Practice Essentials
The term presbycusis refers to age-related, sensorineural hearing impairment in elderly individuals. [1] A complex condition, presbycusis arises from multiple factors that, over a number of years, result in progressive and symmetrical hearing loss. Characteristically, presbycusis involves bilateral high-frequency hearing loss associated with difficulty in speech discrimination and central auditory processing of information. However, other patterns of presbycusis exist. The association between advanced age and high-tone deafness was first described by Zwaardemaker in 1899. Since then, extensive research has attempted to determine the pathologic changes of presbycusis, but the exact mechanisms remain unknown. [2] Audiometric testing with pure-tone average and speech discrimination forms the cornerstone of diagnostic testing for presbycusis. Properly fitted hearing aids may contribute to the rehabilitation of a patient with presbycusis.
Presbycusis is an important problem in society. It occurs in an elderly population that relies on special senses to compensate for other age-associated disabilities. Elderly individuals may rely on their hearing to overcome limitations of impaired vision and slowed reaction time. In addition, age-associated decline in concentration and memory contribute to difficulty understanding speech, especially in noisy situations. Arthritis and impaired dexterity may limit their ability to take advantage of the amplification devices used in rehabilitation of age-associated hearing loss. Finally, hearing loss may contribute to the isolation of some elderly people by restricting their use of the phone, causing them to forfeit social opportunities such as concerts and social gatherings and amplifying their sense of disability.
The inner ear is a complex, fluid-filled structure within the dense area of the temporal bone called the otic capsule. The cochlea and vestibular system of the inner ear are the organs of hearing and balance, respectively. The cochlea has three fluid-filled compartments: the scala vestibuli, the scala media, and the scala tympani. Fluid (or endolymph) for the scala media arises from the stria vascularis, a group of blood vessels. Inner hair cells sense pressure changes in this fluid and transmit neural signals to the brain by the vestibulocochlear (eighth) cranial nerve. An image depicting the inner ear can be seen below.
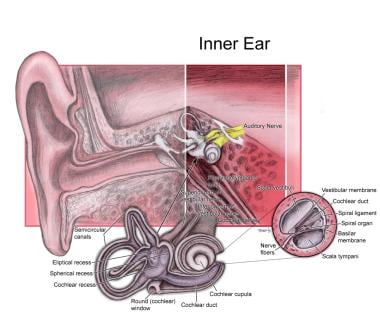 Inner ear.
Inner ear.
Signs and symptoms of presbycusis
Patients typically may have more difficulty understanding rapidly spoken language, vocabulary that is less familiar or more complex, and speech within a noisy, distracting environment. Patients may often complain that they have more difficulty understanding women than men, given the higher pitch at which women speak. In addition, localizing sound is increasingly difficult as the disease progresses. Patients with presbycusis may rely strongly on lip reading to improve intelligibility of spoken words. [3]
Workup in presbycusis
Audiometric testing with pure-tone average and speech discrimination forms the cornerstone of diagnostic testing for presbycusis. Evaluation can also include blood tests for autoimmune-induced hearing loss and computed tomography (CT) scanning or magnetic resonance imaging (MRI) to exclude anatomic abnormalities or mass lesions that may affect hearing.
Tests of central auditory processing may be employed to exclude abnormal processing of auditory information in the central nervous system.
Management of presbycusis
Presbycusis is not curable, but the effects of the disease on patients’ lives can be mitigated. The following treatments and strategies may be employed:
-
Amplification devices
-
Lip reading
-
Assistive listening devices
-
Cochlear implants
Pathophysiology
Histologic changes associated with aging occur throughout the auditory system from the hair cells of the cochlea to the auditory cortex in the temporal lobe of the brain. These changes may correlate with different clinical findings and auditory test results, depending on the severity of the changes and the anatomic level at which they occur. Over the past 50 years some brilliant research in the field of presbycusis has been witnessed, but elucidation of the pathophysiology of presbycusis is still incomplete.
Many researchers have investigated the causes of this disease. Crowe and associates, Saxen, and Gacek and Schuknecht have studied histologic changes in the cochleae of human ears with presbycusis. Gacek and Schuknecht identified 4 sites of aging in the cochlea and divided presbycusis into 4 types based on these sites. [4] The histologic changes are correlated approximately with symptoms and auditory test results.
-
Sensory presbycusis: This refers to epithelial atrophy with loss of sensory hair cells and supporting cells in the organ of Corti. This process originates in the basal turn of the cochlea and slowly progresses toward the apex. These changes correlate with a precipitous drop in the high-frequency thresholds, which begins after middle age. The abrupt downward slope of the audiogram begins above the speech frequencies; therefore, speech discrimination is often preserved. Histologically, the atrophy may be limited to only the first few millimeters of the basal end of the cochlea. The process is slowly progressive over time. One theory proposes that these changes are due to the accumulation of lipofuscin pigment granules.
-
Neural presbycusis: This refers to atrophy of nerve cells in the cochlea and central neural pathways. Schuknecht estimated that 2100 neurons are lost every decade (of 35,000 total). This loss begins early in life and may be genetically predetermined. Effects are not noticeable until old age because pure-tone average is not affected until 90% of neurons are gone. Atrophy occurs throughout the cochlea, with the basilar region only slightly more predisposed than the remainder of the cochlea. Therefore, no precipitous drop in the high-frequency thresholds on audio is observed. A disproportionately severe decrease in speech discrimination is a clinical correlate of neural presbycusis and may be observed before hearing loss is noted because fewer neurons are required to maintain speech thresholds than speech discrimination.
