ganglion. The IOF is at the most anterior limit of the pterygomaxillary fossa and is continuous with the infratemporal fossa.
Two important bony surgical landmarks may be identified in the infratemporal fossa. The first is the root of the lateral pterygoid plate. This plate serves as a marker for the foramen rotundum, which lies immediately anterior to it, as well as for the foramen ovale, which lies immediately posterior. Once the foramen ovale is identified, the foramen spinosum is easily identifiable immediately posterior to the foramen. The second landmark is the sphenoid spine, which helps in identifying the highest portion of the cervical ICA and the carotid canal. The sphenoid spine is just medial to the condylar or glenoid fossa and posterolateral to the foramen spinosum.
Drainage of the external lateral skull base involves the internal and external jugular venous system and the retromandibular vein. The mastoid and occipital emissary veins can link the intracranial dural sinus system with the external circulation, namely, with branches of the occipital, postauricular, or retrofacial veins. The pterygoid venous system can be highly variable in this region.
The facial, superficial temporal, and occipital and postauricular branches of the external carotid artery provide arterial supply to the lateral skull base. The internal maxillary artery, with its deep temporal and middle meningeal branches, can be identified in the infratemporal fossa as well. The cervical portion of the ICA ascends vertically to enter the middle fossa medial to the sphenoid spine.
The deep lobe of the parotid gland and the accompanying facial nerve (CN VII) and its branches may be encountered in the lateral aspect of the extracranial skull base.
The facial nerve exits the mastoid through the stylomastoid foramen and enters the substance of the parotid gland. Before exiting, the postauricular branch of the facial nerve branches off and gives rise to the occipital, auricular, digastric, and stylohyoid branches, as well as to a communicating branch that joins the glossopharyngeal nerve. The chorda tympani nerve arises from the temporal segment of the facial nerve and eventually joins the lingual nerve to supply taste to the anterior two thirds of the tongue.
The jugular foramen, which transports CNs IX, X, and XI, is a large, bony gap between the jugular process of the occipital bone and the jugular process of the petrous bone. In the extracranial aspect, its anterior border is the carotid canal, its lateral border is the styloid process sheath, and its medial borders are the hypoglossal foramen and canal. It lies posterolaterally in the lateral skull base and anteromedially to the mastoid tip. The jugular foramen can be divided into the pars nervosa anteriorly and the pars venosa posteriorly. Intracranial details of the jugular foramen are discussed in the Posterior Skull Base section.
Medial relationships
The sphenoid sinus can serve as an access route to the pituitary and the clivus. Sellar pneumatization of the sinus facilitates entry during transsphenoidal approaches. It is important to avoid disrupting the lateral wall during instrumentation, because the ICA and optic nerve are just lateral to a thin margin of bone. Dehiscence may be present in the lateral wall of the sphenoid, resulting in exposure of the carotid artery, optic nerve, or vidian nerve.
The nasopharynx lies posterior and inferior to the sphenoid sinus along the midline. Mucosa covers the medial surface of the medial pterygoid plate. Along with the investing pharyngobasilar fascia and the superior pharyngeal constrictor muscle, it helps to form the lateral portion of the choana and part of the lateral portion of the nasopharynx.
The sinus of Morgagni is a weak point in the superolateral nasopharyngeal wall. It is created by the passage of the levator veli palatini and the cartilaginous eustachian tube through the superior constrictor muscle. This is a region for infections or tumor to potentially invade the skull base. Directly superior to the nasopharynx is the foramen lacerum and the ICA, just before its entry point into the cavernous sinus.
The investing fascia of the nasopharynx, also known as the pharyngobasilar fascia, is suspended from the skull base and clivus, located superiorly. The vertebrobasilar artery and the brainstem lie posterior to the clivus.
Posterior Skull Base
Boundaries
The posterior skull base consists of primarily the occipital bone, with contributions from the sphenoid and temporal bones. The basal portion of the occipital bone (the basiocciput) and the basisphenoid form the anterior portion of the posterior skull base. These 2 regions combine to form the midline clivus.
The posterior surface of the petrous temporal bone and the lateral aspect of the occipital bone form the lateral wall. The occipital bone also fuses with the mastoid portion of the temporal bone to form the occipitomastoid suture. The petrous portion of the temporal bone and the greater wings of the sphenoid bone are particularly important for identifying structures. The overlying tentorium cerebelli separates the cerebellum from the cerebral hemispheres above, whereas the occipital bone forms the lateral walls and floor.
The floor is grooved for the cerebellar hemispheres, and the midline internal occipital crest runs from the foramen magnum to the internal occipital protuberance. The crest serves as an attachment for the falx cerebelli, which contains the occipital sinus. Grooves for the superior sagittal sinus are superior to the internal occipital protuberance. The horizontal grooves for the paired transverse sinuses can be found lateral to the internal occipital protuberance. They descend to the mastoid angle of the parietal bone to become continuous with the sigmoid sulcus. (See the image below.)
The sigmoid sulcus can be found in the lateral aspect of the posterior cranial fossa in the mastoid portion of the temporal bone. It ends at the jugular foramen. The sulcus for the inferior petrosal sinus sits posterior to the clivus and anterior to the petrous apex.
Foramina
The porus acusticus is the opening of the IAC. Found on the posterior surface of the petrous bone, it transmits the CNs VII and VIII, the nervus intermedius, and the labyrinthine vessels (branches of the anterior inferior cerebellar artery en route to the inner ear). The vestibular aqueduct is posteroinferior to the IAC. It transmits the endolymphatic duct.
The jugular foramen extends laterally from the posterior aspect of the occipital condyle. It is formed by the anterior processus jugularis of the petrous bone and the occipital bone in its posterior aspect, and it lies at the posterior end of the petro-occipital fissure. The sigmoid sinus and the jugular bulb enter the foramen at its smooth posterior end (pars venosa). CN's IX, X, and XI enter its rough anterior end (pars nervosa). The inferior petrosal sinus usually enters this portion of the jugular foramen between CNs IX and X, but its path is highly variable. It may even enter the internal jugular vein below the skull base.
Finally, the ascending pharyngeal artery may send a posterior meningeal branch through the jugular foramen. The jugular tubercle may be medial to the lower aspect of the jugular foramen, and it serves as a landmark for the hypoglossal foramen.
The hypoglossal foramen is inferomedial to the jugular foramen and near the jugular tubercle. It transmits the hypoglossal nerve (CN XII), a meningeal branch of the ascending pharyngeal artery, and the hypoglossal venous plexus. Emissary veins in connection with the sigmoid sinus may leave the posterior fossa through mastoid foramina.
The brainstem communicates with the vertebral canal through the foramen magnum. The structures that pass through are the medulla oblongata, the spinal accessory nerve, the vertebral and posterior spinal arteries, and the apical ligament of the dens and membrane tectoria.
Contents
The midbrain, the pons, the medulla, and the cerebral and cerebellar hemispheres lie in the posterior fossa. Dura and the tentorium cerebelli enclose the various aforementioned venous sinuses. CN's VII-XII exit through the posterior fossa. CN's VII and VIII and the nervus intermedius exit through the porus acusticus, and nerves IX, X, and XI traverse the jugular foramen. CN XII exits through the hypoglossal canal. [8]
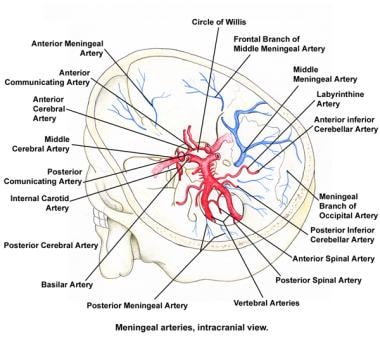
On entering the posterior fossa through the foramen magnum, the vertebral arteries ascend ventral to the roots of CNs IX, X, and XI. The posterior inferior cerebellar arteries usually branch off from the vertebral arteries before forming the midline basilar artery at the base of the pons. The basilar artery then branches into the anterior inferior cerebellar arteries, which travel to the cerebellopontine angle in close relationship to CN's VII and VIII. The basilar artery then branches into the labyrinthine artery, numerous long and short pontine arteries, and, finally, the superior cerebellar arteries, which make up the posterior portion of the circle of Willis. (See the image below.)