-
Metabolic (ie, strial) presbycusis: This condition results from atrophy of the stria vascularis. The stria vascularis normally maintains the chemical and bioelectric balance and metabolic health of the cochlea. Atrophy of the stria vascularis results in hearing loss represented by a flat hearing curve because the entire cochlea is affected or a low-frequency hearing deficit. Speech discrimination is preserved. This process tends to occur in people aged 30-60 years. It progresses slowly and may be familial.
-
Mechanical (ie, cochlear conductive) presbycusis: This condition results from thickening and secondary stiffening of the basilar membrane of the cochlea. The thickening is more severe in the basal turn of the cochlea where the basilar membrane is narrow. This correlates with a gradually sloping high-frequency sensorineural hearing loss that is slowly progressive. Speech discrimination is average for the given pure-tone average.
The changes associated with presbycusis are rarely found exclusively at one site; the development of presbycusis typically involves simultaneous changes at multiple sites. A histologic study of temporal bones from patients with typical presbycusis found the degree of hearing loss was associated with degeneration of the stria vascularis, spiral ganglion cells, and hair cells. This explains the difficulty of associating specific clinical symptoms or signs with specific anatomic locations, as pointed out by Suga and Lindsay and also by Nelson and Hinojosa. [5, 6, 7]
A large volume of current research is being conducted to determine the exact underlying cause of presbycusis. Much of the current research focuses on finding underlying genetic abnormalities that may cause, contribute to, or predispose to the development of this disease. [8]
One of the most widely investigated potential causes is a genetic mutation in mitochondrial DNA. [9] Reduced perfusion of the cochlea associated with age may contribute to the formation of reactive oxygen metabolites, which may adversely affect the inner ear neural structures as well as cause damage to mitochondrial DNA. Damaged mitochondrial DNA may cause reduced oxidative phosphorylation, which may lead to problems with neural functioning in the inner ear. A study by Dai et al also suggested that damaged mitochondrial DNA may lead to anatomic changes of the inner ear. [10] Specifically, they found more severe narrowing of the vaso nervorum in the internal auditory meatus in temporal bones with a mitochondrial DNA deletion. Damaged mitochondrial DNA has also been linked to a greater rate of apoptosis of certain cells in the inner ear in a study by Pickles. [11]
Two specific mitochondrial DNA deletions, mtDNA4834 and mtDNA4977, have been linked to age-related hearing loss in rodents. Additionally, studies by Han et al and Dai et al have linked the mtDNA4977 deletion with archived human temporal bones from patients with presbycusis. [12, 13]
Nutritional and anatomic causes of presbycusis have also been researched. Berner et al investigated the relation between vitamin B12 and folate deficiency with age-related hearing loss but did not find a statistically significant relationship. [14] Martin Villares et al did, however, find a positive relationship between high cholesterol levels and hearing loss. [15] However, Olzowy et al, in a randomized controlled trial, failed to show a difference in the rate of hearing loss in patients with presbycusis with the use of atorvastatin. [16] Although the degree of mastoid pneumatization did not correlate with the presence of presbycusis in a study by Pata et al, ultrastructural changes of the cuticular plate did appear to correlate with a known history of age related high-tone hearing loss in a human temporal bone study by Scholtz. [17, 18]
A study by Gao et al indicated that in persons with presbycusis, there is a lower concentration of gamma-aminobutyric acid+ (GABA+) in the auditory region of the brain than there is in persons with normal hearing. [19]
In general, the exact cause of age-related hearing loss is still not known today. However, promising research is currently underway in an effort to elucidate the etiology, whether it be genetic, anatomic, or a combination of factors.
Epidemiology
Frequency
United States
No accurate account of the incidence of presbycusis in the United States is available. Approximately 25-30% of people aged 65-74 years are estimated to have impaired hearing. For people aged 75 years and older, this incidence is thought to rise to 40-50%.
According to the 2014 National Health Interview Survey, 43.2% of American adults above age 70 years reported having hearing trouble, compared with 5.5% of adults aged 18-39 years and 19.0% of adults aged 40-69 years. [20, 21] It is estimated that by 2025, over 500 million individuals worldwide will suffer from clinically significant hearing impairment. [22]
International
The international incidence of presbycusis varies widely among societies. Westernized foreign countries and primitive civilizations have very different patterns of hearing loss. A 1962 study by Rosen and colleagues of a remote tribe of the Sudan called the Mabaans revealed significantly less hearing loss in the elderly population than in similarly aged people of urban societies. Whether this is because of the lack of chronic noise exposure or the paucity of other systemic ailments that are common in industrialized societies (eg, atherosclerosis, diabetes, reactive airway disease) is not known. In general, most of the world's population experiences some degree of decline in hearing with advancing age. [23]
Race
No known difference exists in prevalence of presbycusis based on race.
Sex
No difference in the prevalence of presbycusis between the sexes is found.
Age
By definition, prevalence of presbycusis increases with advancing age.
-
Inner ear.