Inferior relationships — extracranial aspects
A surgeon must have knowledge of the outer regions of the skull base, because these regions often serve as access points during surgery.
Suboccipital region
The mastoid tip serves as the origin for the sternocleidomastoid, while the posterior digastric muscle originates deep to this area. In the posterior aspect, the trapezius muscle is most superficial. Immediately deep lies the splenius capitis and cervicis muscles and the semispinalis capitis muscle. On reflection of these muscles from the superior nuchal line, the suboccipital triangle is exposed. (See the image below.)
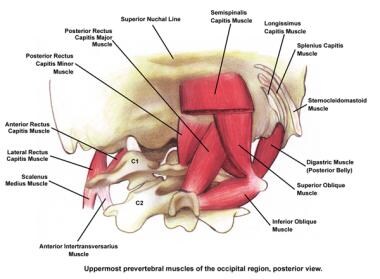
The suboccipital triangle is superficial to the ligaments connecting the atlas to the axis and contains the occipital artery, the vertebral artery, a complex of veins, the greater occipital nerve, and the C1 nerve. The occipital artery courses posteriorly deep to the mastoid tip. Surgical approaches in this area allow mobilization of the vertebral artery and access to the foramen magnum.
Vertebral artery
The vertebral artery originates from the subclavian artery and has 4 parts: cervical, foraminal, atlantic, and subarachnoid. The atlantic portion is encountered in the suboccipital triangle of the nuchal region and is covered by the semispinalis capitis muscle.
The atlantic portion exits the atlas at the transverse foramen medial to the lateral rectus capitis muscle and curves posteriorly behind the lateral mass of the atlas. It then passes medially along the groove on the posterior arch of the atlas and pierces the atlantooccipital membrane to enter the vertebral canal and subarachnoid space. The subarachnoid portion of the artery is considered to lie in the posterior cranial fossa proper.
-
Osseous components and compartments of the cranial base.
-
Bony orbit, oblique view.
-
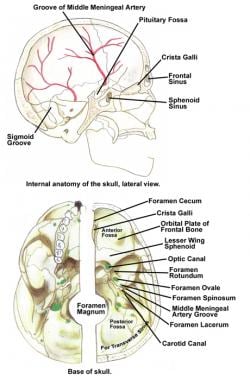
Internal anatomy of the skull base, lateral view, and base of the skull.
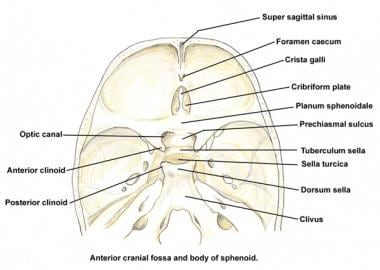
-
Anterior cranial fossa and body of the sphenoid.
-
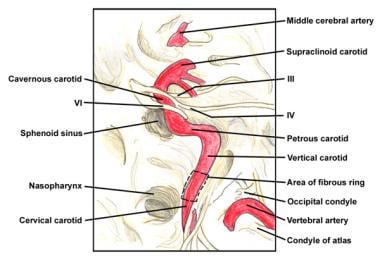
Intracranial course of the internal carotid artery.
-
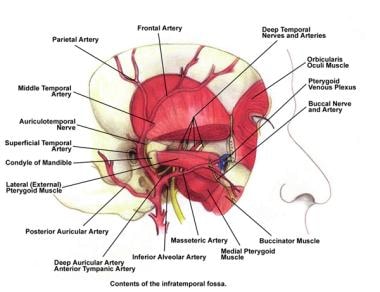
Contents of the infratemporal fossa.
-
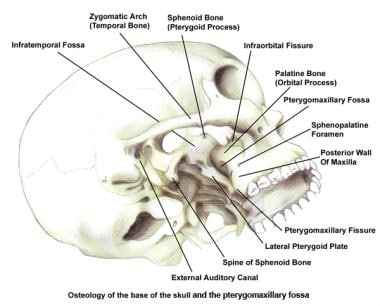
Osteology of the base of the skull and the pterygomaxillary fossa.
-
Cranial venous sinuses and the basilar plexus.
-
Meningeal arteries, intracranial view.
-
Uppermost prevertebral muscles of the occipital region, posterior view.